Citation: Lufeng Yao, Haiqing Wang, Feng Zhang, Liping Wang, Jianghui Dong. Minimally invasive treatment of calcaneal fractures via the sinus tarsi approach based on a 3D printing technique[J]. Mathematical Biosciences and Engineering, 2019, 16(3): 1597-1610. doi: 10.3934/mbe.2019076

| [1] | N. Gougoulias, A. Khanna and D. J. McBride, et al., Management of calcaneal fractures: Systematic review of randomized trials, Brit. Med. Bull., 92 (2009), 153–167. |
| [2] | N. Epstein, S. Chandran and L. Chou, Current concepts review: Intra-articular fractures of the calcaneus, Foot. Ankle. Int., 33 (2012), 79–86. |
| [3] | M. J. Gardner, S. E. Nork and D. P. Barei, et al., Secondary soft tissue compromise in tongue-type calcaneus fractures, J. Orthop. Trauma., 22 (2008), 439–45. |
| [4] | T. Tomesen, J. Biert and J. P. Frolke, Treatment of displaced intra-articular calcaneal fractures with closed reduction and percutaneous screw fixation, J. Bone. Joint. Surg. Am., 93 (2011), 920–928. |
| [5] | B. S. Sivakumar, P. Wong and C. G. Dick, et al., Arthroscopic reduction and percutaneous fixation of selected calcaneus fractures: Surgical technique and early results, J. Orthop. Trauma., 28 (2014), 569–576. |
| [6] | A. A. Abdelgawad and E. Kanlic, Minimally invasive (sinus tarsi) approach for open reduction and internal fixation of intra-articular calcaneus fractures in children: Surgical technique and case report of two patients, J. Foot. Ankle. Surg., 54 (2015), 135–139. |
| [7] | M. Ni, J. Mei and K. Li, et al., The primary stability of different implants for intra-articular calcaneal fractures: An in vitro study, Biomed. Eng. Online., 17 (2018), 50. |
| [8] | Ihab I. El-Desouky and W. Abu Senna, The outcome of super-cutaneous locked plate fixation with percutaneous reduction of displaced intra-articular calcaneal fractures, Injury., 48 (2017), 525–530. |
| [9] | C. H. Park and D. H. Yoon, Role of Subtalar Arthroscopy in Operative Treatment of Sanders Type 2 Calcaneal Fractures Using a Sinus Tarsi Approach, Foot. Ankle. Int., 39 (2018), 443–449. |
| [10] | T. Zhang, Y. Su and W. Chen, et al., Displaced intra-articular calcaneal fractures treated in a minimally invasive fashion: Longitudinal approach versus sinus tarsi approach, J. Bone. Joint. Surg. Am., 96 (2014), 302–309. |
| [11] | J. H. Yeo, H. J. Cho and K. B. Lee, Comparison of two surgical approaches for displaced intra-articular calcaneal fractures: Sinus tarsi versus extensile lateral approach, BMC. Musculoskeletal. Disord., 16 (2015), 63. |
| [12] | H. C. Zhou, T. Yu and H. Y. Ren, et al., Clinical Comparison of Extensile Lateral Approach and Sinus Tarsi Approach Combined with Medial Distraction Technique for Intra-Articular Calcaneal Fractures, Orthop. Surg., 9 (2017), 77–85. |
| [13] | M. Ni, D. W. C. Wong and J. Mei, et al., Biomechanical comparison of locking plate and crossing metallic and absorbable screws fixations for intra-articular calcaneal fractures, Sci. China. Life. Sci., 59 (2016), 958–964. |
| [14] | I. L. Gitajn, M. Abousayed and R. J. Toussaint, et al., Anatomic Alignment and Integrity of the Sustentaculum Tali in Intra-Articular Calcaneal Fractures: Is the Sustentaculum Tali Truly Constant? J. Bone. Joint. Surg. Am., 96 (2014), 1000–1005. |
| [15] | A. R. Hsu, R. B. Anderson and B. E. Cohen, Advances in Surgical Management of Intra-articular Calcaneus Fractures, J. Am. Acad. Orthop. Surg., 23 (2015), 399–407. |
| [16] | B. Swartman, D. Frere and W. Wei, et al., Wire Placement in the Sustentaculum Tali Using a 2D Projection-Based Software Application for Mobile C-Arms: Cadaveric Study, Foot. Ankle. Int., 39 (2018), 485–492. |
| [17] | P. P. Lin, S. Roe and M. Kay, et al., Placement of screws in the sustentaculum tali. A calcaneal fracture model, Clin. Orthop. Relat. Res., (1998), 194–201. |
| [18] | C. Wang, D. Huang and X. Ma, et al., Sustentacular screw placement with guidance during ORIF of calcaneal fracture: An anatomical specimen study, J. Orthop. Surg. Res., 12 (2017), 78. |
| [19] | A. T. Scott, D. A. Pacholke and K. S. Hamid, Radiographic and CT Assessment of Reduction of Calcaneus Fractures Using a Limited Sinus Tarsi Incision, Foot. Ankle. Int., 37 (2016), 950–957. |
| [20] | K. J. Chung, D. Y. Hong and Y. T. Kim, et al., Preshaping plates for minimally invasive fixation of calcaneal fractures using a real-size 3D-printed model as a preoperative and intraoperative tool, Foot. Ankle. Int., 35 (2014), 1231–1236. |
| [21] | A. R. Hsu and J. K. Ellington, Patient-Specific 3-Dimensional Printed Titanium Truss Cage With Tibiotalocalcaneal Arthrodesis for Salvage of Persistent Distal Tibia Nonunion, Foot. Ankle. Spec., 8 (2015), 483–489. |
| [22] | J. R. Jastifer and P. A. Gustafson, Three-Dimensional Printing and Surgical Simulation for Preoperative Planning of Deformity Correction in Foot and Ankle Surgery, J. Foot. Ankle. Surg., 56 (2017), 191–195. |
| [23] | W. Zheng, M. D. Zhenyu Tao and M. D. Yiting Lou, et al., Comparison of the Conventional Surgery and the Surgery Assisted by 3d Printing Technology in the Treatment of Calcaneal Fractures, J. Invest. Surg., (2017), 1–11. |
| [24] | T. Kurozumi, Y. Jinno and T. Sato, et al., Open reduction for intra-articular calcaneal fractures: Evaluation using computed tomography, Foot. Ankle. Int., 24 (2003), 942–948. |
| [25] | H. B. Kitaoka, I. J. Alexander and R. S. Adelaar, et al., Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes, Foot. Ankle. Int., 15 (1994), 349. |
| [26] | M. Freyd, The Graphic Rating Scale, J. Educ. Psychol., 14 (1923), 83–102. |
| [27] | B. W. Bussewitz and C. F. Hyer, Screw placement relative to the calcaneal fracture constant fragment: An anatomic study, J. Foot. Ankle. Surg., 54 (2015), 392–394. |
| [28] | M. Qiang, Y. Chen and K. Zhang, et al., Effect of sustentaculum screw placement on outcomes of intra-articular calcaneal fracture osteosynthesis: A prospective cohort study using 3D CT, Int. J. Surg., 19 (2015), 72–77. |
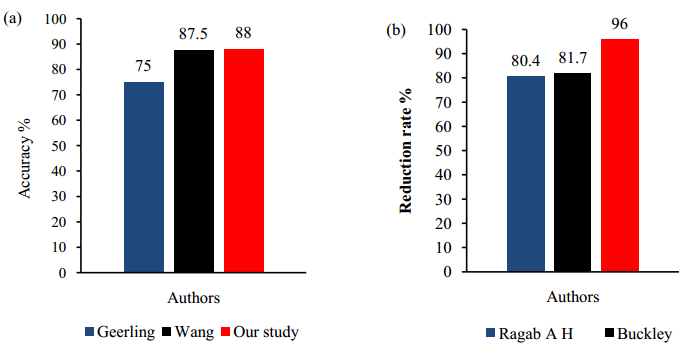
| [29] | J. Geerling, D. Kendoff and M. Citak, et al., Intraoperative 3D imaging in calcaneal fracture care-clinical implications and decision making, J. Trauma., 66 (2009), 768–773. |
| [30] | R. Kakwani and M. Siddique, Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial, J. Bone. Joint. Surg. Am., 84 (2002), 1733–1744. |
| [31] | A. H. Ragab, I. M. Mubark and A. M. Nagi, et al., Treatment of subtalar calcanean fractures using trans-osseous limited lateral approach, Ortop. Traumatol. Rehabil., 16 (2014), 629–638. |
Figures(7) / Tables(1)

Lufeng Yao, Haiqing Wang, Feng Zhang, Liping Wang, Jianghui Dong. Minimally invasive treatment of calcaneal fractures via the sinus tarsi approach based on a 3D printing technique[J]. Mathematical Biosciences and Engineering, 2019, 16(3): 1597-1610. doi: 10.3934/mbe.2019076







 DownLoad:
DownLoad: