The data input process for most chest pain centers is not intelligent, requiring a lot of staff to manually input patient information. This leads to problems such as long processing times, high potential for errors, an inability to access patient data in a timely manner and an increasing workload. To address the challenge, an Internet of Things (IoT)-driven chest pain center is designed, which crosses the sensing layer, network layer and application layer. The system enables the construction of intelligent chest pain management through a pre-hospital app, Ultra-Wideband (UWB) positioning, and in-hospital treatment. The pre-hospital app is provided to emergency medical services (EMS) centers, which allows them to record patient information in advance and keep it synchronized with the hospital's database, reducing the time needed for treatment. UWB positioning obtains the patient's hospital information through the zero-dimensional base station and the corresponding calculation engine, and in-hospital treatment involves automatic acquisition of patient information through web and mobile applications. The system also introduces the Bidirectional Long Short-Term Memory (BiLSTM)-Conditional Random Field (CRF)-based algorithm to train electronic medical record information for chest pain patients, extracting the patient's chest pain clinical symptoms. The resulting data are saved in the chest pain patient database and uploaded to the national chest pain center. The system has been used in Liaoning Provincial People's Hospital, and its subsequent assistance to doctors and nurses in collaborative treatment, data feedback and analysis is of great significance.
Citation: Feng Li, Zhongao Bi, Hongzeng Xu, Yunqi Shi, Na Duan, Zhaoyu Li. Design and implementation of a smart Internet of Things chest pain center based on deep learning[J]. Mathematical Biosciences and Engineering, 2023, 20(10): 18987-19011. doi: 10.3934/mbe.2023840
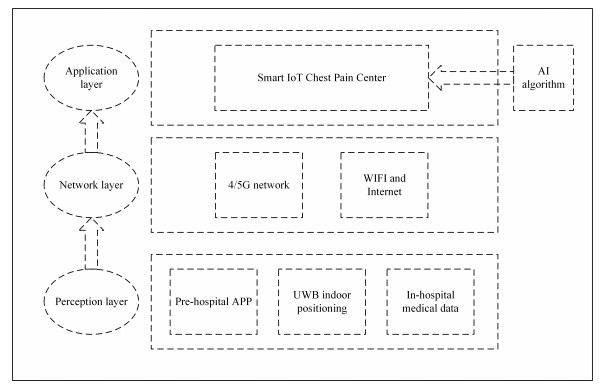
The data input process for most chest pain centers is not intelligent, requiring a lot of staff to manually input patient information. This leads to problems such as long processing times, high potential for errors, an inability to access patient data in a timely manner and an increasing workload. To address the challenge, an Internet of Things (IoT)-driven chest pain center is designed, which crosses the sensing layer, network layer and application layer. The system enables the construction of intelligent chest pain management through a pre-hospital app, Ultra-Wideband (UWB) positioning, and in-hospital treatment. The pre-hospital app is provided to emergency medical services (EMS) centers, which allows them to record patient information in advance and keep it synchronized with the hospital's database, reducing the time needed for treatment. UWB positioning obtains the patient's hospital information through the zero-dimensional base station and the corresponding calculation engine, and in-hospital treatment involves automatic acquisition of patient information through web and mobile applications. The system also introduces the Bidirectional Long Short-Term Memory (BiLSTM)-Conditional Random Field (CRF)-based algorithm to train electronic medical record information for chest pain patients, extracting the patient's chest pain clinical symptoms. The resulting data are saved in the chest pain patient database and uploaded to the national chest pain center. The system has been used in Liaoning Provincial People's Hospital, and its subsequent assistance to doctors and nurses in collaborative treatment, data feedback and analysis is of great significance.

| [1] |
L. Ma, Z. Wang, J. Fan, S. Hu, An essential introduction to the annual report on cardiovascular health and diseases in china (2021) (in Chinese), Chin. Gen. Pract., 25 (2022), 3331–3346. https://doi.org/10.12114/j.issn.1007-9572.2022.0506 doi: 10.12114/j.issn.1007-9572.2022.0506

|
| [2] |
W. Wang, X. Yu, B. Fang, D. Y. Zhao, Y. Chen, W. Wei, et al., Cross-modality lge-cmr segmentation using image-to-image translation based data augmentatio, IEEE/ACM Trans. Comput. Biol. Bioinf., 20 (2023), 2367–2375. https://doi.org/10.1109/TCBB.2022.3140306 doi: 10.1109/TCBB.2022.3140306
|
| [3] |
Y. Duan, S. Tang, Observation on the effect of bian quefei rescue remote first aid system in pre-hospital first aid for patients with chest pain (in Chinese), Chin. Med. Equip., 14 (2017), 83–86. https://doi.org/10.3969/J.ISSN.1672-8270.2017.10.024 doi: 10.3969/J.ISSN.1672-8270.2017.10.024
|
| [4] |
S. Ding, J. Xiong, Y. Zhang, Y. Zhao, H. Zhang, Y. Xu, Clinical application of time management system in chest pain center (in Chinese), Intern. Med. Theory Pract., 16 (2021), 202–204. https://doi.org/10.16138/j.1673-6087.2021.03.013 doi: 10.16138/j.1673-6087.2021.03.013
|
| [5] |
H. V. Denysyuk, R. J. Pinto, P. M. Silva, R. P. Duarte, F. A. Marinho, L. Pimenta, et al., Algorithms for automated diagnosis of cardiovascular diseases based on ECG data: A comprehensive systematic review, Heliyon, 9 (2023), e13601. https://doi.org/10.1016/j.heliyon.2023.e13601 doi: 10.1016/j.heliyon.2023.e13601
|
| [6] |
H. Costa, C. A. Costa, R. S. Antunes, R. D. R. Righi, P. A. Crocker, V. R. Q. Leithardt, et al., ID-Care: A model for sharing wide healthcare data, IEEE Access, 11 (2023), 33455–33469. https://doi.org/10.1109/ACCESS.2023.3249109 doi: 10.1109/ACCESS.2023.3249109
|
| [7] | H. Chen, D. Xiang, W. Qin, M. Zhou, Y. Tian, J. Liu, et al., A study of regional cooperative emergency care system for st-elevation myocardial infarction patients based on the internet of things, in 2012 IEEE 14th International Conference on e-Health Networking, Applications and Services (Healthcom), (2012), 73–77. https://doi.org/10.1109/HealthCom.2012.6380069 |
| [8] | H. Chen, D. Xiang, W. Qin, M. Zhou, J. Yang, J. Liu, et al., Optimal st-elevation myocardial infarction system by regional cooperative emergency care based on the internet of things, in Smart Health, Springer, (2014), 225–232. https://doi.org/10.1007/978-3-319-08416-9_24 |
| [9] |
Y. Cao, S. Miraba, S. Rafiei, A. Ghabussi, F. Bokaei, S. Baharom, et al., Economic application of structural health monitoring and internet of things in efficiency of building information modeling, Smart Struct. Syst., 26 (2020), 559–573. https://doi.org/10.12989/sss.2020.26.5.559 doi: 10.12989/sss.2020.26.5.559
|
| [10] |
R. Ma, M. Karimzadeh, A. Ghabussi, Y. Zandi, S. Baharom, A. Selmi, et al., Assessment of composite beam performance using GWO–ELM metaheuristic algorithm, Eng. Comput., 38 (2021), 2083–2099. https://doi.org/10.1007/s00366-021-01363-1 doi: 10.1007/s00366-021-01363-1
|
| [11] |
A. Morasaei, A. Ghabussi, S. Aghlmand, M. Yazdani, S. Baharom, H. Assilzade, Simulation of steel–concrete composite floor system behavior at elevated temperatures via multi-hybrid metaheuristic framework, Eng. Comput., 38 (2022), 2567–2582. https://doi.org/10.1007/s00366-020-01228-z doi: 10.1007/s00366-020-01228-z
|
| [12] |
K. Tajziehchi, A. Ghabussi, H. Alizadeh, Control and optimization against earthquake by using genetic algorithm, J. Appl. Eng. Sci., 8 (2018), 73–78. https://doi.org/10.2478/jaes-2018-0010 doi: 10.2478/jaes-2018-0010
|
| [13] |
D. Xiang, S. Yi, Chest pain centers in china: current status and prospects, Cardiol. Plus, 2 (2017), 18–21. https://doi.org/10.4103/2470-7511.248469 doi: 10.4103/2470-7511.248469
|
| [14] |
Q. Xiao, M. Zhou, Y. Tian, Informatization construction and practice of chest pain center (in Chinese), China Digital Med., 2015 (2015), 17–18. https://doi.org/10.3969/j.issn.1673-7571.2015.09.006 doi: 10.3969/j.issn.1673-7571.2015.09.006
|
| [15] |
B. G. Choi, J. Y. Park, S. W. Rha, Y. K. Noh, Pre-test probability for coronary artery disease in patients with chest pain based on machine learning techniques, Int. J. Cardiol., 385 (2023), 85–93. https://doi.org/10.1016/j.ijcard.2023.05.041 doi: 10.1016/j.ijcard.2023.05.041
|
| [16] |
H. Zhou, W. Feng, H. Li, L. Jin, L. Qian, X. Zhu, et al., Effect evaluation and quality control strategy of grassroots chest pain center construction (in Chinese), Chin. J. Gen. Pract., 19 (2020), 434–437. https://doi.org/10.3760/cma.j.cn114798-20200312-00280 doi: 10.3760/cma.j.cn114798-20200312-00280
|
| [17] |
Y. Han, S. Sun, B. Qiao, H. Liu, C. Zhang, B. Wang, et al., Timing of angiography and outcomes in patients with non-st-segment elevation myocardial infarction: insights from the evaluation and management of patients with acute chest pain in china registry, Front. Cardiovasc. Med., 9 (2022), 1000554. https://doi.org/10.3389/fcvm.2022.1000554 doi: 10.3389/fcvm.2022.1000554
|
| [18] |
F. Fan, Y. Li, Y. Zhang, J. Li, J. Liu, H. Hao, et al., Deep learning-based classification of mesothelioma improves prediction of patient outcome, J. Am. Heart Assoc., 8 (2019), e013384. https://doi.org/10.1161/JAHA.119.013384 doi: 10.1161/JAHA.119.013384
|
| [19] |
J. Li, X. Li, Q. Wang, S. Hu, Y. Wang, F. A. Masoudi, et al., ST-segment elevation myocardial infarction in china from 2001 to 2011 (the china peace-retrospective acute myocardial infarction study): a retrospective analysis of hospital data, The Lancet, 385 (2015), 441–451. https://doi.org/10.1016/S0140-6736(14)60921-1 doi: 10.1016/S0140-6736(14)60921-1
|
| [20] |
W. B. Gibler, J. P. Runyon, R. C. Levy, M. R. Sayre, R. Kacich, C. R. Hattemer, et al., A rapid diagnostic and treatment center for patients with chest pain in the emergency department, Annals of emergency medicine, 25 (1995), 1–8. https://doi.org/10.1016/S0196-0644(95)70347-0 doi: 10.1016/S0196-0644(95)70347-0
|
| [21] |
K. Tang, Z. Shuai, Z. Li, L. Zhou, J. Gou, Y. Wang, et al., Research status of biomarkers of acute coronary syndrome, Chin. J. Arterioscler., 29 (2021), 451–455. https://doi.org/10.3969/j.issn.1007-3949.2021.05.016 doi: 10.3969/j.issn.1007-3949.2021.05.016
|
| [22] |
J. Liu, D. Zhao, Q. Zhang, Recent hospitalization trends for acute myocardial infarction in Beijing, Eur. Heart J., 37 (2016), 3188–3189. https://doi.org/10.1093/eurheartj/ehw472 doi: 10.1093/eurheartj/ehw472
|
| [23] |
L. Li, J. Zhao, L. Hou, Y. Zhai, J. Shi, F. Cui, An attention-based deep learning model for clinical named entity recognition of Chinese electronic medical records, BMC Med. Inf. Decis. Making, 19 (2019), 1–11. https://doi.org/10.1186/s12911-019-0933-6 doi: 10.1186/s12911-019-0933-6
|
| [24] |
J. Yu, X. Kang, C. Bai, H. Liu, A new text retrieval model for chinese electronic medical records (in Chinese), Comput. Sci., 49 (2022), 32–38. https://doi.org/10.11896/jsjkx.210400198 doi: 10.11896/jsjkx.210400198
|
| [25] |
K. Xu, Z. Yang, P. Kang, Q. Wang, W. Liu, Document-level attention-based bilstm-crf incorporating disease dictionary for disease named entity recognition, Comput. Biol. Med., 108 (2019), 122–132. https://doi.org/10.1016/j.compbiomed.2019.04.002 doi: 10.1016/j.compbiomed.2019.04.002
|
| [26] |
Q. Wan, J. Liu, L. Wei, B. Ji, A self-attention based neural architecture for Chinese medical named entity recognition, Math. Biosci. Eng., 17 (2020), 3498–3511. https://doi.org/10.3934/mbe.2020197 doi: 10.3934/mbe.2020197
|
| [27] |
Z. Long, W. Liu, Z. Zhao, S. Tong, L. Wang, M. Zhou, et al., Case fatality rate of patients with acute myocardial infarction in 253 chest pain centers—china, 2019–2020, China CDC Weekly, 4 (2022), 518–521. https://doi.org/10.46234/ccdcw2022.026 doi: 10.46234/ccdcw2022.026
|
| [28] |
D. C. Xiang, Y. Z. Jin, W. Y. Fang, X. Su, B. Yu, Y. Wang, et al., The national chest pain centers program: Monitoring and improving quality of care for patients with acute chest pain in China, Cardiol. Plus, 6 (2021), 187–197. https://doi.org/10.4103/2470-7511.327239 doi: 10.4103/2470-7511.327239
|
| [29] |
F. Tong, C. Wang, S. Han, Y. Li, Z. Li, Z. Sun, Differential risk assessment of acute aortic syndrome with chest pain onset less than 3 hours and non-st-segment elevation myocardial infarction (in Chinese), Chin. J. Arterioscler., 8 (2021), 681–687. https://doi.org/10.3969/j.issn.1007-3949.2021.08.006 doi: 10.3969/j.issn.1007-3949.2021.08.006
|
| [30] |
J. Chen, Z. Guo, X. Xu, L. Zhang, Y. Teng, Y. Chen, et al., A robust deep learning framework based on spectrograms for Heart sound classification, IEEE/ACM Trans. Comput. Biol. Bioinf., 2023 (2023), 1–12. https://doi.org/10.1109/TCBB.2023.3247433 doi: 10.1109/TCBB.2023.3247433
|
| [31] |
J. Chen, S. Sun, L. Zhang, B. Yang, W. Wang, Compressed sensing framework for heart sound acquisition in internet of medical things, IEEE Trans. Ind. Inf., 18 (2021), 2000–2009. https://doi.org/10.1109/TII.2021.3088465 doi: 10.1109/TII.2021.3088465
|
| [32] |
J. Wang, C. J. Rao, M. Goh, X. P. Xiao, Risk assessment of coronary heart disease based on cloud-random forest, Artif. Intell. Rev., 56 (2023), 203–232. https://doi.org/10.1007/s10462-022-10170-z doi: 10.1007/s10462-022-10170-z
|











Figures(12) / Tables(7)

Feng Li, Zhongao Bi, Hongzeng Xu, Yunqi Shi, Na Duan, Zhaoyu Li. Design and implementation of a smart Internet of Things chest pain center based on deep learning[J]. Mathematical Biosciences and Engineering, 2023, 20(10): 18987-19011. doi: 10.3934/mbe.2023840







 DownLoad:
DownLoad: