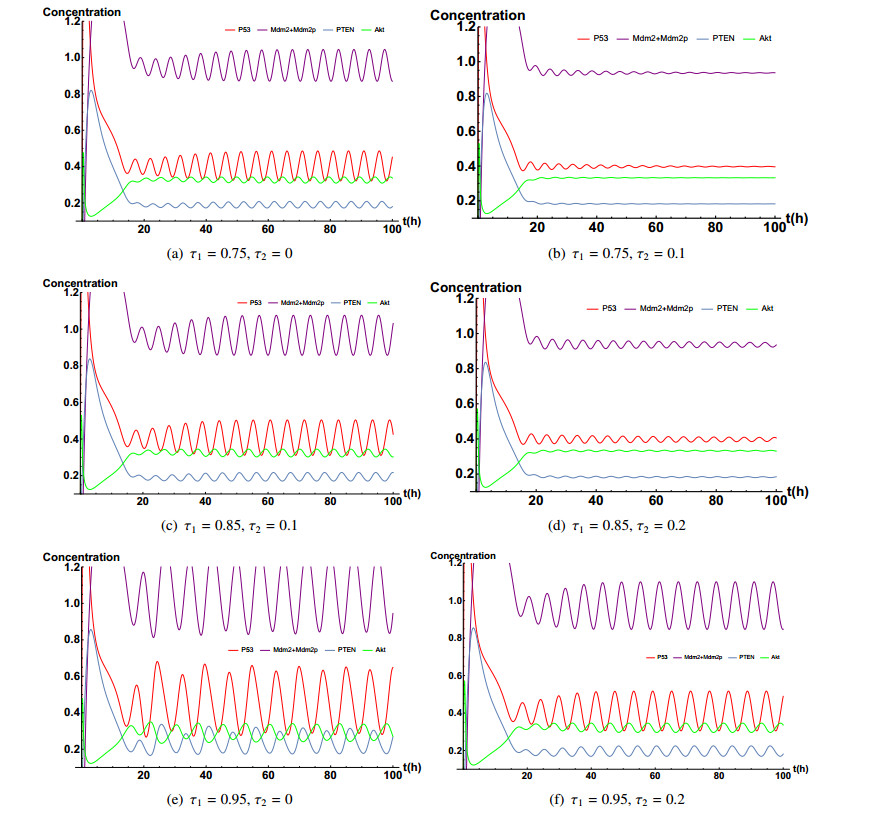
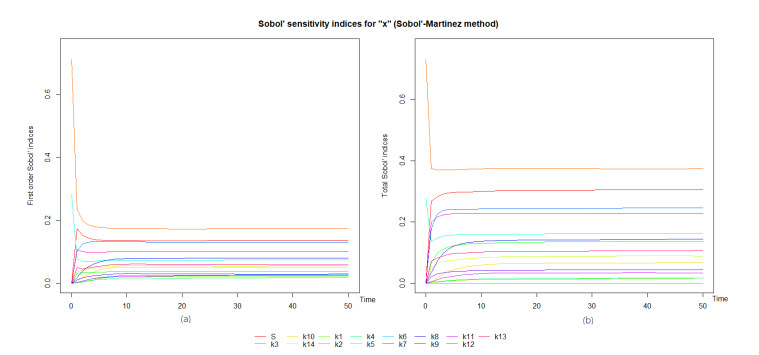
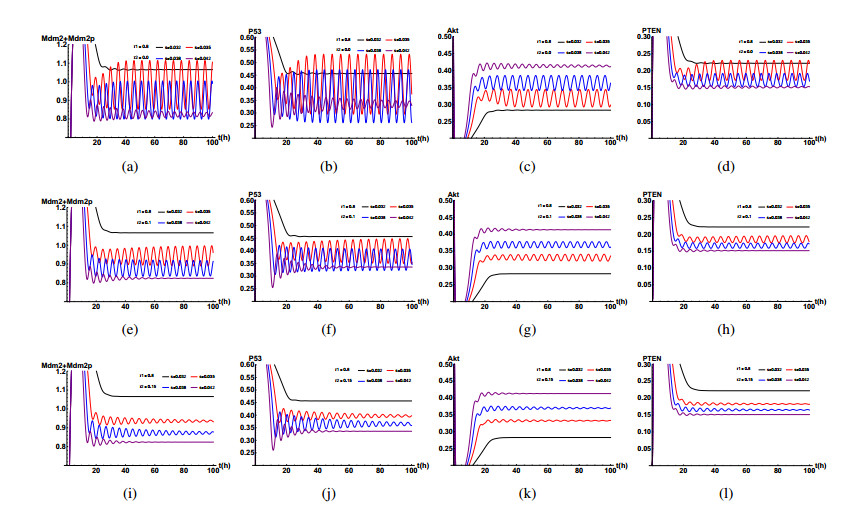
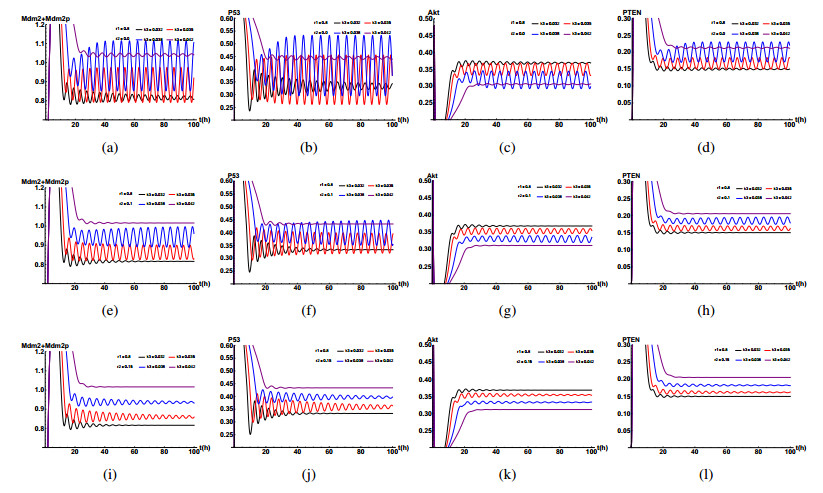
In this paper, a delayed mathematical model for the P53-Mdm2 network is developed. The P53-Mdm2 network we study is triggered by growth factor instead of DNA damage and the amount of DNA damage is regarded as zero. We study the influences of time delays, growth factor and other important chemical reaction rates on the dynamic behaviors in the system. It is shown that the time delay is a critical factor and its length determines the period, amplitude and stability of the P53 oscillation. Furthermore, as for some important chemical reaction rates, we also obtain some interesting results through numerical simulation. Especially, S (growth factor), k3 (rate constant for Mdm2p dephosphorylation), k10 (basal expression of PTEN) and k14 (Rate constant for PTEN-induced Akt dephosphorylation) could undermine the dynamic behavior of the system in different degree. These findings are expected to understand the mechanisms of action of several carcinogenic and tumor suppressor factors in humans under normal conditions.
Citation: Changyong Dai, Haihong Liu, Fang Yan. The role of time delays in P53 gene regulatory network stimulated by growth factor[J]. Mathematical Biosciences and Engineering, 2020, 17(4): 3794-3835. doi: 10.3934/mbe.2020213
In this paper, a delayed mathematical model for the P53-Mdm2 network is developed. The P53-Mdm2 network we study is triggered by growth factor instead of DNA damage and the amount of DNA damage is regarded as zero. We study the influences of time delays, growth factor and other important chemical reaction rates on the dynamic behaviors in the system. It is shown that the time delay is a critical factor and its length determines the period, amplitude and stability of the P53 oscillation. Furthermore, as for some important chemical reaction rates, we also obtain some interesting results through numerical simulation. Especially, S (growth factor), k3 (rate constant for Mdm2p dephosphorylation), k10 (basal expression of PTEN) and k14 (Rate constant for PTEN-induced Akt dephosphorylation) could undermine the dynamic behavior of the system in different degree. These findings are expected to understand the mechanisms of action of several carcinogenic and tumor suppressor factors in humans under normal conditions.

| [1] |
D. W. Meek, Tumour suppression by P53: A role for the DNA damage response, Nat. Rev. Cancer, 9 (2009), 714-723. doi: 10.1038/nrc2716

|
| [2] |
V. Rotter, p53, a transformation-related cellular-encoded protein, can be used as a biochemical marker for the detection of primary mouse tumor cells, P Natl. Acad. Sci. USA, 80 (1983), 2613-2617. doi: 10.1073/pnas.80.9.2613
|
| [3] |
F. Mantovani, L. Collavin, G. Del Sal, Mutant p53 as a guardian of the cancer cell, Cell Death Differ., 26 (2019), 199-212. doi: 10.1038/s41418-018-0246-9
|
| [4] | J. Bartek, J. Bartkova, B. Vojtesek, Z. Staskova, J. Lukas, A. Rejthar, et al., Aberrant expression of thep53 oncoprotein is a common feature of a wide spectrum of human malignancies, Oncogene, 6 (1991), 1699-1703. |
| [5] |
R. Iggo, J. Bartek, D. Lane, K. Gatter, A. L. Harris, J. Bartek, Increased expression of mutant forms of p53 oncogene in primary lung cancer, Lancet, 335 (1990), 675-679. doi: 10.1016/0140-6736(90)90801-B
|
| [6] |
A. J. Levine, P53, the cellular gatekeeper for growth and division, Cell, 88 (1997), 323-331. doi: 10.1016/S0092-8674(00)81871-1
|
| [7] |
J. E. Purvis, K. W. Karhohs, C. Mock, E. Batchelor, A. Loewer, G. Lahav, P53 dynamics control cell fate, Science, 336 (2012), 1440-1444. doi: 10.1126/science.1218351
|
| [8] |
K. H. Vousden, X. Lu, Live or let die: The cell's response to P53, Nat. Rev. Cancer, 2 (2002), 594-604. doi: 10.1038/nrc864
|
| [9] |
B. Vogelstein, D. Lane, A. Levine, Surfing the P53 network, Nature, 408 (2000), 307-310. doi: 10.1038/35042675
|
| [10] |
J. D. Oliner, K. W. Kinzler, P. S. Meltzer, D. L. George, B. Vogelstein, Amplification of a gene encoding a P53-associated protein in human sarcomas, Nature, 358 (1992), 80-83. doi: 10.1038/358080a0
|
| [11] |
M. H. G. Kubbutat, S. N. Jones, K. H. Vousden, Regulation of P53 stability by Mdm2, Nature, 387 (1997), 299-303. doi: 10.1038/42342-c1
|
| [12] |
J. H. Park, S. W. Yang, J. M. Park, S. H. Ka, J. Kim, Y. Kong, et al., Positive feedback regulation of P53 transactivity by DNA damage-induced ISG15 modification, Nat. Commun., 7 (2016), 12513. doi: 10.1038/ncomms12513
|
| [13] |
K. H. Vousden, D. P. Lane, P53 in health and disease, Nat. Rev. Mol. Cell Biol., 8 (2007), 275-283. doi: 10.1038/nrm2147
|
| [14] |
N. D. Lakin, S. P. Jackson, Regulation of P53 in response to DNA damage, Oncogene, 18 (1999), 7644-7655. doi: 10.1038/sj.onc.1203015
|
| [15] | U. M. Moll, O. Petrenko, The MDM2-P53 interaction, Mol. Cancer Res., 1 (2004), 1001-1008. |
| [16] |
Y. Haupt, R. Maya, A. Kazaz, M. Oren, Mdm2 promotes the rapid degradation of P53, Nature, 387 (1997), 296-299. doi: 10.1038/387296a0
|
| [17] |
G. Liao, D. Yang, L. Ma, W. Li, L. Hu, L, Zeng, et al., The development of piperidinones as potent MDM2-P53 protein-protein interaction inhibitors for cancer therapy, Eur. J. Med. Chem., 159 (2018), 1-9. doi: 10.1016/j.ejmech.2018.09.044
|
| [18] |
D. Cao, T. K. Ng, Y. W. Y. Yip, A. L. Young, C. P. Pang, W. K. Chu, et al., P53 inhibition by MDM2 in human pterygium, Exp. Eye Res., 175 (2018), 142-147. doi: 10.1016/j.exer.2018.06.021
|
| [19] |
R. Li, P. D. Sutphin, D. Schwartz, D. Matas, N. Almog, R. Wolkowicz, et al., Mutant p53 protein expression interferes with p53-independent apoptotic pathways, Oncogene, 16 (1998), 3269-3277. doi: 10.1038/sj.onc.1201867
|
| [20] |
G. Blandino, A. J Levine, M. Oren, Mutant p53 gain of function: Differential effects of different p53 mutants on resistance of cultured cells to chemotherapy, Oncogene, 18 (1999), 477-485. doi: 10.1038/sj.onc.1202314
|
| [21] |
G. Bossi, E. Lapi, S. Strano, C. Rinaldo, G. Blandino, A. Sacchi, Mutant p53 gain of function: Reduction of tumor malignancy of human cancer cell lines through abrogation of mutant p53 expression, Oncogene, 25 (2006), 304-309. doi: 10.1038/sj.onc.1209026
|
| [22] |
M. S. Irwin, K. Kondo, M. C. Marin, L. S. Cheng, W. C. Hahn, W. G. Kaelin, Chemosensitivity linked to p73 function, Cancer Cell, 3 (2003), 403-410. doi: 10.1016/S1535-6108(03)00078-3
|
| [23] |
R. Maya, R. Segel, U. Alon, A. J. Levine, Generation of oscillations by the P53-Mdm2 feedback loop: A theoretical and experimental study, P Natl. Acad. Sci. USA, 97 (2000), 11250-11255. doi: 10.1073/pnas.210171597
|
| [24] |
L. Ma, J. Wagner, J. Rice, W. Hu, A. Levine, G. Stolovitzky, A plausible model for the digital response of P53 to DNA damage, P Natl. Acad. Sci. USA, 102 (2005), 14266-14271. doi: 10.1073/pnas.0501352102
|
| [25] |
T. Zhang, P. Brazhnik, J. J. Tyson, Exploring mechanisms of the DNA-damage response: P53 pulses and their possible relevance to apoptosis, Cell Cycle, 6 (2007), 85-94. doi: 10.4161/cc.6.1.3705
|
| [26] |
X. P. Zhang, F. Liu, Z. Cheng, W. Wang, Cell fate decision mediated by P53 pulses, P Natl. Acad. Sci. USA., 106 (2009), 12245-12250. doi: 10.1073/pnas.0813088106
|
| [27] |
X. P. Zhang, F. Liu, W. Wang, Two-phase dynamics of P53 in the DNA damage response, P Natl. Acad. Sci. USA, 108 (2011), 8990-8995. doi: 10.1073/pnas.1100600108
|
| [28] |
T. Sun, W. Yang, J. Liu, P. Shen, Modeling the basal dynamics of P53 system, PLoS ONE, 6 (2011), e27882. doi: 10.1371/journal.pone.0027882
|
| [29] |
B. C. Torrico, M. P. d. A. Filho, T. A. Lima, M. D. D. N. Forte, R. C. Sa, F. G. Nogueira, Tuning of a dead-time compensator focusing on industrial processes, Isa Transact., 83 (2018), 189-198. doi: 10.1016/j.isatra.2018.09.003
|
| [30] |
T. Zhang, P. Brazhnik, J. J. Tyson, Computational Analysis of Dynamical Responses to the Intrinsic Pathway of Programmed Cell Death, Biophys J., 97 (2009), 415-434. doi: 10.1016/j.bpj.2009.04.053
|
| [31] |
K. H. Chong, S. Samarasinghe, D. Kulasiri, J. Zheng, Mathematical modelling of core regulatory mechanism in P53 protein that activates apoptotic switch, J. Theor. Biol., 462 (2019), 134-147. doi: 10.1016/j.jtbi.2018.11.008
|
| [32] |
Y. Zhang, Y. Xiong, W. G. Yarbrough, ARF promotes MDM2 degradation and stabilizes P53: ARF-INK4a locus deletion impairs both the Rb and P53 tumor suppression pathways, Cell, 92 (1998), 725-735. doi: 10.1016/S0092-8674(00)81401-4
|
| [33] |
E. Shaulian, D. Resnitzky, O. Shifman, G. Blandino, A. Amsterdam, A. Yayon, et al., Induction of Mdm2 and enhancement of cell survival by bFGF, Oncogene, 15 (1997), 2717-2725. doi: 10.1038/sj.onc.1201453
|
| [34] |
Y. Ogawara, S. Kishishita, T. Obata, Y. Isazawa, T. Suzuki, K. Tanaka, et al, Akt enhances Mdm2- mediated ubiquitination and degradation of P53, J. Biol. Chem., 277 (2002), 21843-21850. doi: 10.1074/jbc.M109745200
|
| [35] |
A. Carnero, C. Blanco-Aparicio, O. Renner, W. Link, The PTEN/PI3K/Akt signalling pathway in cancer, therapeutic implications, Curr. Cancer Drug Tar., 8 (2008), 187-198. doi: 10.2174/156800908784293659
|
| [36] |
X. Tian, B. Huang, X. P. Zhang, M. Lu, W. Wang, Modeling the response of a tumor-suppressive network to mitogenic and oncogenic signals, P Natl. Acad. Sci. USA, 114 (2017), 5337-5342. doi: 10.1073/pnas.1702412114
|
| [37] |
B. Novak, J. J. Tyson, Design principles of biochemical oscillators, Nat. Rev. Mol. Cell Biol., 9 (2008), 981-991. doi: 10.1038/nrm2530
|
| [38] |
J. R. Pomerening, S. Y. Kim, J. E. Ferrell, Systems-level dissection of the cell-cycle oscillator: Bypassing positive feedback produces damped oscillations, Cell, 122 (2005), 565-578. doi: 10.1016/j.cell.2005.06.016
|
| [39] |
K. Jonak, M. Kurpas, K. Szoltysek, J. Patryk, A. Abramowicz, K. Puszynski, A novel mathematical model of ATM/P53/NF-kB pathways points to the importance of the DDR switch-off mechanisms, BMC Syst. Biol., 10 (2016), 75. doi: 10.1186/s12918-016-0293-0
|
| [40] |
A. Honkela, J. Peltonen, H. Topa, I. Charapitsa, F. Matarese, Genome-wide modeling of transcription kinetics reveals patterns of RNA production delays, P Natl. Acad. Sci. USA, 112 (2015), 13115-13120. doi: 10.1073/pnas.1420404112
|
| [41] |
A. Prindle, J. Selimkhanov, H. Li, I. Razinkov, L. S. Tsimring, J. Hasty, Rapid and tunable post-translational coupling of genetic circuits, Nature, 508 (2014), 387-391. doi: 10.1038/nature13238
|
| [42] |
H. K. Yalamanchili, B. Yan, M. J. Li, J. Qin, Z. Zhao, F. Y. L. Chin, et al., DDGni: Dynamic delay gene-network inference from high-temporal data using gapped local alignment, Bioinformatics, 30 (2014), 377-383. doi: 10.1093/bioinformatics/btt692
|
| [43] |
V. Stambolic, D. Macpherson, D. Sas, Y. Lin, B. Snow, Regulation of PTEN transcription by P53, Mol. Cell, 8 (2001), 317-325. doi: 10.1016/S1097-2765(01)00323-9
|
| [44] |
Y. Barak, E. Gottlieb, T. Juven-Gershon, M. Oren, Regulation of mdm2 expression by P53: Alternative promoters produce transcripts with nonidentical translation potential, Gene Dev., 8 (1994), 1739-1749. doi: 10.1101/gad.8.15.1739
|
| [45] |
K. B. Wee, B. D. Aguda, Akt versus P53 in a network of oncogenes and tumor suppressor genes regulating cell survival and death, Biophys J., 91 (2006), 857-865. doi: 10.1529/biophysj.105.077693
|
| [46] |
D. Qiu, L. Mao, S. Kikuchi, M. Tomita, Sustained MAPK activation is dependent on continual NGF receptor regeneration, Dev. Growth Differ., 46 (2004), 393-403. doi: 10.1111/j.1440-169x.2004.00756.x
|
| [47] |
B. N. Kholodenko, Negative feedback and ultrasensitivity can bring about oscillations in the mitogen-activated protein kinase cascades, Eur. J. Biochem., 267 (2000), 1583-1588. doi: 10.1046/j.1432-1327.2000.01197.x
|
| [48] |
Y. Zhang, H. Liu, F. Yan, J. Zhou, Oscillatory dynamics of p38 activity with transcriptional and translational time delays, Sci. Rep. 7, (2017), 11495. doi: 10.1038/s41598-017-11149-5
|
| [49] |
Y. Harima, Y. Takashima, Y. Ueda, T. Ohtsuka, R. Kageyama, Accelerating the tempo of the segmentation clock by reducing the number of introns in the Hes7 gene, Cell Rep., 3, (2013), 1-7. doi: 10.1016/j.celrep.2012.11.012
|
| [50] | Y. Takashima, T. Ohtsuka, A. Gonzalez, H. Miyachi, R. Kageyama, Intronic delay is essential for oscillatory expression in the segmentation clock, P Natl. Acad. Sci. USA, 108, (2011), 3300-3305. |
| [51] |
J. Lewis, Autoinhibition with transcriptional delay: A simple mechanism for the zebrafish somitogenesis oscillator, Curr. Biol., 13, (2003), 1398-1408. doi: 10.1016/S0960-9822(03)00534-7
|
| [52] |
A. Audibert, D. Weil, F. Dautry, In vivo kinetics of mrna splicing and transport in mammalian cells, Mol. Cell Biol., 22, (2002), 6706-6718. doi: 10.1128/MCB.22.19.6706-6718.2002
|
| [53] | J. Fruth, New methods for the sensitivity analysis of black-box functions with an application to sheet metal forming, TU Dortmund University, 2015. |
| [54] |
B. P. Zhou, Y. Liao, W. Xia, Y. Zou, B. Spohn, M.C. Hung, HER-2/neu induces P53 ubiquitination via Akt-mediated MDM2 phosphorylation, Nat. Cell Biol., 3 (2001), 973-982. doi: 10.1038/ncb1101-973
|
| [55] | S. Ruan, J. Wei, On the zeros of transcendental functions with applications to stability of delay differential equations with two delays, Dynam. Cont. Dis. Ser. A, 10 (2003), 863-874. |
| [56] | B. D. Hassard, N. D. Kazarinoff, Y. H. Wan, Theory and applications of Hopf bifurcation, Cambridge University Press, 1981. |
Figures(11) / Tables(2)

Changyong Dai, Haihong Liu, Fang Yan. The role of time delays in P53 gene regulatory network stimulated by growth factor[J]. Mathematical Biosciences and Engineering, 2020, 17(4): 3794-3835. doi: 10.3934/mbe.2020213







 DownLoad:
DownLoad: