Citation: Nosheen Aslam, Muhammad Sarfaraz Iqbal, Syed Makhdoom Hussain, Muhammad Rizwan, Qurat-Ul-Ain Naseer, Muhammad Afzal, Rizwan Muneer, Farzana Batool. Effects of chelating agents on heavy metals in Hepatitis C Virus (HCV) patients[J]. Mathematical Biosciences and Engineering, 2019, 16(3): 1138-1149. doi: 10.3934/mbe.2019054

| [1] | M. S. Iqbal, U. A. Ashfaq and S. Khaliq, et al., Toll-like receptor 4 polymorphism as pretreatment predictor of response to HCV genotype 3a interferon-based treatment, Future. Med., 12 (2017). |
| [2] | A. Arshad and U. A. Ashfaq, Epidemiology of hepatitis c infection in pakistan: Current estimate and major risk factors, 27 (2017), 63–77. |
| [3] | M. S. Iqbal, U. A. Ashfaq and S. Aslam, et al., Analysis of polymorphism rs1990760 of IFIH1 gene and treatment outcomes in HCV infection, Future. Virol., 13 (2018). |
| [4] | N. Jiwani, N. J. Mscn and R. Gul, A silent storm : Hepatitis C in Pakistan, 1 (2011), 89–91. |
| [5] | M. U. Ghani, A. Haque and M. Qasim, et al., Involvement of vascular endothelial growth factor (VEGF) gene polymorphism in hepatocellular carcinoma of HCV patients from local population, Pure. Appl. Biol., 6 (2017), 725–732. |
| [6] | R. Aslam, S. M. Raza and H. Naeemi, et al., SOCS3 mRNA expression and polymorphisms as pretreatment predictor of response to HCV genotype 3a IFN-based treatment, SpringerPlus, 5 (2016), 1826. |
| [7] | K. Tarao, S. Ohkawa and Y. Miyagi, et al., Inflammation in background cirrhosis evokes malignant progression in HCC development from HCV-associated liver cirrhosis, Scand. J Gastroentero., 48 (2013), 729–735. |
| [8] | N. Aslam, F. Batool and M. S. Iqbal, et al., Analysis of Toll-like receptors-9 (TLR9) gene polymorphism (rs5743836) in Pakistani patients with HCV, Pak. J. Pharm. Sci., 31 (2018), 2709–2714. |
| [9] | L. Piekuse, M. Kreile and A. Zarina, et al., Association between inherited monogenic liver disorders and chronic hepatitis C, World. J. Hepatol., 6 (2014), 92–97. |
| [10] | T. G. Kazi and N. F. Kolachi, Effects of mineral supplementation on liver cirrhotic/cancer male patients, Biol. Trace. Elem. Res., 150 (2012), 81–90. |
| [11] | M. Afify, M. Diaa and E. A. Elmaksoud, et al., Serum levels of trace elements in Egyptian patients with chronic hepatitis C under interferon therapy. J. Genet. Eng. Biotechnol., 10 (2012), 81–86. |
| [12] | J. E. Gall, R. S. Boyd and N. Rajakaruna, Transfer of heavy metals through terrestrial food webs : A review, Environ. Monit. Assess., 187 (2015), 201. |
| [13] | V. M. Varnai, M. Piasek and K. Kostial, Chelators as antidotes of metal toxicity : Therapeutic and experimental aspects, Curr. Med. Chem., 12 (2005), 2771–2794. |
| [14] | H. V. Aposhian, R. M. Maiorino and R. C. Dart, et al., Urinary excretion of 1989, 520–526. |
| [15] | M. P. Simula and V. De Re, Hepatitis c virus-induced oxidative stress and mitochondrial dysfunction: A focus on recent advances in proteomics, Clin. Appl., 4 (2010), 782–793. |
| [16] | M. Vidali, M. F. Tripodi and A. Ivaldi, et al., Interplay between oxidative stress and hepatic steatosis in the progression of chronic hepatitis C, J. Hepatol., 48 (2008), 399–406. |
| [17] | S. J. Polyak, C. Morishima and M. C. Shuhart, et al., Inhibition of T-Cell Inflammatory Cytokines, Hepatocyte NF-κB Signaling, and HCV Infection by Standardized Silymarin, Gastroenterology, 132 (2007), 1925–1936. |
| [18] | K. H. Ibs and L. Rink, Zinc-Altered Immune function, J. Nutr., 133 (2003), 1452S–1456S. |
| [19] | T. Liu, W. He and C. Yan, et al., Roles of reactive oxygen species and mitochondria in cadmium-induced injury of liver cells, Toxicol. Ind. Health, 27 (2010), 249–256. |
| [20] | S. Turgut, A. Polat and M. Inan, et al., Interaction between anemia and blood levels of iron, zinc, copper, cadmium and lead in children, Ind. J. Pediatr., 74 (2007), 827–830. |
| [21] | B. Halliwell and J. M. C. Gutteridge, Role of free radicals and catalytic metal ions in human disease: An overview, Method. Enzymol., 186 (1990), 1–85. |
| [22] | C. Pramoolsinsap, N. Promvanit and S. Komindr, et al., Gastroenterology serum trace metals in chronic viral hepatitis and hepatocellular carcinoma in Thailand, J. Gastroenterol., 29 (1994), 610–615. |
| [23] | A. Ipek, E. Barut and H. Gulen, et al., Assessment of inter- and intra-cultivar variations in olive using SSR markers, Sci. Agri., 69 (2012), 327–335. |
| [24] | B. M. Science and K. Medical, Selenium, iron, copper, and zinc levels and copper-to-zinc ratios in serum of patients at different stages of viral hepatic diseases, Biol. Trace. Elem. Res., 109 (2006), 15–23. |
| [25] | B. Lo, Phytic acid-trace element (Zn, Cu, Mn) interactions, Int. J. Food Sci. Technol., 37 (2002), 749–758. |
| [26] | C. M. Lange, Z. Kutalik and K. Morikawa, et al., Serum ferritin levels are associated with a distinct phenotype of chronic hepatitis C poorly responding to pegylated interferon-alpha and ribavirin therapy, Hepatology, 55 (2012), 1038–1047. |
| [27] | N. Ganne-Carrié, C. Christidis and C. Chastang, et al., Liver iron is predictive of death in alcoholic cirrhosis: A multivariate study of 229 consecutive patients with alcoholic and/or hepatitis c virus cirrhosis: A prospective follow up study, Gut, 46 (2000), 277–282. |
| [28] | H. Ataee-Esfahani, L. Wang and Y. Nemoto, et al., Synthesis of bimetallic Au@Pt nanoparticles with Au core and nanostructured Pt shell toward highly active electrocatalysts, Chem. Mater., 22 (2010), 6310–6318. |
| [29] | D. Ozcelik, R. Ozaras and Z. Gurel, et al., Copper-mediated oxidative stress in rat liver, Biol. Trace. Elem. Res., 96 (2003), 209–215. |
| [30] | O. Tschritter, A. Fritsche and C. Thamer, et al., Plasma adiponectin concentrations predict insulin sensitivity of both glucose and lipid metabolism, Diabetes, 52 (2003), 239–243. |
| [31] | H. Kinoshita, Y. Hori and T. Fukumoto, et al., Novel assessment of hepatic iron distribution by synchrotron radiation X-ray fluorescence microscopy, Med. Mol. Morphol., 43 (2010), 19–25. |
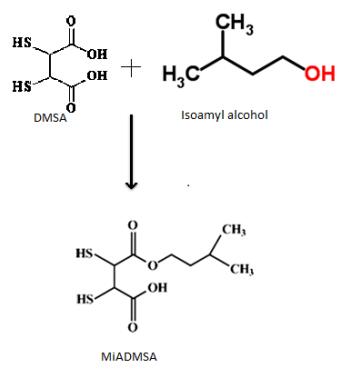
| [32] | V. Pachauri and S. Flora, Combined efficacy of gallic acid and MiADMSA with limited beneficial effects over MiADMSA against arsenic-induced oxidative stress in mouse, Biochem. Insights, 8 (2015), 1–10. |
| [33] | C. Loguercio, V. De Girolamo and A. Federico, et al., Relationship of blood trace elements to liver damage, nutritional status, and oxidative stress in chronic nonalcoholic liver disease, Biol. Trace. Elem. Res., 81 (2001), 245–254. |
| [34] | C. Guo, P. Chen and K. Lin, et al., Trace metal imbalance associated with oxidative stress and inflammatory status in anti-hepatitis c virus antibody, Environ. Toxicol. Phar., 33 (2011), 288–296. |
| [35] | A. U. Neumann, N. P. Lam and H. Dahari, et al., Hepatitis c viral dynamics in vivo and the antiviral efficacy of interferon-α therapy, Science, 282 (1998), 103–107. |
| [36] | R. Y. Dodd and S. L. Stramer, Transfusion complications, 42 (2002), 975–979. |
| [37] | R. Thimme, D, Oldach and K. M. Chang, et al., Determinants of viral clearance and Persistence during Acute hepatitis c virus Infection, J. Exp. Med., 194 (2001), 1395–1406. |
| [38] | O. Lesens, M. Desche and M. Steben, Hepatitis c virus is related to progressive liver disease in human immunodeficiency virus-positive hemophiliacs and should be treated as an opportunistic infection, J. Infect. Dis., 179 (1999), 1254–1258. |
| [39] | G. D. Kelen, G. B. Green and R. H. Purcell, et al., Hepatitis B and Hepatitis C in emergency department patients, New Engl. J. Med., 326 (1992), 1399–1404. |
| [40] | M. El Sayed Zaki and W. Othman, Role of hepatitis E infection in acute on chronic liver failure in Egyptian patients, Liver Int., 31 (2011), 1001–1005. |
| [41] | K. Grüngreiff, T. Hebell and K. Gutensohn, et al., Plasma concentrations of zinc, copper, interleukin-6 and interferon-γ, and plasma dipeptidyl peptidase IV activity in chronic hepatitis C, Mol. Med. Rep., 2 (2009), 63–68. |
| [42] | K. C. Sorensen, S. Venn-Watson and S. H. Ridgway, Trace and non-trace elements in blood cells of bottlenose dolphins (Tursiops truncatus): Variations with values from liver function indicators, J. Wildlife Dis., 44 (2008), 304–317. |
| [43] | M. Takahashi, H. Saito and M. Higashimoto, et al., Possible inhibitory effect of oral zinc supplementation on hepatic fibrosis through downregulation of TIMP-1: A pilot study, Hepatol. Res., 37 (2007), 405–409. |
| [44] | T. Himoto, N. Hosomi and S. Nakai, et al., Efficacy of zinc administration in patients with hepatitis c virus-related chronic liver disease, Scand. J. Gastroentero., 42 (2007), 1078–1087. |
| [45] | M. Blanuša, L. Prester and M. Piasek, et al., Monoisoamyl ester of DMSA reduces 203Hg(NO3)2 retention in rats: 1. Chelation therapy during pregnancy, J. Trace. Elem. Exp. Med., 10 (1997), 173–181. |
| [46] | A. Mehta, S. C. Pant and S. J. S. Flora, Monoisoamyl dimercaptosuccinic acid-induced changes in pregnant female rats during late gestation and lactation, Reprod. Toxicol., 21 (2006), 94–103. |
Figures(2) / Tables(3)

Nosheen Aslam, Muhammad Sarfaraz Iqbal, Syed Makhdoom Hussain, Muhammad Rizwan, Qurat-Ul-Ain Naseer, Muhammad Afzal, Rizwan Muneer, Farzana Batool. Effects of chelating agents on heavy metals in Hepatitis C Virus (HCV) patients[J]. Mathematical Biosciences and Engineering, 2019, 16(3): 1138-1149. doi: 10.3934/mbe.2019054







 DownLoad:
DownLoad: