Citation: J. Appelbaum. A static multiple detector solar radiation sensor[J]. AIMS Energy, 2020, 8(5): 802-818. doi: 10.3934/energy.2020.5.802

| [1] |
Faiman D, Feuermann D, Ibbetson P, et al. (1992) A multipyranometer instrument for obtaining the solar beam and diffuse components, and the irradiance on inclined planes. Sol Energy 48: 253-259. doi: 10.1016/0038-092X(92)90099-V

|
| [2] |
Curtis P (1993) An analysis of methods for deriving the constituent insolation components from multipyranometer array measurements. J Sol Energy Eng 115: 11-21. doi: 10.1115/1.2930018
|
| [3] |
Hamalainen M, Nurkkanen P, Slaen T (1985) A multisensory pyranometer for determination of the direct component and angular distribution of solar radiation. Sol Energy 35: 511-525. doi: 10.1016/0038-092X(85)90120-3
|
| [4] |
Appelbaum J, Bergshtein O (1987) Solar radiation distribution Sensor. Sol Energy 39: 1-10. doi: 10.1016/S0038-092X(87)80046-4
|
| [5] |
Imamura M, Helm P (1992) A novel method of monitoring global normal irradiance with a stationary sensor. Int J Sol Energy 11: 211-217. doi: 10.1080/01425919208909741
|
| [6] | Heisterkamp N, Orthjohann E, Voss J (1994) A multi-purpose irradiance measuring system. 12th European photovoltaic solar Energy conference, Amsterdam, The Netherlans. |
| [7] |
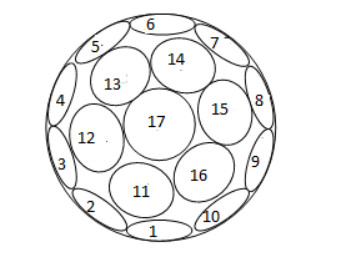
Appelbaum J, Weiss Y (1999) The packing of circles on a hemisphere. Meas Sci Technol 10: 1015-1019. doi: 10.1088/0957-0233/10/11/307
|
| [8] |
Bany J, Appelbaum J (1987) The effect of shading on the design of a field of solar collectors. Sol Cells 20: 201-228. doi: 10.1016/0379-6787(87)90029-9
|
| [9] |
Temp RC, Coulson KL (1977) Solar radiation incident upon slopes of different orientations. Sol Energy 19: 179-184. doi: 10.1016/0038-092X(77)90056-1
|
| [10] | Klucher TM (1979) Evaluation of models to predict insolation on tilted surfaces. Sol Energy 23: 111-114. |
| [11] |
Perez R, Ineichen P, Seal P, et al. (1990) Modeling daylight availability and irradiance componens from direct and global irradiance. Sol Energy 44: 271-289. doi: 10.1016/0038-092X(90)90055-H
|



Figures(16) / Tables(1)

J. Appelbaum. A static multiple detector solar radiation sensor[J]. AIMS Energy, 2020, 8(5): 802-818. doi: 10.3934/energy.2020.5.802







 DownLoad:
DownLoad: