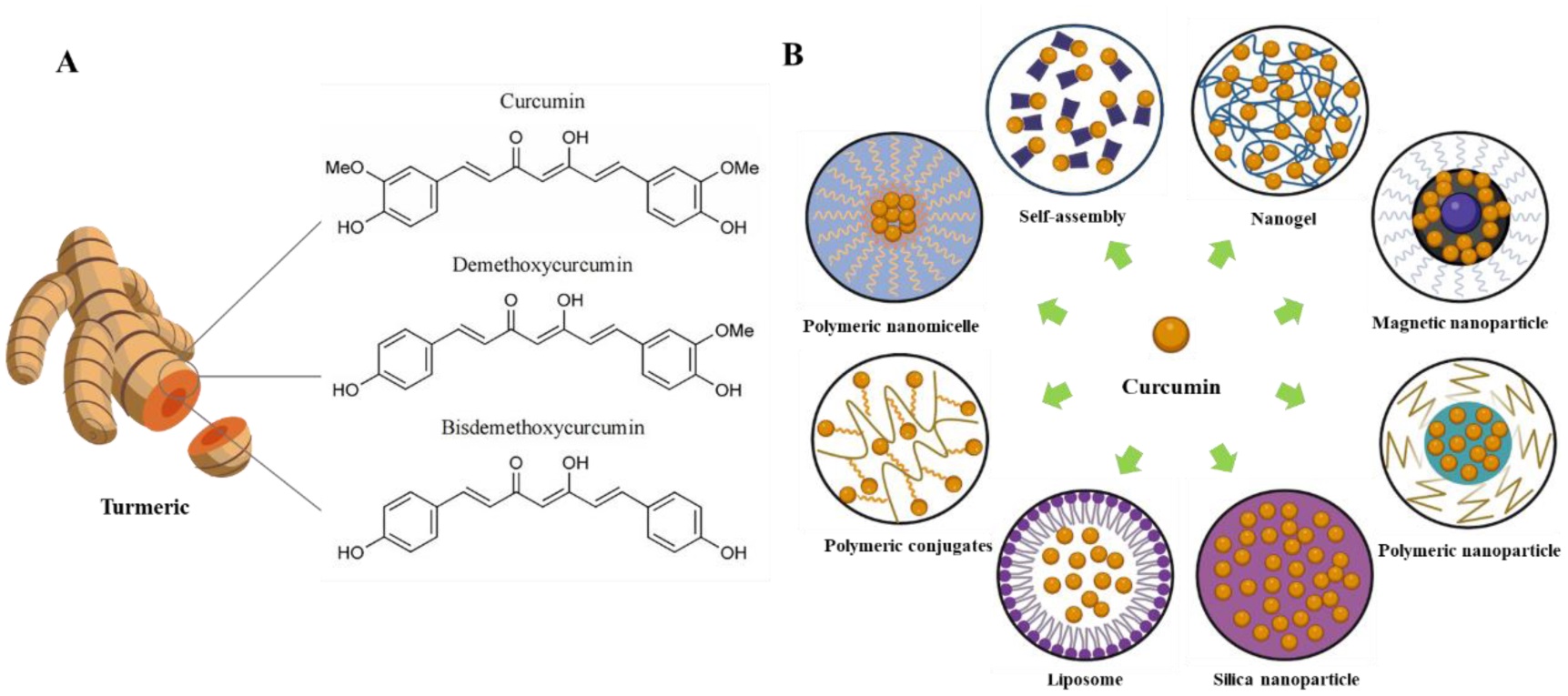
Curcumin (CUR) a natural polyphenolic compound, has attracted significant attention due to its broad-spectrum anti-inflammatory, antioxidant, antimicrobial, and antitumor activities. However, its poor water solubility, low bioavailability, and limited stability have hindered clinical applications. Novel approaches utilizing nanocarrier-based delivery systems (e.g., liposomes, micelles) and structural modification strategies offer promising solutions to enhance the therapeutic efficacy of curcumin. This review and analysis attempted to summarize the therapeutical applications and working mechanisms of CUR in oral infectious diseases, inflammation, traumatic disease and immune disorder. Publications included in this review included references were confined to curcumin, nano-curcumin (nCUR), and the names of different oral diseases; the different methodologies included clinical trials, in vivo animal studies and in vitro studies. Web of Science and Pubmed/MEDLINE databases were explored. The antioxidant, anti-inflammatory, immune regulation and anticancer properties of CUR and nCUR are reported, and their positive applications in oral diseases is discussed. With more favorable structure and improved solubility and bioavailability, nCUR is more beneficial, stable and efficient than CUR. Local application seems to be more effective on oral diseases, which allows for higher concentrations and better bioavailability, and can directly targets specific areas of the mouth, providing more precise treatment. Both CUR and nCUR are likely to be developed into a next-generation drug, but there is no consensus on their concentration, irradiation times and light intensity. Additional trials are required to obtain clinical standards, and establish specific dose ranges and clinical procedures.
Citation: Juan Zhang, Yuhan Peng, Siting Hu, Jianmeng Xu, Chengcheng Yu, Lei Hua, Shihui Zhou, Qi Liu. Therapeutic application of curcumin and its nanoformulation in dentistry: Opportunities and challenges[J]. AIMS Molecular Science, 2025, 12(2): 148-172. doi: 10.3934/molsci.2025010
Curcumin (CUR) a natural polyphenolic compound, has attracted significant attention due to its broad-spectrum anti-inflammatory, antioxidant, antimicrobial, and antitumor activities. However, its poor water solubility, low bioavailability, and limited stability have hindered clinical applications. Novel approaches utilizing nanocarrier-based delivery systems (e.g., liposomes, micelles) and structural modification strategies offer promising solutions to enhance the therapeutic efficacy of curcumin. This review and analysis attempted to summarize the therapeutical applications and working mechanisms of CUR in oral infectious diseases, inflammation, traumatic disease and immune disorder. Publications included in this review included references were confined to curcumin, nano-curcumin (nCUR), and the names of different oral diseases; the different methodologies included clinical trials, in vivo animal studies and in vitro studies. Web of Science and Pubmed/MEDLINE databases were explored. The antioxidant, anti-inflammatory, immune regulation and anticancer properties of CUR and nCUR are reported, and their positive applications in oral diseases is discussed. With more favorable structure and improved solubility and bioavailability, nCUR is more beneficial, stable and efficient than CUR. Local application seems to be more effective on oral diseases, which allows for higher concentrations and better bioavailability, and can directly targets specific areas of the mouth, providing more precise treatment. Both CUR and nCUR are likely to be developed into a next-generation drug, but there is no consensus on their concentration, irradiation times and light intensity. Additional trials are required to obtain clinical standards, and establish specific dose ranges and clinical procedures.

| [1] |
Kotha RR, Luthria DL (2019) Curcumin: Biological, pharmaceutical, nutraceutical, and analytical aspects. Molecules 24: 2930. https://doi.org/10.3390/molecules24162930 
|
| [2] |
Priyadarsini KI (2014) The chemistry of curcumin: From extraction to therapeutic agent. Molecules 19: 20091-20112. https://doi.org/10.3390/molecules191220091
|
| [3] |
Nelson KM, Dahlin JL, Bisson J, et al. (2017) The essential medicinal chemistry of curcumin. J Med Chem 60: 1620-1637. https://doi.org/10.1021/acs.jmedchem.6b00975
|
| [4] |
Salehi B, Stojanović-Radić Z, Matejić J, et al. (2019) The therapeutic potential of curcumin: A review of clinical trials. Eur J Med Chem 163: 527-545. https://doi.org/10.1016/j.ejmech.2018.12.016
|
| [5] |
Yeung AWK, Horbańczuk M, Tzvetkov NT, et al. (2019) Curcumin: Total-scale analysis of the scientific literature. Molecules 24: 1393. https://doi.org/10.3390/molecules24071393
|
| [6] |
Li H, Sureda A, Devkota HP, et al. (2020) Curcumin, the golden spice in treating cardiovascular diseases. Biotechnol Adv 38: 107343. https://doi.org/10.1016/j.biotechadv.2019.01.010
|
| [7] |
Kwiecien S, Magierowski M, Majka J, et al. (2019) Curcumin: A potent protectant against esophageal and gastric disorders. Int J Mol Sci 20: 1477. https://doi.org/10.3390/ijms20061477
|
| [8] | Heidari S, Mahdiani S, Hashemi M, et al. (2020) Recent advances in neurogenic and neuroprotective effects of curcumin through the induction of neural stem cells. Biotechnol Appl Biochem 67: 430-441. https://doi.org/10.1002/bab.1891 |
| [9] |
Scazzocchio B, Minghetti L, D'Archivio M, et al. (2020) Interaction between gut microbiota and curcumin: A new key of understanding for the health effects of curcumin. Nutrients 12: 2499. https://doi.org/10.3390/nu12092499
|
| [10] |
Chen Y, Lu Y, Lee RJ, et al. (2020) Nano encapsulated curcumin: And its potential for biomedical applications. Int J Nanomedicine 15: 3099-3120. https://doi.org/10.2147/IJN.S210320
|
| [11] |
Kabir MT, Rahman MH, Akter R, et al. (2021) Potential role of curcumin and its nanoformulations to treat various types of cancers. Biomolecules 11: 392. https://doi.org/10.3390/biom11030392
|
| [12] |
Tagde P, Tagde P, Islam F, et al. (2021) The multifaceted role of curcumin in advanced nanocurcumin form in the treatment and management of chronic disorders. Molecules 26: 7109. https://doi.org/10.3390/molecules26237109
|
| [13] |
Tang W, Du M, Zhang S, et al. (2021) Therapeutic effect of curcumin on oral diseases: A literature review. Phytother Res 35: 2287-2295. https://doi.org/10.1002/ptr.6943
|
| [14] |
Sharifi S, Fathi N, Memar MY, et al. (2020) Anti-microbial activity of curcumin nanoformulations: New trends and future perspectives. Phytother Res 34: 1926-1946. https://doi.org/10.1002/ptr.6658
|
| [15] |
Kumbar VM, Peram MR, Kugaji MS, et al. (2021) Effect of curcumin on growth, biofilm formation and virulence factor gene expression of Porphyromonas gingivalis. Odontology 109: 18-28. https://doi.org/10.1007/s10266-020-00514-y
|
| [16] |
Soares JM, Yakovlev VV, Blanco KC, et al. (2024) Photodynamic inactivation and its effects on the heterogeneity of bacterial resistance. Sci Rep 14: 28268. https://doi.org/10.1038/s41598-024-79743-y
|
| [17] | Sha AM, Garib BT (2019) Antibacterial effect of curcumin against clinically isolated Porphyromonas gingivalis and connective tissue reactions to curcumin gel in the subcutaneous tissue of rats. Biomed Res Int 2019: 6810936. https://doi.org/10.1155/2019/6810936 |
| [18] |
Adeyemi OS, Obeme-Imom JI, Akpor BO, et al. (2020) Altered redox status, DNA damage and modulation of L-tryptophan metabolism contribute to antimicrobial action of curcumin. Heliyon 6: e03495. https://doi.org/10.1016/j.heliyon.2020.e03495
|
| [19] |
Trigo-Gutierrez JK, Vega-Chacón Y, Soares AB, et al. (2021) Antimicrobial activity of curcumin in nanoformulations: A comprehensive review. Int J Mol Sci 22: 7130. https://doi.org/10.3390/ijms22137130
|
| [20] | Teow SY, Liew K, Ali SA, et al. (2016) Antibacterial action of curcumin against staphylococcus aureus: A brief review. J Trop Med 2016: 2853045. https://doi.org/10.1155/2016/28530 |
| [21] |
Wray R, Iscla I, Blount P (2021) Curcumin activation of a bacterial mechanosensitive channel underlies its membrane permeability and adjuvant properties. PLoS Pathog 17: e1010198. https://doi.org/10.1371/journal.ppat.1010198
|
| [22] |
Javed F, Romanos GE (2013) Does photodynamic therapy enhance standard antibacterial therapy in dentistry?. Photomed Laser Surg 31: 512-518. https://doi.org/10.1089/pho.2012.3329
|
| [23] |
Alves LVGL, Curylofo-Zotti FA, Borsatto MC, et al. (2019) Influence of antimicrobial photodynamic therapy in carious lesion. Randomized split-mouth clinical trial in primary molars. Photodiagn Photodyn 26: 124-130. https://doi.org/10.1016/j.pdpdt.2019.02.018
|
| [24] |
Jia Q, Song Q, Li P, et al. (2019) Rejuvenated photodynamic therapy for bacterial infections. Adv Healthc Mater 8: e1900608. https://doi.org/10.1002/adhm.201900608
|
| [25] |
Saitawee D, Teerakapong A, Morales NP, et al. (2018) Photodynamic therapy of Curcuma longa extract stimulated with blue light against Aggregatibacter actinomycetemcomitans. Photodiagn Photodyn 22: 101-105. https://doi.org/10.1016/j.pdpdt.2018.03.001
|
| [26] |
Pan H, Wang D, Zhang F (2020) In vitro antimicrobial effect of curcumin-based photodynamic therapy on Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans. Photodiagn Photodyn 32: 102055. https://doi.org/10.1016/j.pdpdt.2020.102055
|
| [27] |
Zhang G, Yang Y, Shi J, et al. (2021) Near-infrared light II-assisted rapid biofilm elimination platform for bone implants at mild temperature. Biomaterials 269: 120634. https://doi.org/10.1016/j.biomaterials.2020.120634
|
| [28] |
Ferrisse TM, Dias LM, De Oliveira AB, et al. (2022) Efficacy of curcumin-mediated antibacterial photodynamic therapy for oral antisepsis: A systematic review and network meta-analysis of randomized clinical trials. Photodiagn Photodyn 39: 102876. https://doi.org/10.1016/j.pdpdt.2022.102876
|
| [29] |
Nima G, Soto-Montero J, Alves LA, et al. (2021) Photodynamic inactivation of Streptococcus mutans by curcumin in combination with EDTA. Dent Mater 37: e1-e14. https://doi.org/10.1016/j.dental.2020.09.015
|
| [30] |
Cusicanqui Méndez DA, Gutierres E, Dionisio EJ, et al. (2018) Curcumin-mediated antimicrobial photodynamic therapy reduces the viability and vitality of infected dentin caries microcosms. Photodiagn Photodyn 24: 102-108. https://doi.org/10.1016/j.pdpdt.2018.09.007
|
| [31] |
Girisa S, Kumar A, Rana V, et al. (2021) From simple mouth cavities to complex oral mucosal disorders-Curcuminoids as a promising therapeutic approach. ACS Pharmacol Transl Sci 4: 647-665. https://doi.org/10.1021/acsptsci.1c00017
|
| [32] |
Dashper SG, Liu SW, Walsh KA, et al. (2013) Streptococcus mutans biofilm disruption by κ-casein glycopeptide. J Dent 41: 521-527. https://doi.org/10.1016/j.jdent.2013.03.010
|
| [33] |
Pourhajibagher M, Omrani LR, Noroozian M, et al. (2021) In vitro antibacterial activity and durability of a nano-curcumin-containing pulp capping agent combined with antimicrobial photodynamic therapy. Photodiagn Photodyn 33: 102150. https://doi.org/10.1016/j.pdpdt.2020.102150
|
| [34] |
Méndez DAC, Gutierrez E, Lamarque GCC, et al. (2019) The effectiveness of curcumin-mediated antimicrobial photodynamic therapy depends on pre-irradiation and biofilm growth times. Photodiagn Photodyn 27: 474-480. https://doi.org/10.1016/j.pdpdt.2019.07.011
|
| [35] |
Wenzler JS, Wurzel SC, Falk W, et al. (2024) Bactericidal effect of different photochemical-based therapy options on implant surfaces-An in vitro Sstudy. J Clin Med 13: 4212. https://doi.org/10.3390/jcm13144212
|
| [36] |
Lamarque GCC, Méndez DAC, Matos AA, et al. (2021) In vitro effect of curcumin-mediated antimicrobial photodynamic therapy on fibroblasts: Viability and cell signaling for apoptosis. Lasers Med Sci 36: 1169-1175. https://doi.org/10.1007/s10103-020-03150-8
|
| [37] |
Sakko M, Tjäderhane L, Rautemaa-Richardson R (2016) Microbiology of root canal infections. Prim Dent J 5: 84-89. https://doi.org/10.1308/205016816819304231
|
| [38] |
Pileggi G, Wataha JC, Girard M, et al. (2013) Blue light-mediated inactivation of Enterococcus faecalis in vitro. Photodiag Photodyn 10: 134-140. https://doi.org/10.1016/j.pdpdt.2012.11.002
|
| [39] |
Neelakantan P, Cheng CQ, Ravichandran V, et al. (2015) Photoactivation of curcumin and sodium hypochlorite to enhance antibiofilm efficacy in root canal dentin. Photodiagn Photodyn 12: 108-114. https://doi.org/10.1016/j.pdpdt.2014.10.011
|
| [40] |
Guo Q, Li P, Zhang Y, et al. (2024) Polydopamine-curcumin coating of titanium for remarkable antibacterial activity via synergistic photodynamic and photothermal properties. Photochem Photobiol 100: 699-711. https://doi.org/10.1111/php.13870
|
| [41] | Pourhajibagher M, Chiniforush N, Monzavi A, et al. (2018) Inhibitory effects of antimicrobial photodynamic therapy with curcumin on biofilm-associated gene expression profile of aggregatibacter actinomycetemcomitans. J Dent (Tehran) 15: 169-177. |
| [42] |
Ivanaga CA, Miessi DMJ, Nuernberg MAA, et al. (2019) Antimicrobial photodynamic therapy (aPDT) with curcumin and LED, as an enhancement to scaling and root planing in the treatment of residual pockets in diabetic patients: A randomized and controlled split-mouth clinical trial. Photodiagn Photodyn 27: 388-395. https://doi.org/10.1016/j.pdpdt.2019.07.005
|
| [43] |
Böcher S, Wenzler JS, Falk W, et al. (2019) Comparison of different laser-based photochemical systems for periodontal treatment. Photodiagn Photodyn 27: 433-439. https://doi.org/10.1016/j.pdpdt.2019.06.009
|
| [44] |
Pérez-Pacheco CG, Fernandes NAR, Primo FL, et al. (2021) Local application of curcumin-loaded nanoparticles as an adjunct to scaling and root planing in periodontitis: Randomized, placebo-controlled, double-blind split-mouth clinical trial. Clin Oral Invest 25: 3217-3227. https://doi.org/10.1007/s00784-020-03652-3
|
| [45] |
Negahdari R, Ghavimi MA, Barzegar A, et al. (2021) Antibacterial effect of nanocurcumin inside the implant fixture: An in vitro study. Clin Exp Dent Res 7: 163-169. https://doi.org/10.1002/cre2.348
|
| [46] |
Mahdizade-Ari M, Pourhajibagher M, Bahador A (2019) Changes of microbial cell survival, metabolic activity, efflux capacity, and quorum sensing ability of Aggregatibacter actinomycetemcomitans due to antimicrobial photodynamic therapy-induced bystander effects. Photodiagn Photodyn 26: 287-294. https://doi.org/10.1016/j.pdpdt.2019.04.021
|
| [47] |
Narayanan VS, Muddaiah S, Shashidara R, et al. (2020) Variable antifungal activity of curcumin against planktonic and biofilm phase of different candida species. Indian J Dent Res 31: 145-148. https://doi.org/10.4103/ijdr.IJDR_521_17
|
| [48] |
Ambreen G, Duse L, Tariq I, et al. (2020) Sensitivity of papilloma virus-associated cell lines to photodynamic therapy with curcumin-loaded liposomes. Cancers 12: 3278. https://doi.org/10.3390/cancers12113278
|
| [49] |
Jordão CC, De Sousa TV, Klein MI, et al. (2020) Antimicrobial photodynamic therapy reduces gene expression of Candida albicans in biofilms. Photodiagn Photodyn 31: 101825. https://doi.org/10.1016/j.pdpdt.2020.101825
|
| [50] |
de Cassia Rodrigues Picco D, Cavalcante LLR, Trevisan RLB, et al. (2019) Effect of curcumin-mediated photodynamic therapy on Streptococcus mutans and Candida albicans: A systematic review of in vitro studies. Photodiagn Photodyn 27: 455-461. https://doi.org/10.1016/j.pdpdt.2019.07.010
|
| [51] |
Anwar SK, Elmonaem SNA, Moussa E, et al. (2023) Curcumin nanoparticles: The topical antimycotic suspension treating oral candidiasis. Odontology 111: 350-359. https://doi.org/10.1007/s10266-022-00742-4
|
| [52] |
Jennings MR, Parks RJ (2020) Curcumin as an antiviral agent. Viruses 12: 1242. https://doi.org/10.3390/v12111242
|
| [53] |
Šudomová M, Hassan STS (2021) Nutraceutical curcumin with promising protection against herpesvirus infections and their associated inflammation: Mechanisms and pathways. Microorganisms 9: 292. https://doi.org/10.3390/microorganisms9020292
|
| [54] |
Liczbiński P, Michałowicz J, Bukowska B (2020) Molecular mechanism of curcumin action in signaling pathways: Review of the latest research. Phytother Res 34: 1992-2005. https://doi.org/10.1002/ptr.6663
|
| [55] |
Hasanzadeh S, Read MI, Bland AR, et al. (2020) Curcumin: An inflammasome silencer. Pharmacol Res 159: 104921. https://doi.org/10.1016/j.phrs.2020.104921
|
| [56] |
Sinjari B, Pizzicannella J, D'aurora M, et al. (2019) Curcumin/liposome nanotechnology as delivery platform for anti-inflammatory activities via NFkB/ERK/pERK pathway in human dental pulp treated with 2-HydroxyEthyl MethAcrylate (HEMA). Front Physiol 10: 633. https://doi.org/10.3389/fphys.2019.00633
|
| [57] |
Breschi L, Maravic T, Cunha SR, et al. (2018) Dentin bonding systems: From dentin collagen structure to bond preservation and clinical applications. Dent Mater 34: 78-96. https://doi.org/10.1016/j.dental.2017.11.005
|
| [58] |
Liu Y, Tjäderhane L, Breschi L, et al. (2011) Limitations in bonding to dentin and experimental strategies to prevent bond degradation. J Dent Res 90: 953-968. https://doi.org/10.1177/0022034510391799
|
| [59] |
Seseogullari-Dirihan R, Mutluay MM, Vallittu P, et al. (2015) Effect of pretreatment with collagen crosslinkers on dentin protease activity. Dent Mater 31: 941-947. https://doi.org/10.1016/j.dental.2015.05.002
|
| [60] |
Seseogullari-Dirihan R, Apollonio F, Mazzoni A, et al. (2016) Use of crosslinkers to inactivate dentin MMPs. Dent Mater 32: 423-432. https://doi.org/10.1016/j.dental.2015.12.012
|
| [61] |
Seseogullari-Dirihan R, Mutluay MM, Pashley DH, et al. (2017) Is the inactivation of dentin proteases by crosslinkers reversible?. Dent Mater 33: e62-e68. https://doi.org/10.1016/j.dental.2016.09.036
|
| [62] |
Xiao C, Yu X, Xie J, et al. (2018) Protective effect and related mechanisms of curcumin in rat experimental periodontitis. Head Face Med 14: 12. https://doi.org/10.1186/s13005-018-0169-1
|
| [63] |
Guimarães MR, De Aquino SG, Coimbra LS, et al. (2012) Curcumin modulates the immune response associated with LPS-induced periodontal disease in rats. Innate Immun 18: 155-163. https://doi.org/10.1177/1753425910392935
|
| [64] |
Toraya S, Uehara O, Hiraki D, et al. (2020) Curcumin inhibits the expression of proinflammatory mediators and MMP-9 in gingival epithelial cells stimulated for a prolonged period with lipopolysaccharides derived from Porphyromonas gingivalis. Odontology 108: 16-24. https://doi.org/10.1007/s10266-019-00432-8
|
| [65] |
Anitha V, Rajesh P, Shanmugam M, et al. (2015) Comparative evaluation of natural curcumin and synthetic chlorhexidine in the management of chronic periodontitis as a local drug delivery: A clinical and microbiological study. Indian J Dent Res 26: 53-56. https://doi.org/10.4103/0970-9290.156806
|
| [66] |
Zhang L, Tan J, Liu Y, et al. (2024) Curcumin relieves arecoline-induced oral submucous fibrosis via inhibiting the LTBP2/NF-κB axis. Oral Dis 30: 2314-2324. https://doi.org/10.1111/odi.14656
|
| [67] |
Chatterjee A, Debnath K, Rao NKH (2017) A comparative evaluation of the efficacy of curcumin and chlorhexidine mouthrinses on clinical inflammatory parameters of gingivitis: A double-blinded randomized controlled clinical study. J Indian Soc Periodontol 21: 132-137. https://doi.org/10.4103/jisp.jisp_136_17
|
| [68] |
Malekzadeh M, Kia SJ, Mashaei L, et al. (2021) Oral nano-curcumin on gingival inflammation in patients with gingivitis and mild periodontitis. Clin Exp Dent Res 7: 78-84. https://doi.org/10.1002/cre2.330
|
| [69] |
Saran G, Umapathy D, Misra N, et al. (2018) A comparative study to evaluate the efficacy of lycopene and curcumin in oral submucous fibrosis patients: A randomized clinical trial. Indian J Dent Res 29: 303-312. https://doi.org/10.4103/ijdr.IJDR_551_16
|
| [70] |
Ali FM, Aher V, Prasant MC, et al. (2013) Oral submucous fibrosis: Comparing clinical grading with duration and frequency of habit among areca nut and its products chewers. J Cancer Res Ther 9: 471-476. https://doi.org/10.4103/0973-1482.119353
|
| [71] |
Hande AH, Chaudhary MS, Gawande MN, et al. (2019) Oral submucous fibrosis: An enigmatic morpho-insight. J Cancer Res Ther 15: 463-469. https://doi.org/10.4103/jcrt.JCRT_522_17
|
| [72] |
Srivastava A, Agarwal R, Chaturvedi TP, et al. (2015) Clinical evaluation of the role of tulsi and turmeric in the management of oral submucous fibrosis: A pilot, prospective observational study. J Ayurveda Integr Med 6: 45-49.
|
| [73] |
Nerkar Rajbhoj A, Kulkarni TM, Shete A, et al. (2021) A comparative study to evaluate efficacy of curcumin and aloe vera gel along with oral physiotherapy in the management of oral submucous fibrosis: A randomized clinical trial. Asian Pac J Cancer Prev 22: 107-112. https://doi.org/10.31557/apjcp.2021.22.s1.107
|
| [74] |
Ara SA, Mudda JA, Lingappa A, et al. (2016) Research on curcumin: A meta-analysis of potentially malignant disorders. J Cancer Res Ther 12: 175-181. https://doi.org/10.4103/0973-1482.171370
|
| [75] |
Gupta S, Ghosh S, Gupta S, et al. (2017) Effect of curcumin on the expression of p53, transforming growth factor-β, and inducible nitric oxide synthase in oral submucous fibrosis: A pilot study. J Invest Clin Dent 8: e12252. https://doi.org/10.1111/jicd.12252
|
| [76] | Al-Maweri SA (2019) Efficacy of curcumin for management of oral submucous fibrosis: A systematic review of randomized clinical trials. Oral Surg Oral Med O 127: 300-308. https://doi.org/10.1016/j.oooo.2019.01.010 |
| [77] | Chandrashekar A, Annigeri RG, Va U, et al. (2021) A clinicobiochemical evaluation of curcumin as gel and as buccal mucoadhesive patches in the management of oral submucous fibrosis. Oral Surg Oral Med O 131: 428-434. https://doi.org/10.1016/j.oooo.2020.12.020 |
| [78] |
Chen D, Xi Y, Zhang S, et al. (2022) Curcumin attenuates inflammation of Macrophage-derived foam cells treated with Poly-L-lactic acid degradation via PPARγ signaling pathway. J Mater Sci Mater Med 33: 33. https://doi.org/10.1007/s10856-022-06654-7
|
| [79] |
Rai A, Qazi S, Raza K (2022) In silico analysis and comparative molecular docking study of FDA approved drugs with transforming growth factor beta receptors in oral submucous fibrosis. Indian J Otolaryngol Head Neck Surgery 74: 2111-2121. https://doi.org/10.1007/s12070-020-02014-5
|
| [80] |
Klopfleisch R, Jung F (2017) The pathology of the foreign body reaction against biomaterials. J Biomed Mater Res A 105: 927-940. https://doi.org/10.1002/jbm.a.35958
|
| [81] |
Wu J, Deng J, Theocharidis G, et al. (2024) Adhesive anti-fibrotic interfaces on diverse organs. Nature 630: 360-367. https://doi.org/10.1038/s41586-024-07426-9
|
| [82] |
Yang C, Zhu K, Yuan X, et al. (2020) Curcumin has immunomodulatory effects on RANKL-stimulated osteoclastogenesis in vitro and titanium nanoparticle-induced bone loss in vivo. J Cell Mol Med 24: 1553-1567. https://doi.org/10.1111/jcmm.14842
|
| [83] |
Khezri K, Dizaj SM, Saadat YR, et al. (2021) Osteogenic differentiation of mesenchymal stem cells via curcumin-containing nanoscaffolds. Stem Cells Int 2021: 1520052. https://doi.org/10.1155/2021/1520052
|
| [84] |
Chen S, Liang H, Ji Y, et al. (2021) Curcumin modulates the crosstalk between macrophages and bone mesenchymal stem cells to ameliorate osteogenesis. Front Cell Dev Biol 9: 634650. https://doi.org/10.3389/fcell.2021.634650
|
| [85] |
Liu B, Zhou C, Zhang Z, et al. (2021) Antimicrobial property of halogenated catechols. Chem Eng J 403: 126340. https://doi.org/10.1016/j.cej.2020.126340
|
| [86] |
Jiang C, Luo P, Li X, et al. (2020) Nrf2/ARE is a key pathway for curcumin-mediated protection of TMJ chondrocytes from oxidative stress and inflammation. Cell Stress Chaperon 25: 395-406. https://doi.org/10.1007/s12192-020-01079-z
|
| [87] |
Chen D, Yu C, Ying Y, et al. (2022) Study of the osteoimmunomodulatory properties of curcumin-modified copper-bearing titanium. Molecules 27: 3205. https://doi.org/10.3390/molecules27103205
|
| [88] |
Wusiman P, Maimaitituerxun B, Guli, et al. (2020) Epidemiology and pattern of oral and maxillofacial trauma. J Craniofac Surg 31: e517-e520. https://doi.org/10.1097/scs.0000000000006719
|
| [89] |
Lam R (2016) Epidemiology and outcomes of traumatic dental injuries: A review of the literature. Aust Dent J 61: 4-20. https://doi.org/10.1111/adj.12395
|
| [90] | Lynham A, Tuckett J, Warnke P (2012) Maxillofacial trauma. Aust Fam Physician 41: 172-180. |
| [91] |
Falanga V (2005) Wound healing and its impairment in the diabetic foot. Lancet 366: 1736-1743. https://doi.org/10.1016/s0140-6736(05)67700-8
|
| [92] |
Barchitta M, Maugeri A, Favara G, et al. (2019) Nutrition and wound healing: An overview focusing on the beneficial effects of curcumin. Int J Mol Sci 20: 1119. https://doi.org/10.3390/ijms20051119
|
| [93] |
Velnar T, Bailey T, Smrkolj V (2009) The wound healing process: An overview of the cellular and molecular mechanisms. J Int Med Res 37: 1528-1542. https://doi.org/10.1177/147323000903700531
|
| [94] |
Keihanian F, Saeidinia A, Bagheri RK, et al. (2018) Curcumin, hemostasis, thrombosis, and coagulation. J Cell Physiol 233: 4497-4511. https://doi.org/10.1002/jcp.26249
|
| [95] |
Tabeshpour J, Hashemzaei M, Sahebkar A (2018) The regulatory role of curcumin on platelet functions. J Cell Biochem 119: 8713-8722. https://doi.org/10.1002/jcb.27192
|
| [96] |
Hunter CJ, De Plaen IG (2014) Inflammatory signaling in NEC: Role of NF-κB, cytokines and other inflammatory mediators. Pathophysiology 21: 55-65. https://doi.org/10.1016/j.pathophys.2013.11.010
|
| [97] |
Gopinath D, Ahmed MR, Gomathi K, et al. (2004) Dermal wound healing processes with curcumin incorporated collagen films. Biomaterials 25: 1911-1917. https://doi.org/10.1016/s0142-9612(03)00625-2
|
| [98] |
Tapia E, Sánchez-Lozada LG, García-Niño WR, et al. (2014) Curcumin prevents maleate-induced nephrotoxicity: Relation to hemodynamic alterations, oxidative stress, mitochondrial oxygen consumption and activity of respiratory complex I. Free Radical Res 48: 1342-1354. https://doi.org/10.3109/10715762.2014.954109
|
| [99] |
Chaushu L, Gavrielov MR, Chaushu G, et al. (2021) Curcumin promotes primary oral wound healing in a rat model. J Med Food 24: 422-430. https://doi.org/10.1089/jmf.2020.0093
|
| [100] |
Mohanty C, Das M, Sahoo SK (2012) Sustained wound healing activity of curcumin loaded oleic acid based polymeric bandage in a rat model. Mol Pharm 9: 2801-2811. https://doi.org/10.1021/mp300075u
|
| [101] |
Akbik D, Ghadiri M, Chrzanowski W, et al. (2014) Curcumin as a wound healing agent. Life Sci 116: 1-7. https://doi.org/10.1016/j.lfs.2014.08.016
|
| [102] |
Singer AJ, Clark RA (1999) Cutaneous wound healing. N Engl J Med 341: 738-746. https://doi.org/10.1056/nejm199909023411006
|
| [103] |
Habiboallah G, Nasroallah S, Mahdi Z, et al. (2008) Histological evaluation of Curcuma longa-ghee formulation and hyaluronic acid on gingival healing in dog. J Ethnopharmacol 120: 335-341. https://doi.org/10.1016/j.jep.2008.09.011
|
| [104] |
Murgia D, Angellotti G, Conigliaro A, et al. (2020) Development of a multifunctional bioerodible nanocomposite containing metronidazole and curcumin to apply on L-PRF clot to promote tissue regeneration in dentistry. Biomedicines 8: 425. https://doi.org/10.3390/biomedicines8100425
|
| [105] | Mitie A, Todorovic K, Stojiljkovic N, et al. (2017) Beneficial effects of curcumin on the wound-healing process after tooth extraction. Nat Prod Commun 12: 1905-1908. https://doi.org/10.1177/1934578X1701201223 |
| [106] |
Rujirachotiwat A, Suttamanatwong S (2021) Curcumin promotes collagen type I, keratinocyte growth factor-1, and epidermal growth factor receptor expressions in the in vitro wound healing model of human gingival fibroblasts. Eur J Dent 15: 63-70. https://doi.org/10.1055/s-0040-1715781
|
| [107] | Thakur A, Kumar A, Hasan S, et al. (2019) Curcumin in oral mucosal lesions: An update. Asian J Pharm Clin Res 12: 32-43. https://doi.org/10.22159/ajpcr.2019.v12i2.22458 |
| [108] |
Bashang H, Tamma S (2020) The use of curcumin as an effective adjuvant to cancer therapy: A short review. Biotechnol Appl Biochem 67: 171-179. https://doi.org/10.1002/bab.1836
|
| [109] | Wang Y, Lu J, Jiang B, et al. (2020) The roles of curcumin in regulating the tumor immunosuppressive microenvironment. Oncol Lett 19: 3059-3070. https://doi.org/10.3892/ol.2020.11437 |
| [110] |
Radhika T, Jeddy N, Nithya S, et al. (2016) Salivary biomarkers in oral squamous cell carcinoma-An insight. J Oral Biol Craniofac Res 6: S51-S54. https://doi.org/10.1016/j.jobcr.2016.07.003
|
| [111] |
Nagel-Wolfrum K, Buerger C, Wittig I, et al. (2004) The interaction of specific peptide aptamers with the DNA binding domain and the dimerization domain of the transcription factor Stat3 inhibits transactivation and induces apoptosis in tumor cells. Mol Cancer Res 2: 170-182. https://doi.org/10.1158/1541-7786.170.2.3
|
| [112] |
Ma C, Zhuang Z, Su Q, et al. (2020) Curcumin has anti-proliferative and pro-apoptotic effects on tongue cancer in vitro: A study with bioinformatics analysis and in vitro experiments. Drug Des Devel Ther 14: 509-518. https://doi.org/10.2147/dddt.s237830
|
| [113] |
Liao F, Liu L, Luo E, et al. (2018) Curcumin enhances anti-tumor immune response in tongue squamous cell carcinoma. Arch Oral Biol 92: 32-37. https://doi.org/10.1016/j.archoralbio.2018.04.015
|
| [114] | Zhen L, Fan D, Yi X, et al. (2014) Curcumin inhibits oral squamous cell carcinoma proliferation and invasion via EGFR signaling pathways. Int J Clin Exp Pathol 7: 6438-6446. https://doi.org/10.1158/1541-7786.MCR-04-0010 |
| [115] |
Yaguchi T, Sumimoto H, Kudo-Saito C, et al. (2011) The mechanisms of cancer immunoescape and development of overcoming strategies. Int J Hematol 93: 294-300. https://doi.org/10.1007/s12185-011-0799-6
|
| [116] |
Lee H, Jeong AJ, Ye SK (2019) Highlighted STAT3 as a potential drug target for cancer therapy. BMB Rep 52: 415-423. https://doi.org/10.5483/BMBRep.2019.52.7.152
|
| [117] | Ohnishi Y, Sakamoto T, Zhengguang L, et al. (2020) Curcumin inhibits epithelial-mesenchymal transition in oral cancer cells via c-Met blockade. Oncol Lett 19: 4177-4182. https://doi.org/10.3892/ol.2020.11523 |
| [118] |
Hu A, Huang JJ, Li RL, et al. (2015) Curcumin as therapeutics for the treatment of head and neck squamous cell carcinoma by activating SIRT1. Sci Rep 5: 13429. https://doi.org/10.1038/srep13429
|
| [119] |
Srivastava S, Mohammad S, Pant AB, et al. (2018) Co-delivery of 5-fluorouracil and curcumin nanohybrid formulations for improved chemotherapy against oral squamous cell carcinoma. J Maxillofac Oral Surg 17: 597-610. https://doi.org/10.1007/s12663-018-1126-z
|
| [120] |
Molla S, Hembram KC, Chatterjee S, et al. (2020) PARP inhibitor olaparib enhances the apoptotic potentiality of curcumin by increasing the DNA damage in oral cancer cells through inhibition of BER cascade. Pathol Oncol Res 26: 2091-2103. https://doi.org/10.1007/s12253-019-00768-0
|
| [121] |
Gupta N, Verma K, Nalla S, et al. (2020) Free radicals as a double-edged sword: The cancer preventive and therapeutic roles of curcumin. Molecules 25: 5390. https://doi.org/10.3390/molecules25225390
|
| [122] |
Kia SJ, Basirat M, Saedi HS, et al. (2021) Effects of nanomicelle curcumin capsules on prevention and treatment of oral mucositis in patients under chemotherapy with or without head and neck radiotherapy: a randomized clinical trial. BMC Complement Med Ther 21: 232. https://doi.org/10.1186/s12906-021-03400-4
|
| [123] |
Srivastava S, Mohammad S, Gupta S, et al. (2018) Chemoprotective effect of nanocurcumin on 5-fluorouracil-induced-toxicity toward oral cancer treatment. Natl J Maxillofac Surg 9: 160-166. https://doi.org/10.4103/njms.NJMS_27_18
|
| [124] |
Hegde MN, Gatti P, Hegde ND (2019) Protection of wear resistance behaviour of enamel against electron beam irradiation. BDJ Open 5: 11. https://doi.org/10.1038/s41405-019-0021-0
|
| [125] |
Delavarian Z, Pakfetrat A, Ghazi A, et al. (2019) Oral administration of nanomicelle curcumin in the prevention of radiotherapy-induced mucositis in head and neck cancers. Spec Care Dentist 39: 166-172. https://doi.org/10.1111/scd.12358
|
| [126] |
Antonazzo IC, Gribaudo G, La Vecchia A, et al. (2024) Cost and cost effectiveness of treatments for psoriatic arthritis: An updated systematic literature review. Pharmacoeconomics 42: 1329-1343. https://doi.org/10.1007/s40273-024-01428-1
|
| [127] |
Ulmansky M, Michelle R, Azaz B (1995) Oral psoriasis: Report of six new cases. J Oral Pathol Med 24: 42-45. https://doi.org/10.1111/j.1600-0714.1995.tb01128.x
|
| [128] |
Zargari O (2006) The prevalence and significance of fissured tongue and geographical tongue in psoriatic patients. Clin Exp Dermatol 31: 192-195. https://doi.org/10.1111/j.1365-2230.2005.02028.x
|
| [129] |
Ogueta CI, Ramírez PM, Jiménez OC, et al. (2019) Geographic tongue: What a dermatologist should know. Actas Dermo-Sifiliográficas 110: 341-346. https://doi.org/10.1016/j.ad.2018.10.022
|
| [130] |
Lowes MA, Suárez-Fariñas M, Krueger JG (2014) Immunology of psoriasis. Annu Rev Immunol 32: 227-255. https://doi.org/10.1146/annurev-immunol-032713-120225
|
| [131] |
Rendon A, Schäkel K (2019) Psoriasis pathogenesis and treatment. Int J Mol Sci 20: 1475. https://doi.org/10.3390/ijms20061475
|
| [132] |
Panahi Y, Fazlolahzadeh O, Atkin SL, et al. (2019) Evidence of curcumin and curcumin analogue effects in skin diseases: A narrative review. J Cell Physiol 234: 1165-1178. https://doi.org/10.1002/jcp.27096
|
| [133] |
Kang D, Li B, Luo L, et al. (2016) Curcumin shows excellent therapeutic effect on psoriasis in mouse model. Biochimie 123: 73-80. https://doi.org/10.1016/j.biochi.2016.01.013
|
| [134] |
Tziotzios C, Lee JYW, Brier T, et al. (2018) Lichen planus and lichenoid dermatoses: Clinical overview and molecular basis. J Am Acad Dermatol 79: 789-804. https://doi.org/10.1016/j.jaad.2018.02.010
|
| [135] |
Eisen D, Carrozzo M, Sebastian JVB, et al. (2005) Number V Oral lichen planus: Clinical features and management. Oral Dis 11: 338-349. https://doi.org/10.1111/j.1601-0825.2005.01142.x
|
| [136] |
Roopashree MR, Gondhalekar RV, Shashikanth MC, et al. (2010) Pathogenesis of oral lichen planus—A review. J Oral Pathol Med 39: 729-734. https://doi.org/10.1111/j.1600-0714.2010.00946.x
|
| [137] |
Bombeccari GP, Giannì AB, Spadari F (2017) Oral Candida colonization and oral lichen planus. Oral Dis 23: 1009-1010. https://doi.org/10.1111/odi.12681
|
| [138] |
Salehi B, Lopez-Jornet P, López EPF, et al. (2019) Plant-derived bioactives in oral mucosal lesions: A key emphasis to curcumin, lycopene, chamomile, aloe vera, green tea and coffee properties. Biomolecules 9: 106. https://doi.org/10.3390/biom9030106
|
| [139] |
Kia SJ, Basirat M, Mortezaie T, et al. (2020) Comparison of oral nano-curcumin with oral prednisolone on oral lichen planus: A randomized double-blinded clinical trial. BMC Complement Med Ther 20: 328. https://doi.org/10.1186/s12906-020-03128-7
|
| [140] |
White CM, Chamberlin K, Eisenberg E (2019) Curcumin, a turmeric extract, for oral lichen planus: A systematic review. Oral Dis 25: 720-725. https://doi.org/10.1111/odi.13034
|
| [141] |
Lv KJ, Chen TC, Wang GH, et al. (2019) Clinical safety and efficacy of curcumin use for oral lichen planus: A systematic review. J Dermatol Treat 30: 605-611. https://doi.org/10.1080/09546634.2018.1543849
|
| [142] |
Li H, Yue L, Xu H, et al. (2019) Curcumin suppresses osteogenesis by inducing miR-126a-3p and subsequently suppressing the WNT/LRP6 pathway. Aging 11: 6983-6998. https://doi.org/10.18632/aging.102232
|
| [143] |
Yang Q, Leong SA, Chan KP, et al. (2021) Complex effect of continuous curcumin exposure on human bone marrow-derived mesenchymal stem cell regenerative properties through matrix metalloproteinase regulation. Basic Clin Pharmacol Toxicol 128: 141-153. https://doi.org/10.1111/bcpt.13477
|
| [144] |
Yang M, Liu J, Liu C, et al. (2025) Programmable food-derived peptide coassembly strategies for boosting targeted colitis therapy by enhancing oral bioavailability and restoring gut microenvironment homeostasis. ACS Nano 19: 600-620. https://doi.org/10.1021/acsnano.4c11108
|
| [145] |
Nguyen MH, Yu H, Kiew TY, et al. (2015) Cost-effective alternative to nano-encapsulation: Amorphous curcumin–chitosan nanoparticle complex exhibiting high payload and supersaturation generation. Eur J Pharm Biopharm 96: 1-10. https://doi.org/10.1016/j.ejpb.2015.07.007
|
| [146] |
Pei Z, Chen S, Ding L, et al. (2022) Current perspectives and trend of nanomedicine in cancer: A review and bibliometric analysis. J Control Release 352: 211-241. https://doi.org/10.1016/j.jconrel.2022.10.023
|
| [147] |
Fernandez-Fernandez A, Manchanda R, Rodrigues JMC, et al. (2023) State-of-the-art rational nanodesign: From screening to theranostics and from bench to clinic. Front Pharmacol 14: 1210185. https://doi.org/10.3389/fphar.2023.1210185
|
| [148] |
Szymusiak M, Hu X, Plata PAL, et al. (2016) Bioavailability of curcumin and curcumin glucuronide in the central nervous system of mice after oral delivery of nano-curcumin. Int J Pharm 511: 415-423. https://doi.org/10.1016/j.ijpharm.2016.07.027
|
| [149] |
Bakhshi M, Mahboubi A, Jaafari M R, et al. (2022) Comparative efficacy of 1% curcumin nanomicelle gel and 2% curcumin gel for treatment of recurrent aphthous stomatitis: a double-blind randomized clinical trial. J Evid Based Dent Pract 22: 101708. https://doi.org/10.1016/j.jebdp.2022.101708
|
| [150] |
Hafez Ghoran S, Calcaterra A, Abbasi M, et al. (2022) Curcumin-based nanoformulations: A promising adjuvant towards cancer treatment. Molecules 27: 5236. https://doi.org/10.3390/molecules27165236
|
| [151] |
Yallapu MM, Jaggi M, Chauhan SC (2012) Curcumin nanoformulations: A future nanomedicine for cancer. Drug Discov Today 17: 71-80. https://doi.org/10.1016/j.drudis.2011.09.009
|
| [152] |
Zheng Y, Jia R, Li J, et al. (2025) Expression of concern: Curcumin-and resveratrol-co-loaded nanoparticles in synergistic treatment of hepatocellular carcinoma. J Nanobiotechnol 23: 288. https://doi.org/10.1186/s12951-025-03361-7
|
| [153] |
Wang J, Zhang T, Gu R, et al. (2024) Development and evaluation of reconstructed nanovesicles from turmeric for multifaceted obesity intervention. ACS Nano 18: 23117-23135. https://doi.org/10.1021/acsnano.4c05309
|
| [154] |
Sahyon HBS, da Silva PP, de Oliveira MS, et al. (2019) Influence of curcumin photosensitizer in photodynamic therapy on the mechanical properties and push-out bond strength of glass-fiber posts to intraradicular dentin. Photodiagn Photodyn 25: 376-381. https://doi.org/10.1016/j.pdpdt.2019.01.025
|
| [155] |
Al Ahdal K, Al Deeb L, Al-Hamdan RS, et al. (2020) Influence of different photosensitizers on push-out bond strength of fiber post to radicular dentin. Photodiagn Photodyn 31: 101805. https://doi.org/10.1016/j.pdpdt.2020.101805
|
| [156] |
Strazzi-Sahyon HB, Da Silva PP, Nakao JM, et al. (2021) Influence of two photodynamic therapy sessions and different photosensitizers on the bond strength of glass-fiber posts in different regions of intraradicular dentin. Photodiagn Photodyn 33: 102193. https://doi.org/10.1016/j.pdpdt.2021.102193
|



Figures(4)

Juan Zhang, Yuhan Peng, Siting Hu, Jianmeng Xu, Chengcheng Yu, Lei Hua, Shihui Zhou, Qi Liu. Therapeutic application of curcumin and its nanoformulation in dentistry: Opportunities and challenges[J]. AIMS Molecular Science, 2025, 12(2): 148-172. doi: 10.3934/molsci.2025010







 DownLoad:
DownLoad: