




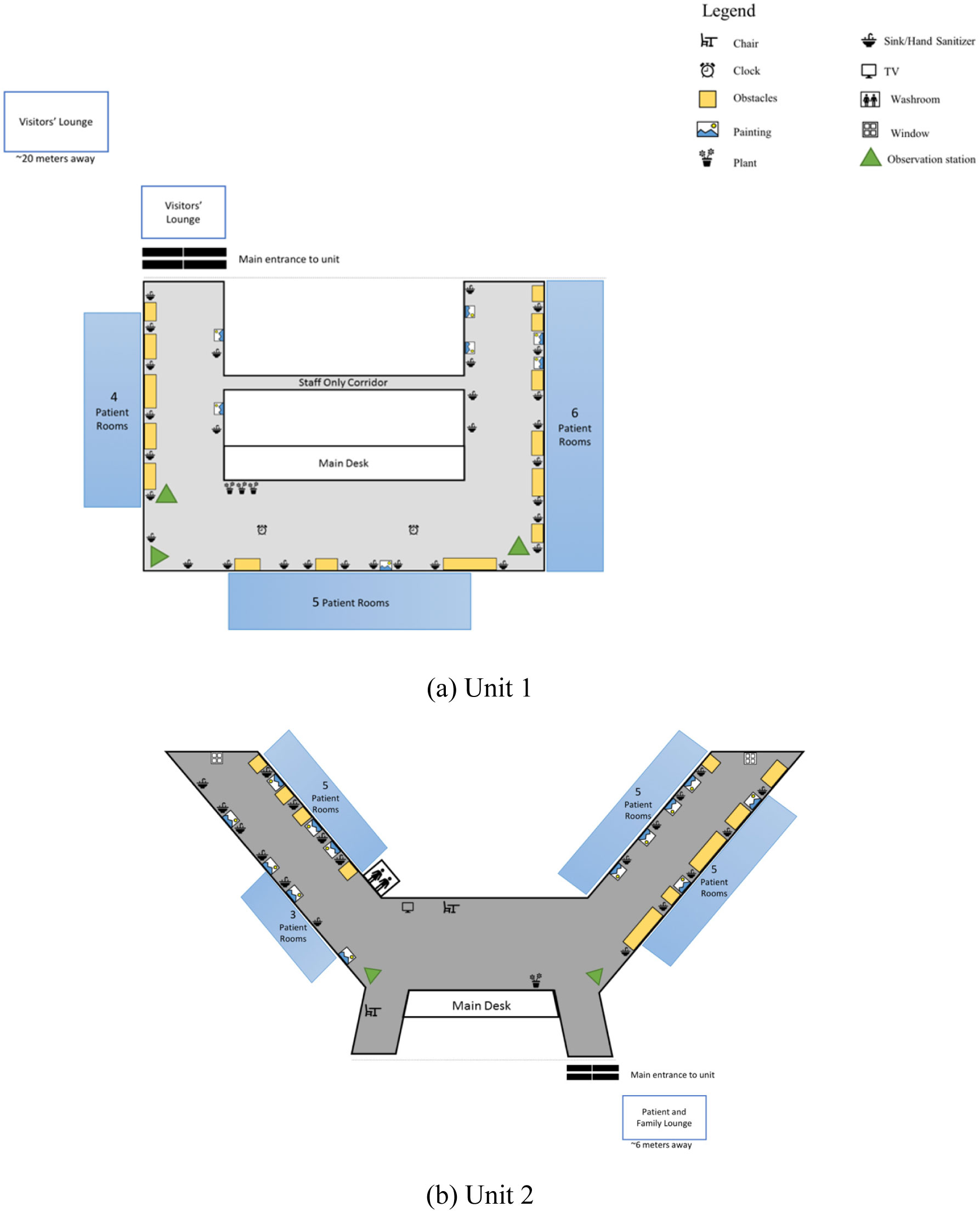
Figure 1.
Illustration of two hospital units with environmental features.
Citation: Patrocinio Ariza-Vega, Hattie Shu, Ruvini Amarasekera, Nicola Y. Edwards, Marta Filipski, Dolores Langford, Kenneth Madden, Maureen C. Ashe. Older adults’ activity on a geriatric hospital unit: A behavioral mapping study[J]. AIMS Medical Science, 2019, 6(1): 33-48. doi: 10.3934/medsci.2019.1.33
| [1] | Wendell C. Taylor, Kevin Rix, Ashley Gibson, Raheem J. Paxton . Sedentary behavior and health outcomes in older adults: A systematic review. AIMS Medical Science, 2020, 7(1): 10-39. doi: 10.3934/medsci.2020002 |
| [2] | Maureen C. Ashe, Khalil Merali, Nicola Edwards, Claire Schiller, Heather M. Hanson, Lena Fleig, Karim M. Khan, Wendy L. Cook, Heather A. McKay . Integrating research into clinical practice for hip fracture rehabilitation: Implementation of a pragmatic RCT. AIMS Medical Science, 2018, 5(2): 102-121. doi: 10.3934/medsci.2018.2.102 |
| [3] | John V. Rider, Shannon Martin, Erin Vieira . Do older adults take action to reduce fall risk after attending a community-based fall risk screening?. AIMS Medical Science, 2024, 11(4): 464-479. doi: 10.3934/medsci.2024032 |
| [4] | Sebastien FM Chastin, Juliet A Harvey, Philippa M Dall, Lianne McInally, Alexandra Mavroeidi, Dawn A Skelton . Beyond “#endpjparalysis”, tackling sedentary behaviour in health care. AIMS Medical Science, 2019, 6(1): 67-75. doi: 10.3934/medsci.2019.1.67 |
| [5] | XinQi Dong, Manrui Zhang . The Prevalence of Neurological Symptoms among Chinese Older Adults in the Greater Chicago Area. AIMS Medical Science, 2015, 2(1): 35-50. doi: 10.3934/medsci.2015.1.35 |
| [6] | Ray Marks . Narrative Review of Vitamin D and Its Specific Impact on Balance Capacity in Older Adults. AIMS Medical Science, 2016, 3(4): 345-358. doi: 10.3934/medsci.2016.4.345 |
| [7] | Alexandra Mavroeidi, Lianne McInally, Flavio Tomasella, Philippa M. Dall, Dawn A. Skelton . An explorative study of current strategies to reduce sedentary behaviour in hospital wards. AIMS Medical Science, 2019, 6(4): 285-295. doi: 10.3934/medsci.2019.4.285 |
| [8] | Ray Marks . Narrative Review of Dance-based Exercise and Its Specific Impact on Depressive Symptoms in Older Adults. AIMS Medical Science, 2016, 3(1): 61-76. doi: 10.3934/medsci.2016.1.61 |
| [9] | Ruijia Chen, XinQi Dong . The Prevalence and Correlates of Gambling Participation among Community-Dwelling Chinese Older Adults in the U.S.. AIMS Medical Science, 2015, 2(2): 90-103. doi: 10.3934/medsci.2015.2.90 |
| [10] | Christina L. Ekegren, Rachel E. Climie, William G. Veitch, Neville Owen, David W. Dunstan, Lara A. Kimmel, Belinda J. Gabbe . Sedentary behaviour and physical activity patterns in adults with traumatic limb fracture. AIMS Medical Science, 2019, 6(1): 1-12. doi: 10.3934/medsci.2019.1.1 |
Sedentary behavior with low levels of physical activity is ubiquitous in the hospital or rehabilitation setting [1]–[3]. Sedentary behavior includes activities of low energy expenditure occurring in a seated, lying or reclined position (e.g., sitting or watching television) [4],[5], while physical activity encompasses a wide range of energy-expending actions, such as activities of daily living, household tasks, work-related activity, or exercise [6]. These concepts are distinct and may impact health outcomes via different mechanisms [7]. While bed rest was traditionally prescribed for recovery, recent evidence demonstrates that prolonged periods of reduced movement may lead to several adverse health outcomes in older adults, such as substantial loss of muscle mass [8], and increased frailty [9],[10]. Alternatively, better health outcomes may be gained with early mobilization during recovery: Literature from intensive care and other hospital settings suggest that early mobilization may prevent muscle atrophy [11], improve future functional outcomes [11], and support falls prevention [12]. Equally important to early mobilization, is to consistently break up prolonged periods of daily sedentary behavior throughout the recovery period.
Several factors may contribute to high periods of sedentary time for patients [13]: Reduced access to resources, falls-risk liabilities, patient perspectives, low staff-patient ratios, and physical aspects of the hospital environment. In particular, the indoor (built) environment can promote or hinder physical activity. In a recent Australian study, there were no statistical differences in sedentary behavior for two groups of patients: adults recovering from a stroke or adults recovering from an acute myocardial infarction despite their different (potential) capacities [14]. This study suggests environmental factors (beyond person-level factors) may also contribute to behavior [14], and warrants further investigation.
There are several studies describing the hospital indoor environment and person-level activity using behavioral mapping, an environmental scanning method used to systematically record and compare behaviors across time and locations [15]. An advantage of behavioral mapping is the ability to detect a lower threshold of activity, which can sometimes be missed due to the known limitations with pedometers and accelerometers for people with slow walking (gait) speed [16]. Further, behavioral mapping can provide important contextual information for activity [17]. However, most current behavioral mapping studies are limited to inpatients with dementia [15],[17] or after stroke [18]–[23]. Few studies, if any, relate to older adults admitted to an acute care of the elderly (ACE) hospital unit [24],[25]. These ACE units were “developed to disrupt the [unavoidable] trajectory of functional decline of geriatric patients who are admitted to acute hospital wards.” [25] page 219.
The ACE unit incorporates five key components—patient-centered, frequent medical review, early rehabilitation, environment, and enhanced discharge planning—to minimize the risk of older adults' functional decline during an acute hospital admission [26],[27]. Although rehabilitation is key to mitigate limited activity due to an acute illness, one or two therapy sessions/day leaves ample opportunity for prolonged sitting (and possibly provides an opportunity to reverse the benefits of therapy). Specifically, despite the many positive attributes of an ACE unit, it is also important to recognize the need for breaking up prolonged sitting with periods of light activity over the day (if possible). Light physical activity (e.g., activities of daily living, household tasks) provides health benefits [28]–[32], and may be perceived as more attainable, especially for an older adult who is hospitalized. The indoor environment may support older adults to be active in general [33], via destination rooms and or clear hallways with handrails, and benches or chairs for rest stops, for example. We wanted to understand these factors in an already enriched hospital (ACE) unit for older adults.
Our aim was to describe the indoor environment of geriatric hospital units, and patients' and visitors' behavior. Specifically, we used an environmental scan and behavioral mapping to characterize two ACE units to describe the, physical, therapeutic, and social opportunities for older adult inpatient mobility outside their hospital rooms. This contextual knowledge was an essential first step to understand older patients' activity patterns in the acute care setting, and is a foundation to develop interventions to maximize mobility recovery in older adults admitted to hospital.
This was an observational inquiry of two inpatient units within a teaching hospital in Vancouver, Canada. We included two ACE units with patients (60 years and older). We also obtained minimal information on unit occupancy (number of patients, age and gender) during the data collection period. Please see Figure 1 for a visual description of both units. We documented the indoor environment and the behavior of patients and visitors (e.g., caregivers, friends, relatives). We used two data collection methods: First, we conducted an environmental scan to describe the indoor features and opportunities for movement in the unit, and second, we used behavioral mapping to describe the actions of people within unit environments during weekdays and weekends. We recognize the difference between gender and sex [34], however in this manuscript, we use gender-based terms, as we do not know the contribution of gender (“socially constructed roles”) or sex (biology) [34] for older adults' observed mobility whilst hospitalized. This study was approved by the university and hospital research ethics boards, and data were collected in September and October 2017.
We conducted an environmental scan of the two units to determine overall design and other key features that may (or may not) encourage physical activity. Specifically, we were interested in collecting information on environmental features that support or hinder safe physical activity, such as access to chairs, benches, and corridors with handrails [35], the color and texture of the floor material [36], noise and lighting [37],[38]. The same observer scanned each ward and recorded the environmental features, such as permanent structures (e.g., windows and bathrooms), and more transient items such as portable laundry carts. The observer recorded the information based on a checklist we created to assess the unit design, guided by the Evidence-Based Design conceptual framework [39]. In addition, the observer drew a map of each unit, and indicated the location of permanent and portable items.
Behavioral mapping is an observational research method to systematically record behavior within a specific environment [40]. We used standard methods [40] to observe activity every 15 minutes on each unit for two days (one week day/unit and one weekend/unit) from 8 am to 4 pm (except at 12 noon when we only recorded two sessions during lunch time). We specifically chose to look at weekend days as some hospitals generally have less therapy available on weekends. One trained observer, a combined-trained physiotherapist and occupational therapist, conducted the behavioral mapping over the four days. The observer moved in a predetermined pattern throughout each unit (in the public access areas only). Working with hospital staff, we identified two or three places on the unit (called “stations”), and one station in lounges, where the observer stopped for 5–10 seconds four times an hour for data collection. The identified lounges were immediately adjacent, but outside of the hospital units. During the observation period, the observer counted the number of patients and visitors (distinguished their role and posture/activity, and estimated the age and gender of patients) if they were in public areas of each unit (that is, the observer did not enter any rooms) to respect patient privacy. During the observation days, the observer also collected information on noise and lighting, because of the potential negative impact on patients' and staff's health and safety [37],[38].
We describe the units (based on the environmental scan of the indoor environment), use frequencies (and percentages) to record the sum of people and activity over each hour in two units, and differentiate between week days and weekend days. One trained research assistant entered data, and reviewed it on multiple occasions for accuracy. We created summary tables, and met with hospital staff to discuss and situate our findings within the context of the hospital unit (member checking). We used the actual number and gender of patients admitted to hospital units on the observational days as the denominator for some calculations. We used Chi square tests to explore associations for observed number of patients (based on the total number of patients admitted) and (i) women and men for overall observations, (ii) women and men for weekdays, and (iii) women and men for weekend days. We conservatively applied a Bonferroni correction to account for multiple testing (p = 0.05/three analyses), and considered p < 0.017 as significant. We used SPSS Version 23 (IBM, Armonk, New York) for data description and analyses.
We completed the environmental scan and behavioral mapping protocol as planned. Tables 1 and 2 provide an overview of the units' environment features. The units differed in their floorplans, number of beds (23 vs 28), and an additional visitor lounge in Unit 2. Both units had a number of obstacles along the corridors and few handrails; but they also had pictures, plants and furniture placed outside hospital rooms (Figure 1). Flooring material differed in their color and design: Unit 1 had light colored floor materials perceived to better distinguish between the floor and adjacent items. Overall, lighting was sufficient, and there were moderate to low levels of noise observed in both units throughout the day (Table 2).
During the data collection period there were 22 patients (Wednesday) and 23 patients (Saturday) admitted on Unit 1, and 28 patients admitted on both days (Thursday and Sunday) for Unit 2. In Tables 2 and 3, we provide a summary of patient and visitor observations. There was consistency between observed and actual patient numbers, gender and age groups, with only one patient misclassified as younger than their actual age. Sitting was noted in 61% of the patients' observations. There was an equal distribution of upright and sitting postures for three days; the exception was a weekend day with considerably more observed sitting. There were more observations in Unit 1, but more visitor observations in Unit 2 (94 vs 134), especially on the weekend.
Table 3 provides a detailed description of observations by unit. In Unit 1 (weekday), there were 42 observations from 19 patients: This included five patients (one woman and four men) who were observed more than once (four patients had five or less observations, and one patient > five observations). For this same unit on the weekend day (23 observations from 14 patients), there were three participants observed (two women and one man) more than once (one patient < five observations, and two patients > five observations). In Unit 2, there was only one patient (woman) observed twice on the weekday (14 observations from 13 patients). For this same unit on the weekend day (38 observations from 14 patients), there were three patients (one woman and two men) observed multiple times (one patient < five observations, and two patients > five observations). In sum, for the patients observed in the public areas of the units, 24% of the patients in Unit 1 had more than one observation, compared with just 15% of patients in Unit 2 (overall average 20%). For all admitted patients, 10% of women (5/48) and 13% of men (7/53) had multiple observations.
There were no significant associations for women's and men's overall observations (Chi square = 1.04, p = 0.31). However, men were more commonly observed outside their rooms on weekdays, and the reverse effect was recorded for women's observations on the weekends. Specifically, there were significant associations for gender and observations on weekdays (men > women; Chi square = 17.01, p < 0.0001), and weekend days (women > men; Chi square = 6.11, p = 0.013).
| Environmental feature | Unit 1 | Unit 2 |
| Physical description | Unit: Rectangle-shaped with three corridors with rooms; there were machines and other items (blood pressure machine, charts, linen, etc.) pushed up against the side of one wall for each corridor. There was one chair in the corridor. Lounge 1 (large): Rectangle-shaped room with a television, two sofas, two chairs, and a table. Lounge 2 (small): Square-shaped room with two sofas and a tableAiry, open concept design |
Unit: V-shaped unit with two long corridors and windows at each end; there were machines and other items (blood pressure machine, charts, linen, etc.), pushed up against the side of one wall for each corridor. Across from the nursing station desk there was a television, a table and two chairs, and a table with three chairs. Lounge: Rectangle-shaped room with television, books and bookcase, information pamphlets, five small tables, piano, and 11 chairs Older traditional hospital design, a bit darker lighting |
| Bathrooms | Two: Corridor and near lounge | Two: Corridor and near lounge |
| Destination rooms on unit | None, lounges adjacent unit | None, lounge adjacent unit |
| Dining room for patients | No | No |
| Family support features (e.g., lounge, access to washrooms) | Two lounges (large and small) and access to bathroom | Large lounge with plants and a piano, and access to bathroom |
| Flooring type | Linoleum, light color and easy to distinguish objects | Linoleum, dark speckled flooring |
| Gardens and plants | Three plants in the corridor, garden visible outside | One plant on the desk, and six in the lounge; outside green space visible |
| Handrails | Not on unit or lounge | In corridors, but not in the lounge |
| Items on walls or ceilings | Paintings in corridors and lounge, a lot of messaging on the walls about patient care and hand washing | Paintings in corridors and lounge, a lot of messaging on the walls about patient care and hand washing |
| Televisions | Lounge only | Corridors and lounge |
| Temperature | Good in the corridor but lower in the lounge | Good in the corridor but lower in the lounge |
| Wayfinding | Signage available for reception, bathrooms, hand washing sinks and sanitizers, but not for consumer services, stairs or elevators | Signage available for reception, bathrooms and hand sanitizers, but not for hand washing sinks, consumer services, stairs or elevators |
| Windows | Windows only in lounge with views of parking, trees and street | Windows at the end of each corridor and in lounge with views of parking, trees and street |
 DownLoad:
CSV
DownLoad:
CSV
| Unit 1 | Unit 2 | ||||||||
| Observations | Observations | ||||||||
| Time | Noise | Light | Visitor | Patient | Noise | Light | Visitor | Patient | |
| WEEKDAY | 8:00 | 2 | 1 | 1 | 5 | 2 | 1 | 5 | 0 |
| 9:00 | 3 | 1 | 0 | 6 | 3 | 1 | 3 | 1 | |
| 10:00 | 3 | 1 | 11 | 7 | 2 | 1 | 3 | 2 | |
| 11:00 | 3 | 1 | 15 | 7 | 3 | 1 | 11 | 3 | |
| 12:00 | 5 | 1 | 8 | 2 | 3 | 1 | 5 | 2 | |
| 13:00 | 3 | 1 | 8 | 5 | 3 | 1 | 8 | 4 | |
| 14:00 | 3 | 1 | 3 | 4 | 2 | 1 | 6 | 1 | |
| 15:00 | 3 | 1 | 2 | 5 | 3 | 1 | 18 | 1 | |
| 16:00 | 2 | 1 | 0 | 1 | 4 | 1 | 4 | 0 | |
| Total observations | 48 | 42 | 63 | 14 | |||||
| Observations | Observations | ||||||||
| Time | Noise | Light | Visitor | Patient | Noise | Light | Visitor | Patient | |
| WEEKEND | 8:00 | 2 | 1 | 0 | 6 | 2 | 2 | 5 | 0 |
| 9:00 | 2 | 1 | 4 | 5 | 4 | 2 | 7 | 3 | |
| 10:00 | 2 | 1 | 5 | 3 | 3 | 1 | 9 | 11 | |
| 11:00 | 4 | 1 | 15 | 3 | 4 | 1 | 9 | 8 | |
| 12:00 | 2 | 1 | 1 | 0 | 3 | 1 | 6 | 4 | |
| 13:00 | 2 | 1 | 0 | 0 | 2 | 1 | 22 | 6 | |
| 14:00 | 2 | 1 | 8 | 5 | 2 | 1 | 6 | 2 | |
| 15:00 | 2 | 1 | 11 | 1 | 2 | 2 | 7 | 3 | |
| 16:00 | 2 | 1 | 2 | 0 | 3 | 2 | 0 | 1 | |
| Total observations | 46 | 23 | 71 | 38 | |||||
DownLoad:
CSV
| Day 1 (Wednesday) | Day 3 (Saturday) | Day 2 (Thursday) | Day 4 (Sunday) | |
| Unit 1 | Unit 1 | Unit 2 | Unit 2 | |
| Number of observations/day | 42 | 23 | 14 | 38 |
| Upright | 22 | 11 | 7 | 6 |
| Sitting | 20 | 12 | 7 | 32 |
| Patients admitted on unit | 22 | 23 | 28 | 28 |
| Women | 9 | 10 | 16 | 13 |
| Men | 13 | 13 | 12 | 15 |
| Age < 65 years | 2 | 3 | 2 | 1 |
| Age > 65 years | 20 | 20 | 26 | 27 |
| Patients observed on unit | 19 (86%) | 14 (61%) | 13 (46%) | 14 (50%) |
| Women | 6 (67%) | 10 (100%) | 3 (19%) | 7 (54%) |
| Men | 13 (100%) | 4 (31%) | 10 (83%) | 7 (47%) |
| Age < 65 years | 3 | 1 | 0 | 0 |
| Age > 65 years | 16 | 13 | 13 | 14 |
DownLoad:
CSV
Sedentary behaviors, such as prolonged sitting, lying or reclining, use very little energy expenditure [4],[5], and are ever-present throughout the hospital phase and subsequent recovery period [1],[2]. Studies indicate hospitalization can lead to the development of disability and loss of autonomy [41], and may mediate a change in residence upon discharge. Here, we describe the indoor environment for two ACE units with features that encourage more activity such as, low to moderate noise levels, adequate lighting, good esthetics (windows, pictures and plants), hallways for walking with rest stops (chairs), and destination rooms (visitor lounges). However, few handrails and the presence of items against walls in the hallways (perceived obstacles) were potential barriers to patients' mobility outside their rooms. Based on the behavioral mapping exercise, we observed about 60% of patients admitted to the ACE units left their room on at least one occasion, with 20% of patients with multiple observations. Sitting was noted in more than half of the observations. However, we recognize that patients may have engaged in routine rehabilitation (in their room or therapy department). Our work extends the literature to highlight an interesting finding related to gender and activity patterns. We observed significantly more older men outside their rooms during weekdays, and more older women outside their rooms on the weekend days: Concurrently, we recorded more visitor observations on the weekend. To our knowledge, our study is the first to observe activity patterns (using behavioral mapping) on an ACE unit, thus it is difficult to put our results into perspective. That is, older adults admitted to an ACE unit are generally considered frail, thus observing more than half of patients in the public areas of the units is encouraging. A laudable goal is to optimize physical activity for all older adults in the acute hospital setting, to avoid the cycle of prolonged sedentary behavior that can be difficult to change once discharged home. Therefore, these results serve as a baseline, and generate hypotheses for future testing to optimize the hospital experience for older adults.
The exploratory work presented here is an important first step to work collaboratively with key stakeholders. Behavioral mapping is a unique approach to provide contextual information on patients' mobility in the hospital setting. As there are few, if any, studies using behavioral mapping conducted within ACE units, we do not know if more patient observations lead to better health outcomes. However, other studies underscore that early [42]–[44] (and frequent) daily movement can be beneficial. The approach presented here provides a person-centered way to develop and test interventions to encourage safe mobility on the hospital unit and circumvent the post-hospital syndrome, a multifactorial phenomenon negatively impacting health and recovery [45]. As aptly stated by Professor Krumholz, “The hospitalization should not only address the urgencies of the acute illness, but also seek to promote health actively by strengthening patients and contributing to their physiological reserve.” [45] page 3. Hospital policies are generally developed for the health and safety of patients and staff. Although there has been a recent call to re-evaluate patients' activity in hospital vs. the risk of falls [13], there is an urgent need for solutions that promote mobility while minimizing harm. This is an important goal that would benefit from further clarification with empirical evidence.
Early mobilization is essential, however it is equally important to balance activity with restorative breaks, and develop skills, strategies and confidence with new or evolving mobility and health status. Technology advances could assist this change in focus by providing staff with real-time monitoring of patients' daily movement patterns [46]. Reduced self-efficacy (resulting from hospitalization) and or an increased fear of falling [47],[48] may result in older adults' hesitancy to mobilize. Support for activity and developing good health habits could begin through modeling within the hospital setting, while patients are still supervised by health care staff. It does not seem to be enough to “tell” people to be active once they are home. This can be an opportunity to develop positive health habits for longer term adoption outside of the hospital setting. Ultimately, the hospital experience is a complex, multi-dimensional issue that we need to better understand from different perspectives: Patients' families, hospital staff and policy makers. This comprehensive approach with a person-centered lens is ideal to develop and test possible solutions to minimize the risk for iatrogenic development of mobility disability and support in-hospital harm reduction.
We noted an interesting finding in our study: Older men were observed more in the unit during the weekdays and older women during the weekends. We do not know why this may have occurred but speculate that it may be a result of gender-based behaviors, the presence of family members (visitors), or by chance. It is possible that older men took a more traditional approach to the hospital admission and “worked” on their recovery during the weekdays: Older men (compared with older women) generally engage in more higher intensity physical activity [49]. Alternatively, maybe older men engaged in steps to gain back some control [50] (through exercise) when confronted with an acute hospital admission. Interestingly, based on our previous work at the same hospital, we noted there were more men who fell, compared with women [51] during a hospital admission: we do not know why they fell, but it is possible that older men may be at greater exposure for falls due to walking outside hospital rooms. There is other literature with similar observations for men in hospital [52],[53]. Conversely, there were slightly more visitors observed on the weekend, which may have encouraged women to leave their rooms. In a similar study by Prakash and colleagues [54], they noted that patients with stroke were more active (in hospital) when family was present, although there were no gender differences reported. We stopped data collection at 4 pm, so do not know whether visitors, such as family members, may have supported older women to leave their rooms on weekday evenings. These preliminary data generate hypothesis for future studies to disentangle the role of gender (if any) in the recovery period.
To address the current state of prolonged sedentary behavior in the hospital setting requires understanding factors at multiple levels: person, practitioner, policy and environment. The built environment is emerging as a key factor to support older adults' outdoor physical activity [55],[56], but, in general, less is known about older adults' physical activity and the indoor (home) setting [33]. Similar principles may apply to hospital settings, thus we used a framework to guide our research [39] and conducted an environmental scan of the hospital units. We noted several challenges within units which may account for patients' reduced activity. For example, handrails were missing on Unit 1, and for both units there were obstacles in the hallways, and no destination rooms within the unit (e.g., central dining room, small gym). In addition, we observed fewer patients in Unit 2; here the floor plan was more traditional, and flooring was darker (and possibly creating obstacles for older patients with low vision). These features may or may not have contributed to our findings, and it remains uncertain as there are no publications on barriers to activity in ACE units. Activity is most likely influenced by the interaction of the person within the physical and social environment. Within the stroke literature, Rosbergen and colleagues explored the effect of an “enriched environment” on activity for older adults with stroke [57]–[59]. In this controlled pre-post pilot study, they noted an increase in patients' activity, with no significant difference in adverse events compared with a control group [58]. This study is informative to guide future interventions for patients, staff, and hospital culture and policies.
We acknowledge the following limitations with this study. First, we only collected data in the public areas of the hospital units and are not able to account for activity participants engaged in within their room, or areas of the hospital outside of the unit. In particular, some ACE units have cycle ergometers for use in patient rooms. Second, we only collected data during the day for a few days, and cannot comment on any physical activity during the evenings. Nonetheless, we have detailed observations of patients' daily routines outside their rooms and can provide context to their patterns. Third, we observed low numbers of participants, and this may or may not represent typical behavior for older patients admitted to ACE units. Further, we do not have information on the health status of the patients on each unit, thus these factors could explain the observations (or lack thereof). We also did not use a direct measurement (e.g., accelerometry) of patients' activity patterns. However, given the low level of patients' observed physical activity, there is the possibility of missing data (due to slow gait speed) with accelerometry [60]. Conversely, in this study, an experienced physiotherapist-occupational therapist collected all data reducing the risk of missed activity. Finally, we do not know if the observed behaviors in hospital were associated with health outcomes post-discharge, but collectively, this valuable information is hypothesis-generating for our next research phase.
In conclusion, we describe the indoor environment for two ACE units, with features that can encourage mobility, but also noted potential barriers, such as few handrails, and obstacles in the hallways. We also describe older adults' physical activity patterns in the acute hospital units during a recent admission. We noted variability in observations (based on day and unit) for patients outside of their rooms, and sitting was observed over half of the time. Emerging evidence supports early activity, but to date, many older adults engage in prolonged periods of sedentary behavior as a hospital inpatient. A recent international consensus on older adults and sedentary behavior [61] includes a recommendation for more research to reduce prolonged sitting during hospitalization. Our exploratory data is a beginning to advance the field and supports our next phase, the co-creation of safe and person-centered policies on inpatient mobilization.
| [1] |
Zusman EZ, Dawes MG, Edwards N, et al. (2018) A systematic review of evidence for older adults' sedentary behavior and physical activity after hip fracture. Clin Rehabil 32: 679–691. doi: 10.1177/0269215517741665

|
| [2] |
Ekegren CL, Beck B, Climie RE, et al. (2018) Physical activity and sedentary behavior subsequent to serious orthopedic injury: A systematic review. Arch Phys Med Rehabil 99: 164–177. doi: 10.1016/j.apmr.2017.05.014
|
| [3] |
Ostir GV, Berges IM, Kuo YF, et al. (2013) Mobility activity and its value as a prognostic indicator of survival in hospitalized older adults. J Am Geriatr Soc 61: 551–557. doi: 10.1111/jgs.12170
|
| [4] |
Barnes J, Behrens TK, Benden ME (2012) Letter to the editor: Standardized use of the terms "sedentary" and "sedentary behaviours". Appl Physiol Nutr Metab 37: 540–542. doi: 10.1139/h2012-024
|
| [5] |
Tremblay MS, Aubert S, Barnes JD, et al. (2017) Sedentary behavior research network (SBRN)-terminology consensus project process and outcome. Int J Behav Nutr Phys Act 14: 75. doi: 10.1186/s12966-017-0525-8
|
| [6] | Caspersen CJ, Powell KE, Christenson GM (1985) Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep 100: 126–131. |
| [7] | Hamilton MT, Hamilton DG, Zderic TW (2004) Exercise physiology versus inactivity physiology: An essential concept for understanding lipoprotein lipase regulation. Exerc Sport Sci Rev 32: 161–166. |
| [8] |
Stevens-Lapsley JE, Loyd BJ, Falvey JR, et al. (2016) Progressive multi-component home-based physical therapy for deconditioned older adults following acute hospitalization: A pilot randomized controlled trial. Clin Rehabil 30: 776–785. doi: 10.1177/0269215515603219
|
| [9] | Gill TM, Gahbauer EA, Han L, et al. (2011) The relationship between intervening hospitalizations and transitions between frailty states. J Gerontol A-Biol 66: 1238–1243. |
| [10] |
Lim SER, Dodds R, Bacon D, et al. (2018) Physical activity among hospitalised older people: Insights from upper and lower limb accelerometry. Aging Clin Exp Res 30: 1363–1369. doi: 10.1007/s40520-018-0930-0
|
| [11] |
Grimandi R, Paupy H, Prot H, et al. (2015) Early Mobilization in ICU: About New Strategies in Physiotherapy's Care. Crit Care Med 43: e400. doi: 10.1097/CCM.0000000000001073
|
| [12] |
Talkowski JB, Lenze EJ, Munin MC, et al. (2009) Patient participation and physical activity during rehabilitation and future functional outcomes in patients after hip fracture. Arch Phys Med Rehabil 90: 618–622. doi: 10.1016/j.apmr.2008.10.024
|
| [13] |
Growdon ME, Shorr RI, Inouye SK (2017) The tension between promoting mobility and preventing falls in the hospital. JAMA Intern Med 177: 759–760. doi: 10.1001/jamainternmed.2017.0840
|
| [14] | Lay S, Bernhardt J, West T, et al. (2016) Is early rehabilitation a myth? Physical inactivity in the first week after myocardial infarction and stroke. Disabil Rehabil 38: 1493–1499. |
| [15] |
Bell PA, Smith JM (1997) A behavior mapping method for assessing efficacy of change on special care units. Am J Alzheimer's Dis 12: 184–189. doi: 10.1177/153331759701200407
|
| [16] | Storti KL, Pettee KK, Brach JS, et al. (2008) Gait speed and step-count monitor accuracy in community-dwelling older adults. Med Sci Sport Exer 40: 59–64. |
| [17] |
Milke DL, Beck CH, Danes S, et al. (2009) Behavioral mapping of residents' activity in five residential style care centers for elderly persons diagnosed with dementia: Small differences in sites can affect behaviors. J Hous Elderly 23: 335–367. doi: 10.1080/02763890903327135
|
| [18] |
Gustafsson L, McKenna K (2010) Is there a role for meaningful activity in stroke rehabilitation? Top Stroke Rehabil 17: 108–118. doi: 10.1310/tsr1702-108
|
| [19] |
Gustafsson L, Nugent N, Biros L (2012) Occupational therapy practice in hospital-based stroke rehabilitation? Scand J Occup Ther 19: 132–139. doi: 10.3109/11038128.2011.562915
|
| [20] |
Janssen H, Ada L, Karayanidis F, et al. (2012) Translating the use of an enriched environment poststroke from bench to bedside: Study design and protocol used to test the feasibility of environmental enrichment on stroke patients in rehabilitation. Int J Stroke 7: 521–526. doi: 10.1111/j.1747-4949.2011.00727.x
|
| [21] | Sjoholm A, Skarin M, Churilov L, et al. (2014) Sedentary behaviour and physical activity of people with stroke in rehabilitation hospitals. Stroke Res Treat 2014: 591897. |
| [22] |
Skarin M, Sjoholm A, Nilsson A, et al. (2013) A mapping study on physical activity in stroke rehabilitation: Establishing the baseline. J Rehabil Med 45: 997–1003. doi: 10.2340/16501977-1214
|
| [23] | West T, Bernhardt J (2012) Physical activity in hospitalised stroke patients. Stroke Res Treat 2012: 13. |
| [24] |
Jayadevappa R, Bloom BS, Raziano DB, et al. (2003) Dissemination and characteristics of acute care for elders (ACE) units in the United States. Int J Technol Assess Health Care 19: 220–227. doi: 10.1017/S0266462303000205
|
| [25] |
Ahmed NN, Pearce SE (2010) Acute care for the elderly: A literature review. Popul Health Manag 13: 219–225. doi: 10.1089/pop.2009.0058
|
| [26] | Lai L, Wong R (2017) Leading best practice: Acute Care for Elders Units (ACE)-evidence and keys to successful operation. Can Geriatr J CME 7: 1–9. |
| [27] | Wong R, Shaw M, Acton C (2003) Geriatrics today: An interdisciplinary approach to optimize health services in a specialized acute care for elders unit. J Can Geriatr Soc 6: 177–186. |
| [28] |
Amagasa S, Machida M, Fukushima N, et al. (2018) Is objectively measured light-intensity physical activity associated with health outcomes after adjustment for moderate-to-vigorous physical activity in adults? A systematic review. Int J Behav Nutr Phys Act 15: 65. doi: 10.1186/s12966-018-0695-z
|
| [29] | Chastin SFM, De Craemer M, De Cocker K, et al. (2018) How does light-intensity physical activity associate with adult cardiometabolic health and mortality? Systematic review with meta-analysis of experimental and observational studies. Br J Sports Med bjsports-2017. |
| [30] |
Fuzeki E, Engeroff T, Banzer W (2017) Health benefits of light-intensity physical activity: A systematic review of accelerometer data of the national health and nutrition examination survey (NHANES). Sport Med 47: 1769–1793. doi: 10.1007/s40279-017-0724-0
|
| [31] | Saint-Maurice PF, Troiano RP, Berrigan D, et al. (2018) Volume of Light Versus Moderate-to-Vigorous Physical Activity: Similar Benefits for All-Cause Mortality? J Am Heart Assoc 7: e008815. |
| [32] |
Piercy KL, Troiano RP, Ballard RM, et al. (2018) The physical activity guidelines for Americans. JAMA 320: 2020–2028. doi: 10.1001/jama.2018.14854
|
| [33] | Ashe MC (2018) Indoor Environments and Promoting Physical Activity Among Older People, In: The Palgrave Handbook of Ageing and Physical Activity Promotion, Springer, 467–483. |
| [34] | McGregor AJ, Choo EK, Becker BM, et al. (2016) Sex and gender in acute care medicine. Online resource, 1. |
| [35] |
Lu Z (2010) Investigating walking environments in and around assisted living facilities: A facility visit study. HERD 3: 58–74. doi: 10.1177/193758671000300406
|
| [36] |
Harris DD (2015) The influence of flooring on environmental stressors: A study of three flooring materials in a hospital. HERD 8: 9–29. doi: 10.1177/1937586715573730
|
| [37] |
Kamdar BB, Martin JL, Needham DM (2017) Noise and Light Pollution in the Hospital: A Call for Action. J Hosp Med 12: 861–862. doi: 10.12788/jhm.2838
|
| [38] | Xyrichis A, Wynne J, Mackrill J, et al. (2018) Noise pollution in hospitals. BMJ 363: k4808. |
| [39] |
Ulrich RS, Berry LL, Quan X, et al. (2010) A conceptual framework for the domain of evidence-based design. HERD 4: 95–114. doi: 10.1177/193758671000400107
|
| [40] | Ng C (2016) Behavioral mapping and tracking, In: Gifford R (editor.), Research methods for environmental psychology, West Sussex, UK: John Wiley & Sons, ltd, 26–52. |
| [41] |
Lang PO, Meyer N, Heitz D, et al. (2007) Loss of independence in Katz's ADL ability in connection with an acute hospitalization: Early clinical markers in French older people. Eur J Epidemiol 22: 621–630. doi: 10.1007/s10654-007-9150-1
|
| [42] |
Siu AL, Penrod JD, Boockvar KS, et al. (2006) Early ambulation after hip fracture: Effects on function and mortality. Arch Intern Med 166: 766–771. doi: 10.1001/archinte.166.7.766
|
| [43] |
Goldfarb M, Afilalo J, Chan A, et al. (2018) Early mobility in frail and non-frail older adults admitted to the cardiovascular intensive care unit. J Crit Care 47: 9–14. doi: 10.1016/j.jcrc.2018.05.013
|
| [44] |
Morri M, Forni C, Marchioni M, et al. (2018) Which factors are independent predictors of early recovery of mobility in the older adults' population after hip fracture? A cohort prognostic study. Arch Orthop Traum Su 138: 35–41. doi: 10.1007/s00402-017-2803-y
|
| [45] |
Krumholz HM (2013) Post-hospital syndrome-an acquired, transient condition of generalized risk. N Engl J Med 368: 100–102. doi: 10.1056/NEJMp1212324
|
| [46] |
Pannurat N, Thiemjarus S, Nantajeewarawat E (2014) Automatic fall monitoring: A review. Sensors 14: 12900–12936. doi: 10.3390/s140712900
|
| [47] |
Gettens S, Fulbrook P (2015) Fear of falling: Association between the Modified Falls Efficacy Scale, in-hospital falls and hospital length of stay. J Eval Clin Pract 21: 43–50. doi: 10.1111/jep.12226
|
| [48] |
Schmid AA, Acuff M, Doster K, et al. (2009) Poststroke fear of falling in the hospital setting. Top Stroke Rehabil 16: 357–366. doi: 10.1310/tsr1605-357
|
| [49] | Colley RC, Garriguet D, Janssen I, et al. (2011) Physical activity of Canadian adults: Accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep 22: 7–14. |
| [50] |
Winnett R, Furman R, Enterline M (2012) Men at risk: Considering masculinity during hospital-based social work intervention. Soc Work Health Care 51: 312–326. doi: 10.1080/00981389.2011.650843
|
| [51] |
Dunne TJ, Gaboury I, Ashe MC (2014) Falls in hospital increase length of stay regardless of degree of harm. J Eval Clin Pract 20: 396–400. doi: 10.1111/jep.12144
|
| [52] |
Babine RL, Hyrkas KE, Bachand DA, et al. (2016) Falls in A Tertiary Care Hospital-Association With Delirium: A Replication Study. Psychosomatics 57: 273–282. doi: 10.1016/j.psym.2016.01.003
|
| [53] |
Chen X, Van Nguyen H, Shen Q, et al. (2011) Characteristics associated with recurrent falls among the elderly within aged-care wards in a tertiary hospital: The effect of cognitive impairment. Arch Gerontol Geriat 53: e183–e186. doi: 10.1016/j.archger.2010.08.012
|
| [54] |
Prakash V, Shah MA, Hariohm K (2016) Family's presence associated with increased physical activity in patients with acute stroke: an observational study. Braz J Phys Ther 20: 306–311. doi: 10.1590/bjpt-rbf.2014.0172
|
| [55] | Tuckett AG, Banchoff AW, Winter SJ, et al. (2018) The built environment and older adults: A literature review and an applied approach to engaging older adults in built environment improvements for health. Int J Older People Nurs, 13. |
| [56] | Rosso AL, Auchincloss AH, Michael YL (2011) The urban built environment and mobility in older adults: A comprehensive review. J Aging Res 2011: 816106. |
| [57] |
Rosbergen IC, Grimley RS, Hayward KS, et al. (2016) The effect of an enriched environment on activity levels in people with stroke in an acute stroke unit: Protocol for a before-after pilot study. Pilot Feasibility Stud 2: 36. doi: 10.1186/s40814-016-0081-z
|
| [58] |
Rosbergen IC, Grimley RS, Hayward KS, et al. (2017) Embedding an enriched environment in an acute stroke unit increases activity in people with stroke: A controlled before-after pilot study. Clin Rehabil 31: 1516–1528. doi: 10.1177/0269215517705181
|
| [59] |
Rosbergen ICM, Brauer SG, Fitzhenry S, et al. (2017) Qualitative investigation of the perceptions and experiences of nursing and allied health professionals involved in the implementation of an enriched environment in an Australian acute stroke unit. BMJ Open 7: e018226. doi: 10.1136/bmjopen-2017-018226
|
| [60] |
Phillips LJ, Petroski GF, Markis NE (2015) A comparison of accelerometer accuracy in older adults. Res Gerontol Nurs 8: 213–219. doi: 10.3928/19404921-20150429-03
|
| [61] |
Dogra S, Ashe MC, Biddle SJH, et al. (2017) Sedentary time in older men and women: An international consensus statement and research priorities. Br J Sports Med 51: 1526–1532. doi: 10.1136/bjsports-2016-097209
|
| 1. | Ruby Lipson-Smith, Rebecca McLaughlan, Mapping Healthcare Spaces: A Systematic Scoping Review of Spatial and Behavioral Observation Methods, 2022, 15, 1937-5867, 351, 10.1177/19375867221089702 | |
| 2. | Christina L Ekegren, Anne M Mather, Sandra Reeder, Lara Kimmel, Maureen C Ashe, Belinda J Gabbe, Can a new ward environment and intensive allied health staffing model enhance therapeutic opportunities in trauma care? A behavioural mapping study of patients’ activities and interactions, 2022, 36, 0269-2155, 1314, 10.1177/02692155221107739 | |
| 3. | Laura Jolliffe, Taya A Collyer, Ka Hei Sun, Lisa Done, Siobhan Barber, Michele L Callisaya, David A Snowdon, Geriatric evaluation and management inpatients spend little time participating in physically, cognitively or socially meaningful activity: a time–motion analysis, 2025, 54, 0002-0729, 10.1093/ageing/afaf043 |
Figures(1) / Tables(3)

Patrocinio Ariza-Vega, Hattie Shu, Ruvini Amarasekera, Nicola Y. Edwards, Marta Filipski, Dolores Langford, Kenneth Madden, Maureen C. Ashe. Older adults’ activity on a geriatric hospital unit: A behavioral mapping study[J]. AIMS Medical Science, 2019, 6(1): 33-48. doi: 10.3934/medsci.2019.1.33

| Environmental feature | Unit 1 | Unit 2 |
| Physical description | Unit: Rectangle-shaped with three corridors with rooms; there were machines and other items (blood pressure machine, charts, linen, etc.) pushed up against the side of one wall for each corridor. There was one chair in the corridor. Lounge 1 (large): Rectangle-shaped room with a television, two sofas, two chairs, and a table. Lounge 2 (small): Square-shaped room with two sofas and a tableAiry, open concept design |
Unit: V-shaped unit with two long corridors and windows at each end; there were machines and other items (blood pressure machine, charts, linen, etc.), pushed up against the side of one wall for each corridor. Across from the nursing station desk there was a television, a table and two chairs, and a table with three chairs. Lounge: Rectangle-shaped room with television, books and bookcase, information pamphlets, five small tables, piano, and 11 chairs Older traditional hospital design, a bit darker lighting |
| Bathrooms | Two: Corridor and near lounge | Two: Corridor and near lounge |
| Destination rooms on unit | None, lounges adjacent unit | None, lounge adjacent unit |
| Dining room for patients | No | No |
| Family support features (e.g., lounge, access to washrooms) | Two lounges (large and small) and access to bathroom | Large lounge with plants and a piano, and access to bathroom |
| Flooring type | Linoleum, light color and easy to distinguish objects | Linoleum, dark speckled flooring |
| Gardens and plants | Three plants in the corridor, garden visible outside | One plant on the desk, and six in the lounge; outside green space visible |
| Handrails | Not on unit or lounge | In corridors, but not in the lounge |
| Items on walls or ceilings | Paintings in corridors and lounge, a lot of messaging on the walls about patient care and hand washing | Paintings in corridors and lounge, a lot of messaging on the walls about patient care and hand washing |
| Televisions | Lounge only | Corridors and lounge |
| Temperature | Good in the corridor but lower in the lounge | Good in the corridor but lower in the lounge |
| Wayfinding | Signage available for reception, bathrooms, hand washing sinks and sanitizers, but not for consumer services, stairs or elevators | Signage available for reception, bathrooms and hand sanitizers, but not for hand washing sinks, consumer services, stairs or elevators |
| Windows | Windows only in lounge with views of parking, trees and street | Windows at the end of each corridor and in lounge with views of parking, trees and street |
DownLoad:
CSV
| Unit 1 | Unit 2 | ||||||||
| Observations | Observations | ||||||||
| Time | Noise | Light | Visitor | Patient | Noise | Light | Visitor | Patient | |
| WEEKDAY | 8:00 | 2 | 1 | 1 | 5 | 2 | 1 | 5 | 0 |
| 9:00 | 3 | 1 | 0 | 6 | 3 | 1 | 3 | 1 | |
| 10:00 | 3 | 1 | 11 | 7 | 2 | 1 | 3 | 2 | |
| 11:00 | 3 | 1 | 15 | 7 | 3 | 1 | 11 | 3 | |
| 12:00 | 5 | 1 | 8 | 2 | 3 | 1 | 5 | 2 | |
| 13:00 | 3 | 1 | 8 | 5 | 3 | 1 | 8 | 4 | |
| 14:00 | 3 | 1 | 3 | 4 | 2 | 1 | 6 | 1 | |
| 15:00 | 3 | 1 | 2 | 5 | 3 | 1 | 18 | 1 | |
| 16:00 | 2 | 1 | 0 | 1 | 4 | 1 | 4 | 0 | |
| Total observations | 48 | 42 | 63 | 14 | |||||
| Observations | Observations | ||||||||
| Time | Noise | Light | Visitor | Patient | Noise | Light | Visitor | Patient | |
| WEEKEND | 8:00 | 2 | 1 | 0 | 6 | 2 | 2 | 5 | 0 |
| 9:00 | 2 | 1 | 4 | 5 | 4 | 2 | 7 | 3 | |
| 10:00 | 2 | 1 | 5 | 3 | 3 | 1 | 9 | 11 | |
| 11:00 | 4 | 1 | 15 | 3 | 4 | 1 | 9 | 8 | |
| 12:00 | 2 | 1 | 1 | 0 | 3 | 1 | 6 | 4 | |
| 13:00 | 2 | 1 | 0 | 0 | 2 | 1 | 22 | 6 | |
| 14:00 | 2 | 1 | 8 | 5 | 2 | 1 | 6 | 2 | |
| 15:00 | 2 | 1 | 11 | 1 | 2 | 2 | 7 | 3 | |
| 16:00 | 2 | 1 | 2 | 0 | 3 | 2 | 0 | 1 | |
| Total observations | 46 | 23 | 71 | 38 | |||||
DownLoad:
CSV
| Day 1 (Wednesday) | Day 3 (Saturday) | Day 2 (Thursday) | Day 4 (Sunday) | |
| Unit 1 | Unit 1 | Unit 2 | Unit 2 | |
| Number of observations/day | 42 | 23 | 14 | 38 |
| Upright | 22 | 11 | 7 | 6 |
| Sitting | 20 | 12 | 7 | 32 |
| Patients admitted on unit | 22 | 23 | 28 | 28 |
| Women | 9 | 10 | 16 | 13 |
| Men | 13 | 13 | 12 | 15 |
| Age < 65 years | 2 | 3 | 2 | 1 |
| Age > 65 years | 20 | 20 | 26 | 27 |
| Patients observed on unit | 19 (86%) | 14 (61%) | 13 (46%) | 14 (50%) |
| Women | 6 (67%) | 10 (100%) | 3 (19%) | 7 (54%) |
| Men | 13 (100%) | 4 (31%) | 10 (83%) | 7 (47%) |
| Age < 65 years | 3 | 1 | 0 | 0 |
| Age > 65 years | 16 | 13 | 13 | 14 |
DownLoad:
CSV
| Environmental feature | Unit 1 | Unit 2 |
| Physical description | Unit: Rectangle-shaped with three corridors with rooms; there were machines and other items (blood pressure machine, charts, linen, etc.) pushed up against the side of one wall for each corridor. There was one chair in the corridor. Lounge 1 (large): Rectangle-shaped room with a television, two sofas, two chairs, and a table. Lounge 2 (small): Square-shaped room with two sofas and a tableAiry, open concept design |
Unit: V-shaped unit with two long corridors and windows at each end; there were machines and other items (blood pressure machine, charts, linen, etc.), pushed up against the side of one wall for each corridor. Across from the nursing station desk there was a television, a table and two chairs, and a table with three chairs. Lounge: Rectangle-shaped room with television, books and bookcase, information pamphlets, five small tables, piano, and 11 chairs Older traditional hospital design, a bit darker lighting |
| Bathrooms | Two: Corridor and near lounge | Two: Corridor and near lounge |
| Destination rooms on unit | None, lounges adjacent unit | None, lounge adjacent unit |
| Dining room for patients | No | No |
| Family support features (e.g., lounge, access to washrooms) | Two lounges (large and small) and access to bathroom | Large lounge with plants and a piano, and access to bathroom |
| Flooring type | Linoleum, light color and easy to distinguish objects | Linoleum, dark speckled flooring |
| Gardens and plants | Three plants in the corridor, garden visible outside | One plant on the desk, and six in the lounge; outside green space visible |
| Handrails | Not on unit or lounge | In corridors, but not in the lounge |
| Items on walls or ceilings | Paintings in corridors and lounge, a lot of messaging on the walls about patient care and hand washing | Paintings in corridors and lounge, a lot of messaging on the walls about patient care and hand washing |
| Televisions | Lounge only | Corridors and lounge |
| Temperature | Good in the corridor but lower in the lounge | Good in the corridor but lower in the lounge |
| Wayfinding | Signage available for reception, bathrooms, hand washing sinks and sanitizers, but not for consumer services, stairs or elevators | Signage available for reception, bathrooms and hand sanitizers, but not for hand washing sinks, consumer services, stairs or elevators |
| Windows | Windows only in lounge with views of parking, trees and street | Windows at the end of each corridor and in lounge with views of parking, trees and street |
| Unit 1 | Unit 2 | ||||||||
| Observations | Observations | ||||||||
| Time | Noise | Light | Visitor | Patient | Noise | Light | Visitor | Patient | |
| WEEKDAY | 8:00 | 2 | 1 | 1 | 5 | 2 | 1 | 5 | 0 |
| 9:00 | 3 | 1 | 0 | 6 | 3 | 1 | 3 | 1 | |
| 10:00 | 3 | 1 | 11 | 7 | 2 | 1 | 3 | 2 | |
| 11:00 | 3 | 1 | 15 | 7 | 3 | 1 | 11 | 3 | |
| 12:00 | 5 | 1 | 8 | 2 | 3 | 1 | 5 | 2 | |
| 13:00 | 3 | 1 | 8 | 5 | 3 | 1 | 8 | 4 | |
| 14:00 | 3 | 1 | 3 | 4 | 2 | 1 | 6 | 1 | |
| 15:00 | 3 | 1 | 2 | 5 | 3 | 1 | 18 | 1 | |
| 16:00 | 2 | 1 | 0 | 1 | 4 | 1 | 4 | 0 | |
| Total observations | 48 | 42 | 63 | 14 | |||||
| Observations | Observations | ||||||||
| Time | Noise | Light | Visitor | Patient | Noise | Light | Visitor | Patient | |
| WEEKEND | 8:00 | 2 | 1 | 0 | 6 | 2 | 2 | 5 | 0 |
| 9:00 | 2 | 1 | 4 | 5 | 4 | 2 | 7 | 3 | |
| 10:00 | 2 | 1 | 5 | 3 | 3 | 1 | 9 | 11 | |
| 11:00 | 4 | 1 | 15 | 3 | 4 | 1 | 9 | 8 | |
| 12:00 | 2 | 1 | 1 | 0 | 3 | 1 | 6 | 4 | |
| 13:00 | 2 | 1 | 0 | 0 | 2 | 1 | 22 | 6 | |
| 14:00 | 2 | 1 | 8 | 5 | 2 | 1 | 6 | 2 | |
| 15:00 | 2 | 1 | 11 | 1 | 2 | 2 | 7 | 3 | |
| 16:00 | 2 | 1 | 2 | 0 | 3 | 2 | 0 | 1 | |
| Total observations | 46 | 23 | 71 | 38 | |||||
| Day 1 (Wednesday) | Day 3 (Saturday) | Day 2 (Thursday) | Day 4 (Sunday) | |
| Unit 1 | Unit 1 | Unit 2 | Unit 2 | |
| Number of observations/day | 42 | 23 | 14 | 38 |
| Upright | 22 | 11 | 7 | 6 |
| Sitting | 20 | 12 | 7 | 32 |
| Patients admitted on unit | 22 | 23 | 28 | 28 |
| Women | 9 | 10 | 16 | 13 |
| Men | 13 | 13 | 12 | 15 |
| Age < 65 years | 2 | 3 | 2 | 1 |
| Age > 65 years | 20 | 20 | 26 | 27 |
| Patients observed on unit | 19 (86%) | 14 (61%) | 13 (46%) | 14 (50%) |
| Women | 6 (67%) | 10 (100%) | 3 (19%) | 7 (54%) |
| Men | 13 (100%) | 4 (31%) | 10 (83%) | 7 (47%) |
| Age < 65 years | 3 | 1 | 0 | 0 |
| Age > 65 years | 16 | 13 | 13 | 14 |
