Facial expression of humans is one of the main channels of everyday communication. The reported research work investigated communication regarding the pattern of emotional expression of healthy older adults and with mild cognitive impairments (MCI) or Alzheimer's disease (AD). It focuses on mimicking of displayed emotional facial expression on a sample of 25 older adults (healthy, MCI and AD patients). The adequacy of the patients' individual facial expressions in six basic emotions was measured with the Kinect 3D recording of the participants' facial expressions and compared to their own typical emotional facial expressions. The reactions were triggered by mimicking 49 still pictures of emotional facial expressions. No statistically significant differences in terms of frequency nor adequacy of emotional facial expression were reported in healthy and MCI groups. Unique patterns of emotional expressions have been observed in the AD group. Further investigating the pattern of older adults' facial expression may decrease the misunderstandings and increase the quality of life of the patients.
Citation: Justyna Gerłowska, Krzysztof Dmitruk, Konrad Rejdak. Facial emotion mimicry in older adults with and without cognitive impairments due to Alzheimer's disease[J]. AIMS Neuroscience, 2021, 8(2): 226-238. doi: 10.3934/Neuroscience.2021012
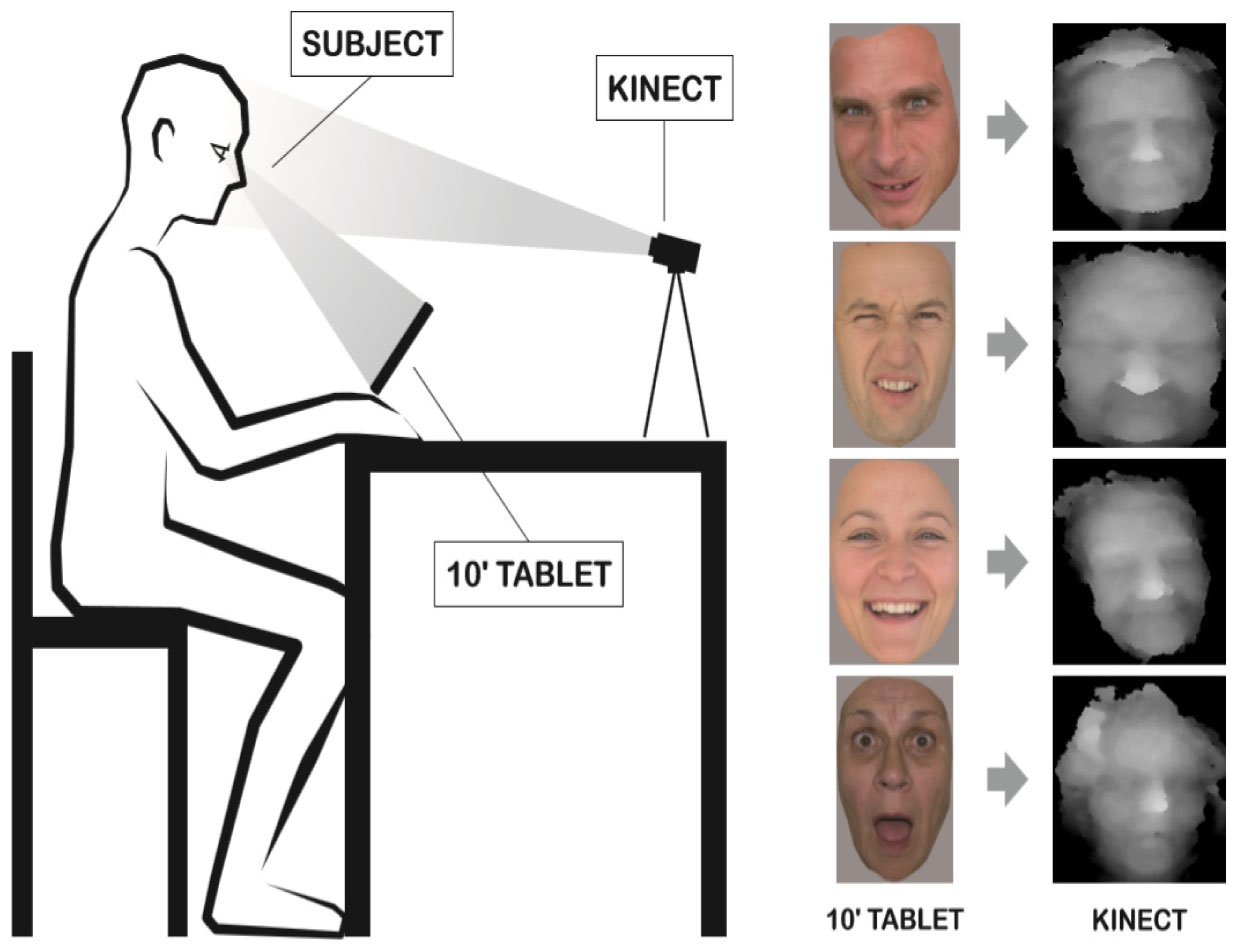
Facial expression of humans is one of the main channels of everyday communication. The reported research work investigated communication regarding the pattern of emotional expression of healthy older adults and with mild cognitive impairments (MCI) or Alzheimer's disease (AD). It focuses on mimicking of displayed emotional facial expression on a sample of 25 older adults (healthy, MCI and AD patients). The adequacy of the patients' individual facial expressions in six basic emotions was measured with the Kinect 3D recording of the participants' facial expressions and compared to their own typical emotional facial expressions. The reactions were triggered by mimicking 49 still pictures of emotional facial expressions. No statistically significant differences in terms of frequency nor adequacy of emotional facial expression were reported in healthy and MCI groups. Unique patterns of emotional expressions have been observed in the AD group. Further investigating the pattern of older adults' facial expression may decrease the misunderstandings and increase the quality of life of the patients.

| [1] |
Gola KA, Shany-Ur T, Pressman P, et al. (2017) A neural network underlying intentional emotional facial expression in neurodegenerative disease. Neuroimage Clin 14: 672-678. doi: 10.1016/j.nicl.2017.01.016

|
| [2] |
Marshall CR, Hardy CJD, Russell LL, et al. (2018) Motor signatures of emotional reactivity in frontotemporal dementia. Sci Rep 8: 1030. doi: 10.1038/s41598-018-19528-2
|
| [3] |
Carr AR, Mendez MF (2018) Affective Empathy in Behavioral Variant Frontotemporal Dementia: A Meta-Analysis. Front Neurol 9: 417. doi: 10.3389/fneur.2018.00417
|
| [4] |
Patel S, Oishi K, Wright A, et al. (2018) Right Hemisphere Regions Critical for Expression of Emotion Through Prosody. Front Neurol 9: 224. doi: 10.3389/fneur.2018.00224
|
| [5] |
Sapey-Triomphe L-A, Heckermann RA, Boublay N, et al. (2015) Neuroanatomical correlates of recognizing face expressions in mild stages of Alzheimer's disease. PLoS One 10: e0143586. doi: 10.1371/journal.pone.0143586
|
| [6] |
Sturm VE, Yokoyama JS, Seeley WW, et al. (2013) Heightened emotional contagion in mild cognitive impairment and Alzheimer's disease is associated with temporal lobe degeneration. Proc Natl Acad Sci USA 110: 9944-9949. doi: 10.1073/pnas.1301119110
|
| [7] |
Virtanen M, Singh-Manoux A, Batty DG, et al. (2017) The level of cognitive function and recognition of emotions in older adults. PLoS One 12: e0185513. doi: 10.1371/journal.pone.0185513
|
| [8] |
Savaskan E, Summermatter D, Schroeder C, et al. (2018) Memory deficits for facial identity in patients with amnestic mild cognitive impairment (MCI). PLoS One 13: e0195693. doi: 10.1371/journal.pone.0195693
|
| [9] |
Rajan KB, Weuve J, Barnes LL, et al. (2019) The diagnosis of dementia due to Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 15: 1-7. doi: 10.1016/j.jalz.2018.07.216
|
| [10] |
Raggi A, Tasca D, Panerai S, et al. (2015) The burden of distress and related coping processes in family caregivers of patients with Alzheimer's disease living in the community. J Neurol Sci 358: 77-81. doi: 10.1016/j.jns.2015.08.024
|
| [11] |
Raivio MM, Laakkonen M-L, Pitkälä KH (2015) Psychological well-being of spousal caregivers of persons with Alzheimer's disease and associated factors. Eur Geriatr Med 6: 128-133. doi: 10.1016/j.eurger.2014.08.006
|
| [12] |
Ikeda C, Terada S, Oshima E, et al. (2015) Difference in determinants of caregiver burden between amnestic mild cognitive impairment and mild Alzheimer's disease. Psychiatry Res 226: 242-246. doi: 10.1016/j.psychres.2014.12.055
|
| [13] |
Hackett RA, Steptoe A, Cadar D, et al. (2019) Social engagement before and after dementia diagnosis in the English Longitudinal Study of Ageing. PLoS One 14: e0220195. doi: 10.1371/journal.pone.0220195
|
| [14] | Dmitruk K, Wójcik GM (2010) Modelling 3D scene based on rapid face tracking and object recognition. Ann UMCS Inform X: 63-68. |
| [15] |
Gonçalves AR, Fernandes C, Pasion R, et al. (2018) Emotion identification and aging: behavioral and neural age-related changes. Clin Neurphysiol 129: 1020-1029. doi: 10.1016/j.clinph.2018.02.128
|
| [16] |
Schmitt H, Kray J, Ferdinand NK (2017) Does the Effort of Processing Potential Incentives Influence the Adaption of Context Updating in Older Adults? Front Psychol 8: 1969. doi: 10.3389/fpsyg.2017.01969
|
| [17] |
Arani A, Murphy MC, Glaser KJ, et al. (2015) Measuring the effects of aging and sex on regional brain stiffness with MR elastography in healthy older adults. Neuroimage 111: 59-64. doi: 10.1016/j.neuroimage.2015.02.016
|
| [18] |
Medaglia JD, Pasqualetti F, Hamilton RH, et al. (2017) Brain and cognitive reserve: Translation via network control theory. Neurosci Biobehav Rev 75: 53-64. doi: 10.1016/j.neubiorev.2017.01.016
|
| [19] |
Albohn DN, Adams jr RB (2020) Everyday beliefs about emotion perceptually derived from neural facial appearance. Front Psychol 11: 264. doi: 10.3389/fpsyg.2020.00264
|
| [20] |
Jarick M, Kingstone A (2015) The duality of gaze: eyes extract and signal social information during sustained cooperative and competitive dyadic gaze. Front Psychol 6: 1423. doi: 10.3389/fpsyg.2015.01423
|
| [21] |
Dampney R (2018) Emotion and the Cardiovascular System: Postulated Role of Inputs From the Medial Prefrontal Cortex to the Dorsolateral Periaqueductal Gray. Front Neurosci 12: 343. doi: 10.3389/fnins.2018.00343
|
| [22] |
Lin H, Müller-Bardorff M, Gathmann B, et al. (2020) Stimulus arousal drives amygdalar responses to emotional expressions across sensory modalities. Sci Rep 10: 1898. doi: 10.1038/s41598-020-58839-1
|
| [23] |
Song J, Wei Y, Ke H (2019) The effect of emotional information from eyes on empathy for pain: A subliminal ERP study. PLoS One 14: e0226211. doi: 10.1371/journal.pone.0226211
|
| [24] |
Perusquía-Hernández M, Ayabe-Kanamura S, Suzuki K (2019) Human perception and biosignal-based identification of posed and spontaneous smiles. PLoS One 14: e0226328. doi: 10.1371/journal.pone.0226328
|
| [25] |
Kilpeläinen M, Salmela V (2020) Perceived emotional expressions of composite faces. PLoS One 15: e0230039. doi: 10.1371/journal.pone.0230039
|
| [26] |
Borgomaneri S, Bolloni C, Sessa P, et al. (2020) Blocking facial mimicry affects recognition of facial and body expressions. PLoS One 15: e0229364. doi: 10.1371/journal.pone.0229364
|
| [27] |
Grueschow M, Jelezarova I, Westphal M, et al. (2020) Emotional conflict adaptation predicts intrusive memories. PLoS One 15: e0225573. doi: 10.1371/journal.pone.0225573
|
| [28] |
Wirth BE, Wentura D (2018) Furious snarling: Teeth-exposure and anxiety-related attentional bias towards angry faces. PLoS One 13: e0207695. doi: 10.1371/journal.pone.0207695
|
| [29] | Avenanti A (2019) Blocking facial mimicry affects recognition of facial and body expressions Available from: https://doi.org/10.17605/OSF.IO/CSUD3. |
| [30] |
Natu VS, Barnett MA, Hartley J, et al. (2016) Development of Neural Sensitivity to Face Identity Correlates with Perceptual Discriminability. J Neurosci 36: 10893-10907. doi: 10.1523/JNEUROSCI.1886-16.2016
|
| [31] |
Kungl MT, Bovenschen I, Spangler G (2017) Early Adverse Caregiving Experiences and Preschoolers' Current Attachment Affect Brain Responses during Facial Familiarity Processing: An ERP Study. Front Psychol 8: 2047. doi: 10.3389/fpsyg.2017.02047
|
| [32] |
Reynolds GD, Roth KC (2018) The Development of Attentional Biases for Faces in Infancy: A Developmental Systems Perspective. Front Psychol 9: 222. doi: 10.3389/fpsyg.2018.00222
|
| [33] |
Hartling C, Fan Y, Weigand A, et al. (2019) Interaction of HPA axis genetics and early life stress shapes emotion recognition in healthy adults. Psychoneuroendocrinology 99: 28-37. doi: 10.1016/j.psyneuen.2018.08.030
|
| [34] |
Ross P, Atkinson AP (2020) Expanding Simulation Models of Emotional Understanding: The Case for Different Modalities, Body-State Simulation Prominence, and Developmental Trajectories. Front Psychol 11: 309. doi: 10.3389/fpsyg.2020.00309
|
| [35] |
Recio G, Wilhelm O, Sommer W, et al. (2017) Are event-related potentials to dynamic facial expressions of emotion related to individual differences in the accuracy of processing facial expressions and identity? Cogn Affect Behav Neurosci 17: 364-380. doi: 10.3758/s13415-016-0484-6
|
| [36] |
Nonis F, Dagnes N, Marcolin F, et al. (2019) 3D Approaches and challenges in facial expression recognition algorithms—a literature review. Appl Sci 9: 3904. doi: 10.3390/app9183904
|
| [37] |
Allaert B, Bilasco IM, Djeraba C (2019) Micro and macro facial expression recognition using advanced Local Motion Patterns. IEEE Trans Affect Comput PP: 1. doi: 10.1109/TAFFC.2019.2949559
|
| [38] |
Kulke L, Feyerabend D, Schacht A (2020) A Comparison of the Affectiva iMotions Facial Expression Analysis Software With EMG for Identifying Facial Expressions of Emotion. Front Psychol 11: 329. doi: 10.3389/fpsyg.2020.00329
|
| [39] |
Colombo D, Fernández-Álvarez J, García Palacios A, et al. (2019) New Technologies for the Understanding, Assessment, and Intervention of Emotion Regulation. Front Psychol 10: 1261. doi: 10.3389/fpsyg.2019.01261
|
| [40] | Bastiaansen M, Oosterholt M, Mitas O, et al. (2020) An Emotional Roller Coaster: Electrophysiological Evidence of Emotional Engagement during a Roller-Coaster Ride with Virtual Reality Add-On. J Hosp Tour Res . |
| [41] |
Van Lier HG, Pieterse ME, Garde A, et al. (2020) A standardized validity assessment protocol for physiological signals from wearable technology: Methodological underpinnings and an application to the E4 biosensor. Behav Res Methods 52: 607-629. doi: 10.3758/s13428-019-01263-9
|
| [42] |
Mao Qr, Pan XY, Zhan YZ, et al. (2015) Using Kinect for real-time emotion recognition via facial expressions. Front Inform Tech El 16: 272-282. doi: 10.1631/FITEE.1400209
|
| [43] |
Ng HW, Nguyen VD, Vonikakis V, et al.Deep Learning for Emotion Recognition on Small Datasets using Transfer Learning. ACM Int Conf Multimodal Interact (2015) .443-449. doi: 10.1145/2818346.2830593
|
| [44] | Liu W, Zheng WL, Lu BL (2016) Emotion Recognition Using Multimodal Deep Learning. Neural Inf Process 9948: 521-529. |
| [45] |
Zhang TY, El Ali A, Wang C, et al. (2021) CorrNet: Fine-Grained Emotion Recognition for Video Watching Using Wearable Physiological Sensors. Sensors 21: 52. doi: 10.3390/s21010052
|
Figures(2) / Tables(3)

Justyna Gerłowska, Krzysztof Dmitruk, Konrad Rejdak. Facial emotion mimicry in older adults with and without cognitive impairments due to Alzheimer's disease[J]. AIMS Neuroscience, 2021, 8(2): 226-238. doi: 10.3934/Neuroscience.2021012







 DownLoad:
DownLoad: