Citation: Shuoer Wang, Yidi Sun, Songjiao Zhao, Feng Wei, Gong Yang. Breast conserving surgery (BCS) with adjuvant radiation therapy showed improved prognosis compared with mastectomy for early staged triple negative breast cancer patients[J]. Mathematical Biosciences and Engineering, 2020, 17(1): 92-104. doi: 10.3934/mbe.2020005

| [1] | R. L. Siegel, K. D. Miller and A. Jemal, Cancer statistics, 2017, Ca-Cancer J. Clin., 67 (2017), 7-30. |
| [2] | R. Ismail-Khan and M. M. Bui, A review of triple-negative breast cancer, Cancer Control: J. Moffitt Cancer Center, 17 (2010), 173-176. |
| [3] | P. Boyle, Triple-negative breast cancer: Epidemiological considerations and recommendations, Ann. Oncol.: Off. J. Eur. Soc. Med. Oncol., 23 (2012), 7-12. |
| [4] | N. U. Lin, A. Vanderplas, M. E. Hughes, et al, Clinicopathologic features, patterns of recurrence, and survival among women with triple-negative breast cancer in the National Comprehensive Cancer Network, Cancer, 118 (2012), 5463-5472. |
| [5] | X. Chen, F. Xia, J. Luo, et al, Postmastectomy radiotherapy reduces locoregional and disease recurrence in patients with stage Ⅱ-Ⅲ triple-negative breast cancer treated with neoadjuvant chemotherapy and mastectomy, OncoTargets Ther., 11 (2018), 1973-1980. |
| [6] | R. W. Carlson, D. C. Allred, B. O. Anderson, et al, Breast cancer. Clinical practice guidelines in oncology, J. Nat. Compr. Cancer Network: JNCCN, 7 (2009), 122-192. |
| [7] | W. Gradishar, K. E. Salerno, NCCN guidelines update: Breast cancer, J. Natl. Compr. Cancer Network, 14 (2016), 641-644. |
| [8] | U. Veronesi, N. Cascinelli, L. Mariani, et al., Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer, New Eng. J. Med., 347 (2002), 1227-1232. |
| [9] | B. S. Abdulkarim, J. Cuartero, J. Hanson, et al., Increased risk of locoregional recurrence for women with T1-2N0 triple-negative breast cancer treated with modified radical mastectomy without adjuvant radiation therapy compared with breast-conserving therapy, J. Clin. Oncol.: Off. J. Am. Soc. Clin. Oncol., 29 (2011), 2852-2858. |
| [10] | F. C. Adkins, A. M. Gonzalez-Angulo, X. Lei, et al, Triple-negative breast cancer is not a contraindication for breast conservation, Ann. Surg. Oncol., 18 (2011), 3164-3173. |
| [11] | M. C. van Maaren, L. de Munck, G. H. de Bock, et al., 10 year survival after breast-conserving surgery plus radiotherapy compared with mastectomy in early breast cancer in the Netherlands: A population-based study, Lancet Oncol., 17 (2016), 1158-1170. |
| [12] | X. Chen, X. Yu, J. Chen, et al., Analysis in early stage triple-negative breast cancer treated with mastectomy without adjuvant radiotherapy: Patterns of failure and prognostic factors, Cancer, 119 (2013), 2366-2374. |
| [13] |
Q. X. Chen, X. X. Wang, P. Y. Lin, et al., The different outcomes between breast-conserving surgery and mastectomy in triple-negative breast cancer: A population-based study from the SEER 18 database, Oncotarget, 8 (2017), 4773-4780. doi: 10.18632/oncotarget.13976

|
| [14] | J. K. Horton, R. Jagsi, W. A. Woodward, et al., Breast cancer biology: Clinical implications for breast radiation therapy, Int. J. Radiat. Oncol., Biol., Phys., 100 (2018), 23-37. |
| [15] | R. C. Brianese, K. D. M. Nakamura, F. Almeida, et al, BRCA1 deficiency is a recurrent event in early-onset triple-negative breast cancer: A comprehensive analysis of germline mutations and somatic promoter methylation, Breast Cancer Res. Treatment., 167 (2018), 803-814. |
| [16] | S. Y. Phuah, L. M. Looi, N. Hassan, et al., Triple-negative breast cancer and PTEN (phosphatase and tensin homologue) loss are predictors of BRCA1 germline mutations in women with early-onset and familial breast cancer, but not in women with isolated late-onset breast cancer, Breast Cancer Res., 14 (2012), R142. |
| [17] |
M. Kalimutho, K. Parsons, D. Mittal, et al., Targeted therapies for triple-negative breast cancer: Combating a stubborn disease, Trends Pharmacol. Sci., 36 (2015), 822-846. doi: 10.1016/j.tips.2015.08.009
|
| [18] | H. Jia, C. I. Truica, B. Wang, et al., Immunotherapy for triple-negative breast cancer: Existing challenges and exciting prospects, Drug Resist. Updates: Rev. Comment. Antimicrob. Anticancer Chemother., 32 (2017), 1-15. |
Figures(1) / Tables(4)

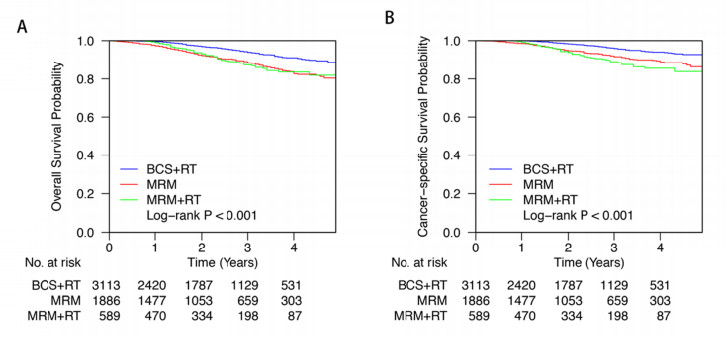
Shuoer Wang, Yidi Sun, Songjiao Zhao, Feng Wei, Gong Yang. Breast conserving surgery (BCS) with adjuvant radiation therapy showed improved prognosis compared with mastectomy for early staged triple negative breast cancer patients







 DownLoad:
DownLoad: