Citation: Michael R Hamblin. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation[J]. AIMS Biophysics, 2017, 4(3): 337-361. doi: 10.3934/biophy.2017.3.337

| [1] | Hamblin MR (2017) History of Low-Level Laser (Light) Therapy, In: Hamblin MR, de Sousa MVP, Agrawal T, Editors, Handbook of Low-Level Laser Therapy, Singapore: Pan Stanford Publishing. |
| [2] |
Anders JJ, Lanzafame RJ, Arany PR (2015) Low-level light/laser therapy versus photobiomodulation therapy. Photomed Laser Surg 33: 183–184. doi: 10.1089/pho.2015.9848

|
| [3] | Hamblin MR, de Sousa MVP, Agrawal T (2017) Handbook of Low-Level Laser Therapy, Singapore: Pan Stanford Publishing. |
| [4] |
de Freitas LF, Hamblin MR (2016) Proposed mechanisms of photobiomodulation or low-level light therapy. IEEE J Sel Top Quantum Electron 22: 348–364. doi: 10.1109/JSTQE.2016.2561201
|
| [5] |
Wang Y, Huang YY, Wang Y, et al. (2016) Photobiomodulation (blue and green light) encourages osteoblastic-differentiation of human adipose-derived stem cells: role of intracellular calcium and light-gated ion channels. Sci Rep 6: 33719. doi: 10.1038/srep33719
|
| [6] |
Wang L, Jacques SL, Zheng L (1995) MCML-Monte Carlo modeling of light transport in multi-layered tissues. Comput Meth Prog Bio 47: 131–146. doi: 10.1016/0169-2607(95)01640-F
|
| [7] | Huang YY, Chen AC, Carroll JD, et al. (2009) Biphasic dose response in low level light therapy. Dose Response 7: 358–383. |
| [8] |
Huang YY, Sharma SK, Carroll JD, et al. (2011) Biphasic dose response in low level light therapy-an update. Dose Response 9: 602–618. doi: 10.2203/dose-response.11-009.Hamblin
|
| [9] |
Mason MG, Nicholls P, Cooper CE (2014) Re-evaluation of the near infrared spectra of mitochondrial cytochrome c oxidase: Implications for non invasive in vivo monitoring of tissues. Biochim Biophys Acta 1837: 1882–1891. doi: 10.1016/j.bbabio.2014.08.005
|
| [10] |
Karu TI, Pyatibrat LV, Kolyakov SF, et al. (2005) Absorption measurements of a cell monolayer relevant to phototherapy: reduction of cytochrome c oxidase under near IR radiation. J Photochem Photobiol B 81: 98–106. doi: 10.1016/j.jphotobiol.2005.07.002
|
| [11] |
Karu TI (2010) Multiple roles of cytochrome c oxidase in mammalian cells under action of red and IR-A radiation. IUBMB Life 62: 607–610. doi: 10.1002/iub.359
|
| [12] |
Wong-Riley MT, Liang HL, Eells JT, et al. (2005) Photobiomodulation directly benefits primary neurons functionally inactivated by toxins: role of cytochrome c oxidase. J Biol Chem 280: 4761–4771. doi: 10.1074/jbc.M409650200
|
| [13] |
Lane N (2006) Cell biology: power games. Nature 443: 901–903. doi: 10.1038/443901a
|
| [14] |
Pannala VR, Camara AK, Dash RK (2016) Modeling the detailed kinetics of mitochondrial cytochrome c oxidase: Catalytic mechanism and nitric oxide inhibition. J Appl Physiol 121: 1196–1207. doi: 10.1152/japplphysiol.00524.2016
|
| [15] |
Fernandes AM, Fero K, Driever W, et al. (2013) Enlightening the brain: linking deep brain photoreception with behavior and physiology. Bioessays 35: 775–779. doi: 10.1002/bies.201300034
|
| [16] |
Poletini MO, Moraes MN, Ramos BC, et al. (2015) TRP channels: a missing bond in the entrainment mechanism of peripheral clocks throughout evolution. Temperature 2: 522–534. doi: 10.1080/23328940.2015.1115803
|
| [17] |
Caterina MJ, Pang Z (2016) TRP channels in skin biology and pathophysiology. Pharmaceuticals 9: 77. doi: 10.3390/ph9040077
|
| [18] |
Montell C (2011) The history of TRP channels, a commentary and reflection. Pflugers Arch 461: 499–506. doi: 10.1007/s00424-010-0920-3
|
| [19] |
Smani T, Shapovalov G, Skryma R, et al. (2015) Functional and physiopathological implications of TRP channels. Biochim Biophys Acta 1853: 1772–1782. doi: 10.1016/j.bbamcr.2015.04.016
|
| [20] |
Cronin MA, Lieu MH, Tsunoda S (2006) Two stages of light-dependent TRPL-channel translocation in Drosophila photoreceptors. J Cell Sci 119: 2935–2944. doi: 10.1242/jcs.03049
|
| [21] |
Sancar A (2000) Cryptochrome: the second photoactive pigment in the eye and its role in circadian photoreception. Annu Rev Biochem 69: 31–67. doi: 10.1146/annurev.biochem.69.1.31
|
| [22] |
Weber S (2005) Light-driven enzymatic catalysis of DNA repair: a review of recent biophysical studies on photolyase. Biochim Biophys Acta 1707: 1–23. doi: 10.1016/j.bbabio.2004.02.010
|
| [23] | Gillette MU, Tischkau SA (1999) Suprachiasmatic nucleus: the brain's circadian clock. Recent Prog Horm Res 54: 33–58. |
| [24] |
Kofuji P, Mure LS, Massman LJ, et al. (2016) Intrinsically photosensitive petinal ganglion cells (ipRGCs) are necessary for light entrainment of peripheral clocks. PLoS One 11: e0168651. doi: 10.1371/journal.pone.0168651
|
| [25] |
Sexton T, Buhr E, Van Gelder RN (2012) Melanopsin and mechanisms of non-visual ocular photoreception. J Biol Chem 287: 1649–1656. doi: 10.1074/jbc.R111.301226
|
| [26] |
Ho MW (2015) Illuminating water and life: Emilio Del Giudice. Electromagn Biol Med 34: 113–122. doi: 10.3109/15368378.2015.1036079
|
| [27] |
Inoue S, Kabaya M (1989) Biological activities caused by far-infrared radiation. Int J Biometeorol 33: 145–150. doi: 10.1007/BF01084598
|
| [28] |
Damodaran S (2015) Water at biological phase boundaries: its role in interfacial activation of enzymes and metabolic pathways. Subcell Biochem 71: 233–261. doi: 10.1007/978-3-319-19060-0_10
|
| [29] | Chai B, Yoo H, Pollack GH (2009) Effect of radiant energy on near-surface water. J Phys Chem B 113: 13953–13958. |
| [30] |
Pollack GH, Figueroa X, Zhao Q (2009) Molecules, water, and radiant energy: new clues for the origin of life. Int J Mol Sci 10: 1419–1429. doi: 10.3390/ijms10041419
|
| [31] |
Sommer AP, Haddad M, Fecht HJ (2015) Light effect on water viscosity: implication for ATP biosynthesis. Sci Rep 5: 12029. doi: 10.1038/srep12029
|
| [32] | FDA (2016) Code of Federal Regulations 21CFR890.5500, Title 21, Vol 8. |
| [33] |
Chen ACH, Huang YY, Arany PR, et al. (2009) Role of reactive oxygen species in low level light therapy. Proc SPIE 7165: 716502–716511. doi: 10.1117/12.814890
|
| [34] |
Chen AC, Arany PR, Huang YY, et al. (2011) Low-level laser therapy activates NF-kB via generation of reactive oxygen species in mouse embryonic fibroblasts. PLoS One 6: e22453. doi: 10.1371/journal.pone.0022453
|
| [35] |
Sharma SK, Kharkwal GB, Sajo M, et al. (2011) Dose response effects of 810 nm laser light on mouse primary cortical neurons. Lasers Surg Med 43: 851–859. doi: 10.1002/lsm.21100
|
| [36] |
Tatmatsu-Rocha JC, Ferraresi C, Hamblin MR, et al. (2016) Low-level laser therapy (904 nm) can increase collagen and reduce oxidative and nitrosative stress in diabetic wounded mouse skin. J Photochem Photobiol B 164: 96–102. doi: 10.1016/j.jphotobiol.2016.09.017
|
| [37] |
De Marchi T, Leal Junior EC, Bortoli C, et al. (2012) Low-level laser therapy (LLLT) in human progressive-intensity running: effects on exercise performance, skeletal muscle status, and oxidative stress. Lasers Med Sci 27: 231–236. doi: 10.1007/s10103-011-0955-5
|
| [38] |
Fillipin LI, Mauriz JL, Vedovelli K, et al. (2005) Low-level laser therapy (LLLT) prevents oxidative stress and reduces fibrosis in rat traumatized Achilles tendon. Lasers Surg Med 37: 293–300. doi: 10.1002/lsm.20225
|
| [39] | Huang YY, Nagata K, Tedford CE, et al. (2013) Low-level laser therapy (LLLT) reduces oxidative stress in primary cortical neurons in vitro. J Biophotonics 6: 829–838. |
| [40] |
Hervouet E, Cizkova A, Demont J, et al. (2008) HIF and reactive oxygen species regulate oxidative phosphorylation in cancer. Carcinogenesis 29: 1528–1537. doi: 10.1093/carcin/bgn125
|
| [41] | Madungwe NB, Zilberstein NF, Feng Y, et al. (2016) Critical role of mitochondrial ROS is dependent on their site of production on the electron transport chain in ischemic heart. Am J Cardiovasc Dis 6: 93–108. |
| [42] |
Martins DF, Turnes BL, Cidral-Filho FJ, et al. (2016) Light-emitting diode therapy reduces persistent inflammatory pain: Role of interleukin 10 and antioxidant enzymes. Neuroscience 324: 485–495. doi: 10.1016/j.neuroscience.2016.03.035
|
| [43] |
Macedo AB, Moraes LH, Mizobuti DS, et al. (2015) Low-level laser therapy (LLLT) in dystrophin-deficient muscle cells: effects on regeneration capacity, inflammation response and oxidative stress. PLoS One 10: e0128567. doi: 10.1371/journal.pone.0128567
|
| [44] |
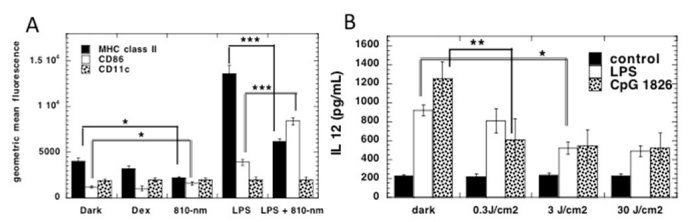
Chen AC, Huang YY, Sharma SK, et al. (2011) Effects of 810-nm laser on murine bone-marrow-derived dendritic cells. Photomed Laser Surg 29: 383–389. doi: 10.1089/pho.2010.2837
|
| [45] |
Yamaura M, Yao M, Yaroslavsky I, et al. (2009) Low level light effects on inflammatory cytokine production by rheumatoid arthritis synoviocytes. Lasers Surg Med 41: 282–290. doi: 10.1002/lsm.20766
|
| [46] |
Hwang MH, Shin JH, Kim KS, et al. (2015) Low level light therapy modulates inflammatory mediators secreted by human annulus fibrosus cells during intervertebral disc degeneration in vitro. Photochem Photobiol 91: 403–410. doi: 10.1111/php.12415
|
| [47] |
Imaoka A, Zhang L, Kuboyama N, et al. (2014) Reduction of IL-20 expression in rheumatoid arthritis by linear polarized infrared light irradiation. Laser Ther 23: 109–114. doi: 10.5978/islsm.14-OR-08
|
| [48] |
Lim W, Choi H, Kim J, et al. (2015) Anti-inflammatory effect of 635 nm irradiations on in vitro direct/indirect irradiation model. J Oral Pathol Med 44: 94–102. doi: 10.1111/jop.12204
|
| [49] | Choi H, Lim W, Kim I, et al. (2012) Inflammatory cytokines are suppressed by light-emitting diode irradiation of P. gingivalis LPS-treated human gingival fibroblasts: inflammatory cytokine changes by LED irradiation. Lasers Med Sci 27: 459–467. |
| [50] |
Sakurai Y, Yamaguchi M, Abiko Y (2000) Inhibitory effect of low-level laser irradiation on LPS-stimulated prostaglandin E2 production and cyclooxygenase-2 in human gingival fibroblasts. Eur J Oral Sci 108: 29–34. doi: 10.1034/j.1600-0722.2000.00783.x
|
| [51] |
Nomura K, Yamaguchi M, Abiko Y (2001) Inhibition of interleukin-1beta production and gene expression in human gingival fibroblasts by low-energy laser irradiation. Lasers Med Sci 16: 218–223. doi: 10.1007/PL00011358
|
| [52] |
Briken V, Mosser DM (2011) Editorial: switching on arginase in M2 macrophages. J Leukoc Biol 90: 839–841. doi: 10.1189/jlb.0411203
|
| [53] |
Whyte CS, Bishop ET, Ruckerl D, et al. (2011) Suppressor of cytokine signaling (SOCS)1 is a key determinant of differential macrophage activation and function. J Leukoc Biol 90: 845–854. doi: 10.1189/jlb.1110644
|
| [54] | Xu H, Wang Z, Li J, et al. (2017) The polarization states of microglia in TBI: A new paradigm for pharmacological intervention. Neural Plast 2017: 5405104. |
| [55] | Lu J, Xie L, Liu C, et al. (2017) PTEN/PI3k/AKT regulates macrophage polarization in emphysematous mice. Scand J Immunol. |
| [56] |
Saha B, Kodys K, Szabo G (2016) Hepatitis C virus-induced monocyte differentiation into polarized M2 macrophages promotes stellate cell activation via TGF-beta. Cell Mol Gastroenterol Hepatol 2: 302–316. doi: 10.1016/j.jcmgh.2015.12.005
|
| [57] | Fernandes KP, Souza NH, Mesquita-Ferrari RA, et al. (2015) Photobiomodulation with 660-nm and 780-nm laser on activated J774 macrophage-like cells: Effect on M1 inflammatory markers. J Photochem Photobiol B 153: 344–351. |
| [58] |
Silva IH, de Andrade SC, de Faria AB, et al. (2016) Increase in the nitric oxide release without changes in cell viability of macrophages after laser therapy with 660 and 808 nm lasers. Lasers Med Sci 31: 1855–1862. doi: 10.1007/s10103-016-2061-1
|
| [59] |
von Leden RE, Cooney SJ, Ferrara TM, et al. (2013) 808 nm wavelength light induces a dose-dependent alteration in microglial polarization and resultant microglial induced neurite growth. Lasers Surg Med 45: 253–263. doi: 10.1002/lsm.22133
|
| [60] | Sousa KB, de Santana Araujo L, Pedroso NM, et al. (2017) Photobiomodulation effects on gene and protein expression of proinflammatory chemokines and cytokines by J774 macrophages polarized to M1 phenotype. Lasers Surg Med 49: 36. |
| [61] | de Lima FJ, de Oliveira Neto OB, Barbosa FT, et al. (2016) Is there a protocol in experimental skin wounds in rats using low-level diode laser therapy (LLDLT) combining or not red and infrared wavelengths? Systematic review. Lasers Med Sci 31: 779–787. |
| [62] | Tchanque-Fossuo CN, Ho D, Dahle SE, et al. (2016) Low-level light therapy for treatment of diabetic foot ulcer: a review of clinical experiences. J Drugs Dermatol 15: 843–848. |
| [63] |
Gupta A, Keshri GK, Yadav A, et al. (2015) Superpulsed (Ga-As, 904 nm) low-level laser therapy (LLLT) attenuates inflammatory response and enhances healing of burn wounds. J Biophotonics 8: 489–501. doi: 10.1002/jbio.201400058
|
| [64] |
Weylandt KH, Chiu CY, Gomolka B, et al. (2012) Omega-3 fatty acids and their lipid mediators: towards an understanding of resolvin and protectin formation. Prostag Oth Lipid M 97: 73–82. doi: 10.1016/j.prostaglandins.2012.01.005
|
| [65] |
Tang Y, Zhang MJ, Hellmann J, et al. (2013) Proresolution therapy for the treatment of delayed healing of diabetic wounds. Diabetes 62: 618–627. doi: 10.2337/db12-0684
|
| [66] |
Bohr S, Patel SJ, Sarin D, et al. (2013) Resolvin D2 prevents secondary thrombosis and necrosis in a mouse burn wound model. Wound Repair Regen 21: 35–43. doi: 10.1111/j.1524-475X.2012.00853.x
|
| [67] |
Castano AP, Dai T, Yaroslavsky I, et al. (2007) Low-level laser therapy for zymosan-induced arthritis in rats: Importance of illumination time. Lasers Surg Med 39: 543–550. doi: 10.1002/lsm.20516
|
| [68] |
Moriyama Y, Moriyama EH, Blackmore K, et al. (2005) In vivo study of the inflammatory modulating effects of low-level laser therapy on iNOS expression using bioluminescence imaging. Photochem Photobiol 81: 1351–1355. doi: 10.1562/2005-02-28-RA-450
|
| [69] |
Pallotta RC, Bjordal JM, Frigo L, et al. (2012) Infrared (810-nm) low-level laser therapy on rat experimental knee inflammation. Lasers Med Sci 27: 71–78. doi: 10.1007/s10103-011-0906-1
|
| [70] | Ferraresi C, Hamblin MR, Parizotto NA (2012) Low-level laser (light) therapy (LLLT) on muscle tissue: performance, fatigue and repair benefited by the power of light. Photonics Lasers Med 1: 267–286. |
| [71] | Ferraresi C, Huang YY, Hamblin MR (2016) Photobiomodulation in human muscle tissue: an advantage in sports performance? J Biophotonics. |
| [72] |
Ferraresi C, de Sousa MV, Huang YY, et al. (2015) Time response of increases in ATP and muscle resistance to fatigue after low-level laser (light) therapy (LLLT) in mice. Lasers Med Sci 30: 1259–1267. doi: 10.1007/s10103-015-1723-8
|
| [73] |
Silveira PC, Scheffer Dda L, Glaser V, et al. (2016) Low-level laser therapy attenuates the acute inflammatory response induced by muscle traumatic injury. Free Radic Res 50: 503–513. doi: 10.3109/10715762.2016.1147649
|
| [74] |
Pires de Sousa MV, Ferraresi C, Kawakubo M, et al. (2016) Transcranial low-level laser therapy (810 nm) temporarily inhibits peripheral nociception: photoneuromodulation of glutamate receptors, prostatic acid phophatase, and adenosine triphosphate. Neurophotonics 3: 015003. doi: 10.1117/1.NPh.3.1.015003
|
| [75] |
de Sousa MV, Ferraresi C, de Magalhaes AC, et al. (2014) Building, testing and validating a set of home-made von Frey filaments: A precise, accurate and cost effective alternative for nociception assessment. J Neurosci Methods 232: 1–5. doi: 10.1016/j.jneumeth.2014.04.017
|
| [76] | Kobiela Ketz A, Byrnes KR, Grunberg NE, et al. (2016) Characterization of Macrophage/Microglial activation and effect of photobiomodulation in the spared nerve injury model of neuropathic pain. Pain Med: pnw144. |
| [77] |
Decosterd I, Woolf CJ (2000) Spared nerve injury: an animal model of persistent peripheral neuropathic pain. Pain 87: 149–158. doi: 10.1016/S0304-3959(00)00276-1
|
| [78] |
de Lima FM, Vitoretti L, Coelho F, et al. (2013) Suppressive effect of low-level laser therapy on tracheal hyperresponsiveness and lung inflammation in rat subjected to intestinal ischemia and reperfusion. Lasers Med Sci 28: 551–564. doi: 10.1007/s10103-012-1088-1
|
| [79] |
Silva VR, Marcondes P, Silva M, et al. (2014) Low-level laser therapy inhibits bronchoconstriction, Th2 inflammation and airway remodeling in allergic asthma. Respir Physiol Neurobiol 194: 37–48. doi: 10.1016/j.resp.2014.01.008
|
| [80] | Rigonato-Oliveira N, Brito A, Vitoretti L, et al. (2017) Effect of low-level laser therapy on chronic lung inflammation in experimental model of asthma: A comparative study of doses. Lasers Surg Med 49: 36. |
| [81] |
Huang YY, Gupta A, Vecchio D, et al. (2012) Transcranial low level laser (light) therapy for traumatic brain injury. J Biophotonics 5: 827–837. doi: 10.1002/jbio.201200077
|
| [82] |
Thunshelle C, Hamblin MR (2016) Transcranial low-level laser (light) therapy for brain injury. Photomed Laser Surg 34: 587–598. doi: 10.1089/pho.2015.4051
|
| [83] |
Hamblin MR (2016) Shining light on the head: Photobiomodulation for brain disorders. BBA Clin 6: 113–124. doi: 10.1016/j.bbacli.2016.09.002
|
| [84] |
Khuman J, Zhang J, Park J, et al. (2012) Low-level laser light therapy improves cognitive deficits and inhibits microglial activation after controlled cortical impact in mice. J Neurotrauma 29: 408–417. doi: 10.1089/neu.2010.1745
|
| [85] |
Veronez S, Assis L, Del Campo P, et al. (2017) Effects of different fluences of low-level laser therapy in an experimental model of spinal cord injury in rats. Lasers Med Sci 32: 343–349. doi: 10.1007/s10103-016-2120-7
|
| [86] |
Muili KA, Gopalakrishnan S, Eells JT, et al. (2013) Photobiomodulation induced by 670 nm light ameliorates MOG35-55 induced EAE in female C57BL/6 mice: a role for remediation of nitrosative stress. PLoS One 8: e67358. doi: 10.1371/journal.pone.0067358
|
| [87] |
Yoshimura TM, Sabino CP, Ribeiro MS (2016) Photobiomodulation reduces abdominal adipose tissue inflammatory infiltrate of diet-induced obese and hyperglycemic mice. J Biophotonics 9: 1255–1262. doi: 10.1002/jbio.201600088
|
| [88] |
Bjordal JM, Lopes-Martins RA, Iversen VV (2006) A randomised, placebo controlled trial of low level laser therapy for activated Achilles tendinitis with microdialysis measurement of peritendinous prostaglandin E2 concentrations. Br J Sports Med 40: 76–80. doi: 10.1136/bjsm.2005.020842
|
| [89] |
Hofling DB, Chavantes MC, Juliano AG, et al. (2010) Low-level laser therapy in chronic autoimmune thyroiditis: a pilot study. Lasers Surg Med 42: 589–596. doi: 10.1002/lsm.20941
|
| [90] |
Hofling DB, Chavantes MC, Juliano AG, et al. (2013) Low-level laser in the treatment of patients with hypothyroidism induced by chronic autoimmune thyroiditis: a randomized, placebo-controlled clinical trial. Lasers Med Sci 28: 743–753. doi: 10.1007/s10103-012-1129-9
|
| [91] | Hofling DB, Chavantes MC, Juliano AG, et al. (2012) Assessment of the effects of low-level laser therapy on the thyroid vascularization of patients with autoimmune hypothyroidism by color Doppler ultrasound. ISRN Endocrinol 2012: 126720. |
| [92] |
Hofling DB, Chavantes MC, Acencio MM, et al. (2014) Effects of low-level laser therapy on the serum TGF-beta1 concentrations in individuals with autoimmune thyroiditis. Photomed Laser Surg 32: 444–449. doi: 10.1089/pho.2014.3716
|
| [93] | Hofling D, Chavantes MC, Buchpiguel CA, et al. (2017) Long-term follow-up of patients with hypothyroidism induced by autoimmune thyroiditis submitted to low-level laser therapy. Lasers Surg Med 49: 36. |
| [94] | Ferraresi C, Beltrame T, Fabrizzi F, et al. (2015) Muscular pre-conditioning using light-emitting diode therapy (LEDT) for high-intensity exercise: a randomized double-blind placebo-controlled trial with a single elite runner. Physiother Theory Pract: 1–8. |
| [95] |
Ferraresi C, Dos Santos RV, Marques G, et al. (2015) Light-emitting diode therapy (LEDT) before matches prevents increase in creatine kinase with a light dose response in volleyball players. Lasers Med Sci 30: 1281–1287. doi: 10.1007/s10103-015-1728-3
|
| [96] |
Pinto HD, Vanin AA, Miranda EF, et al. (2016) Photobiomodulation therapy improves performance and accelerates recovery of high-level rugby players in field test: A randomized, crossover, double-blind, placebo-controlled clinical study. J Strength Cond Res 30: 3329–3338. doi: 10.1519/JSC.0000000000001439
|
| [97] |
Ferraresi C, Bertucci D, Schiavinato J, et al. (2016) Effects of light-emitting diode therapy on muscle hypertrophy, gene expression, performance, damage, and delayed-onset muscle soreness: case-control study with a pair of identical twins. Am J Phys Med Rehabil 95: 746–757. doi: 10.1097/PHM.0000000000000490
|
| [98] | Johnston A, Xing X, Wolterink L, et al. (2016) IL-1 and IL-36 are dominant cytokines in generalized pustular psoriasis. J Allergy Clin Immunol. |
| [99] |
Ablon G (2010) Combination 830-nm and 633-nm light-emitting diode phototherapy shows promise in the treatment of recalcitrant psoriasis: preliminary findings. Photomed Laser Surg 28: 141–146. doi: 10.1089/pho.2009.2484
|
| [100] |
Choi M, Na SY, Cho S, et al. (2011) Low level light could work on skin inflammatory disease: a case report on refractory acrodermatitis continua. J Korean Med Sci 26: 454–456. doi: 10.3346/jkms.2011.26.3.454
|
| [101] |
Hamblin MR (2013) Can osteoarthritis be treated with light? Arthritis Res Ther 15: 120. doi: 10.1186/ar4354
|
| [102] |
Ip D (2015) Does addition of low-level laser therapy (LLLT) in conservative care of knee arthritis successfully postpone the need for joint replacement? Lasers Med Sci 30: 2335–2339. doi: 10.1007/s10103-015-1814-6
|
| [103] | Brosseau L, Robinson V, Wells G, et al. (2005) Low level laser therapy (Classes I, II and III) for treating rheumatoid arthritis. Cochrane Database Syst Rev 19: CD002049. |
| [104] | Brosseau L, Welch V, Wells G, et al. (2004) Low level laser therapy (Classes I, II and III) for treating osteoarthritis. Cochrane Database Syst Rev: CD002046. |
| [105] |
Barabas K, Bakos J, Zeitler Z, et al. (2014) Effects of laser treatment on the expression of cytosolic proteins in the synovium of patients with osteoarthritis. Lasers Surg Med 46: 644–649. doi: 10.1002/lsm.22268
|
| [106] | Gregoriou S, Papafragkaki D, Kontochristopoulos G, et al. (2010) Cytokines and other mediators in alopecia areata. Mediators Inflamm 2010: 928030. |
| [107] |
Avci P, Gupta GK, Clark J, et al. (2014) Low-level laser (light) therapy (LLLT) for treatment of hair loss. Lasers Surg Med 46: 144-151. doi: 10.1002/lsm.22170
|
| [108] |
Gupta AK, Foley KA (2017) A critical assessment of the evidence for low-level laser therapy in the treatment of hair loss. Dermatol Surg 43: 188–197. doi: 10.1097/DSS.0000000000000904
|
| [109] |
Yamazaki M, Miura Y, Tsuboi R, et al. (2003) Linear polarized infrared irradiation using Super Lizer is an effective treatment for multiple-type alopecia areata. Int J Dermatol 42: 738–740. doi: 10.1046/j.1365-4362.2003.01968.x
|
Figures(7)

Michael R Hamblin. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation[J]. AIMS Biophysics, 2017, 4(3): 337-361. doi: 10.3934/biophy.2017.3.337







 DownLoad:
DownLoad: