Citation: Giovanni Messina. Islands of Fire. Stromboli in the documentary by Vittorio De Seta[J]. AIMS Geosciences, 2020, 6(3): 291-297. doi: 10.3934/geosci.2020017

| [1] | Mercatanti L, Messina G (2020) In cammino. Geografie di viaggio e pellegrinaggio. Torino: Nuova Trauben. |
| [2] | Lozato-Giotart JP (2003) Geografia del turismo. Dallo spazio visitato allo spazio consumato. Milano: FrancoAngeli. |
| [3] | Botta G (1989) Introduzione, In: Botta G, Cultura del viaggio, Ri-costruzione storico-geografica del territorio. Milano: Unicopli, 13-30. |
| [4] | Corna-Pellegrini G (1980) Geografia e percezione dell'ambiente: un rapporto da approfondire per la conoscenza e la programmazione del territorio. Riv Geogr Ital 87: 1-5. |
| [5] | Lando F (1993) Fatto e finzione. Geografia e letteratura. Milano: ETAS. |
| [6] | Cusimano G (1999) La costruzione del paesaggio siciliano: geografi e scrittori a confronto. Palermo: Università di Palermo. |
| [7] | Gavinelli D (2019) Geografia e letteratura: luoghi, scritture, paesaggi reali e immaginari. Introduzione, In Salvatori F, editor, L'apporto della Geografia fra rivoluzioni e riforme, Atti del XXXⅡ Congresso Geografico Italiano. Roma: AGEI, 597-604. |
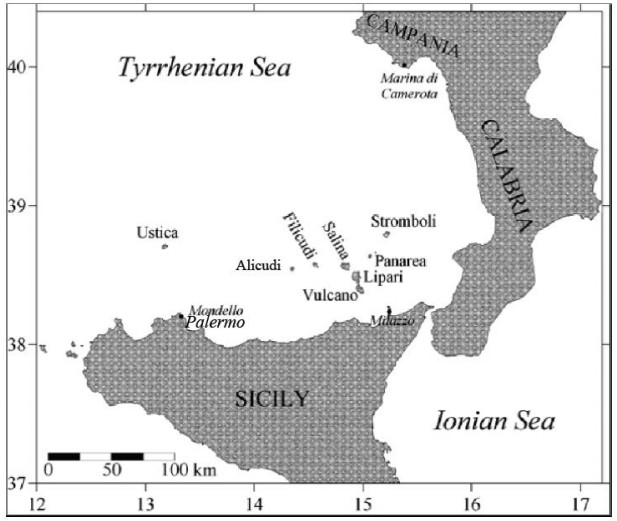
| [8] | Villari L (1980) The Aeolian Islands: an active volcanic arc in the Mediterranean sea. Catania: Istituto Internazionale di Vulcanologia-CNR. |
| [9] | Carveni P, Lo Giudice E, Rasà R (1986) Rischio vulcanico e sismico nell'arcipelago eoliano. Boll Accad Gioenia Sci Nat 19: 71-87. |
| [10] | Romagnoli C, Kokelaar P, Rossi PL, et al. (1993) The submarine extension of Sciara del Fuoco feature (Stromboli island): morphologic characterization. Acta Vulcanol 3: 91-98. |
| [11] |
Barberi F, Gandino A, Gioncada A, et al. (1994) The deep struc-ture of the Eolian arc (Filicudi-Panarea-Vulcano sector) in light of gravity, magnetic and volcanological data. J Volcanol Geotherm Res 61: 189-206. doi: 10.1016/0377-0273(94)90003-5

|
| [12] | Arena G (2003) Bibliografia generale delle Isole Eolie. Seconda edizione riveduta e continuata sino alla fine del XX secolo. Messina: Società Messinese di Storia patria. |
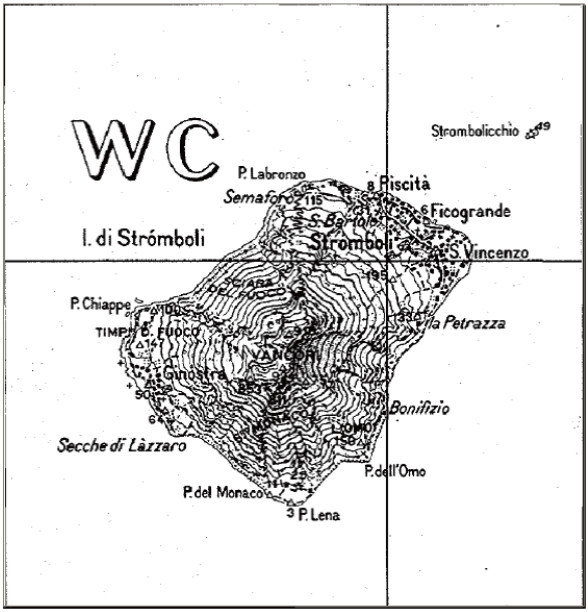
| [13] | Francalanci L, Manetti P, Peccerillo A (1986) Evoluzione vulcanologica e magmatologica dell'isola di Stromboli. Boll IGNV 1: 261-282. |
| [14] | Falsaperla S (1991) Stromboli. Acta Vulcanol 1: 272-275. |
| [15] | Napoleone G, Ripepe M, Saccorotti G, et al. (1993) The strombolian activity presently recorded at Stromboli. Acta Vulcanologica 3: 163-171. |
| [16] | Regione Siciliana-Assessorato dei Beni Culturali, Ambientali e della Pubblica Istruzione, Assessorato Territorio e Ambiente, Fondazione UNESCO per l'Italia (2009) Piano di Gestione UNESCO Isole Eolie. Available from: http://unescosicilia.it/wp/wp-content/uploads/2014/09/PdG-Eolie.pdf (Last visit, May 2020). |
| [17] | Dipartimento Protezione Civile (2015) Isola di Stromboli. Piano nazionale di emergenza a fronte di eventi vulcanici di rilevanza nazionale ex art. 107, comma 1, lettera f) del D.Lgs. 31 marzo 1998, n.112. Available from: http://www.prefettura.it/FILES/AllegatiPag/1196/PIANO_NAZIONALE_EMERGENZA_STROMBOLI_1.pdf (Last visit, May 2020). |
| [18] | Nicosia E (2012) Cineturismo e territorio. Un percorso attraverso i luoghi cinematografici. Bologna: Pàtron Editore. |
| [19] | Perini G (1970) Recenti modificazioni antropogeografiche nelle isole Eolie. Riv Geogr Ital 77: 393-430. |
Figures(2)

Giovanni Messina. Islands of Fire. Stromboli in the documentary by Vittorio De Seta[J]. AIMS Geosciences, 2020, 6(3): 291-297. doi: 10.3934/geosci.2020017







 DownLoad:
DownLoad: