Citation: Giorgia Liguori, Giuseppe Sortino, Giuseppe Gianguzzi, Paolo Inglese, Vittorio Farina. Evaluation of quality attributes and consumer preference of fresh or imported mangoes in Italy[J]. AIMS Agriculture and Food, 2018, 3(4): 426-440. doi: 10.3934/agrfood.2018.4.426
| [1] | Daniele Asioli, Rungsaran Wongprawmas, Erika Pignatti, Maurizio Canavari . Can information affect sensory perceptions? Evidence from a survey on Italian organic food consumers. AIMS Agriculture and Food, 2018, 3(3): 327-344. doi: 10.3934/agrfood.2018.3.327 |
| [2] | Cátia Morgado, José M. Pestana, Manuela M. Guerra, Carlos Brandão . Microbiological quality in convenient ready-to-eat vegetables during shelf life. AIMS Agriculture and Food, 2018, 3(4): 372-383. doi: 10.3934/agrfood.2018.4.372 |
| [3] | Valentina M. Merlino, Danielle Borra, Aurora Bargetto, Simone Blanc, Stefano Massaglia . Innovation towards sustainable fresh-cut salad production: Are Italian consumers receptive?. AIMS Agriculture and Food, 2020, 5(3): 365-386. doi: 10.3934/agrfood.2020.3.365 |
| [4] | Valentina Maria Merlino, Simone Blanc, Stefano Massaglia, Danielle Borra . Innovation in craft beer packaging: Evaluation of consumer perception and acceptance. AIMS Agriculture and Food, 2020, 5(3): 422-433. doi: 10.3934/agrfood.2020.3.422 |
| [5] | Valentina Maria Merlino, Filippo Brun, Alice Versino, Simone Blanc . Milk packaging innovation: Consumer perception and willingness to pay. AIMS Agriculture and Food, 2020, 5(2): 307-326. doi: 10.3934/agrfood.2020.2.307 |
| [6] | Saima Latif, Muhammad Sohaib, Sanaullah Iqbal, Muhammad Hassan Mushtaq, Muhammad Tauseef Sultan . Comparative evaluation of nutritional composition, phytochemicals and sensorial attributes of lyophilized vs conventionally dried Grewia asiatica fruit pulp powder. AIMS Agriculture and Food, 2025, 10(1): 247-265. doi: 10.3934/agrfood.2025013 |
| [7] | Carla Zarbà, Gaetano Chinnici, Biagio Pecorino, Gioacchino Pappalardo, Mario D'Amico . Recent scenarios in Italy on fresh-cut products in the Covid-19 context. AIMS Agriculture and Food, 2022, 7(2): 403-425. doi: 10.3934/agrfood.2022026 |
| [8] | Marcelo Augusto de Carvalho, Cíntia Sorane Good Kitzberger, Altamara Viviane de Souza Sartori, Marta de Toledo Benassi, Maria Brígida dos Santos Scholz, Clandio Medeiros da Silva . Free choice profiling sensory analysis and principal component analysis as tools to support an apple breeding program. AIMS Agriculture and Food, 2020, 5(4): 769-784. doi: 10.3934/agrfood.2020.4.769 |
| [9] | Giacomo Staffolani, Giulia Chiaraluce, Deborah Bentivoglio, Bruno Vodo, Pier Paolo Miglietta, Adele Finco . Blockchain for the valorization of Made in Italy extra virgin olive oil: A discrete choice experiment on young consumers. AIMS Agriculture and Food, 2025, 10(3): 596-617. doi: 10.3934/agrfood.2025030 |
| [10] | Michelle Marais, Henry Jordaan, Willem Abraham Lombard, Yonas T. Bahta . Assessing the potential of a niche market for wool products in South Africa. AIMS Agriculture and Food, 2024, 9(1): 108-128. doi: 10.3934/agrfood.2024007 |
Mango (Mangifera indica L.) is one of the major fruit crop in tropical and subtropical regions. Among tropical fruits, mango production is second behind bananas (more than 113 million tons) reaching 46 million tons [1] that are mainly shipped to export markets [2].
Mango production is mostly concentrated in India, China, Thailand, Indonesia, Philippines, Pakistan and Mexico, but in the last decades its cultivation has been moving also outside the traditional geographical regions to Australia, Central and South America, South-East Asia, Hawaii, Egypt, Israel, South Africa, and Europe, especially for export [3].
The favorable climate of the Mediterranean basin areas is suitable for mango cultivation, particularly in Egypt, Israel, Spain, and in Italy, especially in Sicily [4,5,6].
Mango is a climacteric fruit with a relatively short shelf-life. Usually, fruit from tropical Countries and shipped to the European market are collected precociously, before complete ripening, at mature-green stage, when they are hard and green, and then are ripen progressively after harvest [5]. This practice improves storability and transportability but generally produces fruits lacking developed characteristic color, aroma and taste [5]. The most popular exported mango cultivars are Kent, Tommy Atkins, Haden, and Keitt; less known cultivars such as Ataulfo, Amelie, Francis and Osteen are now being widely accepted all over the world [1,2].
Mango fruit subjected to long transportation distances are usually harvested at the mature-green stage, firm and green but physiologically mature, whereas fruit sent to local markets or air-shipped are harvested at mature-ripe stage [7,8]. The ripening process in mature-green fruit takes within 9–14 days and includes starch to sugar conversion, decreased acidity and increased carotenoids and aroma volatiles; mature-ripe fruits shortly decline within 6 days at room temperature [9].
The largest import markets for fresh and processed tropical fruits belong to the European Union followed by the United States of America [10]; in the last decades, consumers demand for tropical fruits increased, due to several reasons such as, health consciousness, population growth of ethnic minorities in Europe and through international travel and global communication [11].
Several researches investigated the complex interactions of different factors influencing consumers choices and preferences in terms of fruits and vegetables, but only few of that were focused on tropical fruits [12], and there is a lack of data in terms of consumer and sensory analysis on fresh local production and imported mango fruits in Europe. Appearance, freshness and peel color are relevant fruit quality parameters and play a significant role in consumer mango fruit acceptability and preference [13]. Generally, during ripening, mango varieties change color from green to yellow or orange, often showing a red blush [8]. Sensory profile of mango fruits, especially color, taste, aroma and flavor, have a great impact on consumers choices [7].
Sensory experiences play a predominant role in shaping consumers satisfaction and hence acceptance of tropical fruits they are not familiar with [11]. Especially because unfamiliarity with tropical fruits and the perceived high prices are the main barriers for purchase and consumption in Europe.
The present study was conducted to evaluate quality attributes, sensory quality and consumer preference of local fresh and imported mango fruits in Italy.
Mango fruit (cv Keitt, Kent and Osteen) produced in Italy, were harvested from a commercial orchard, located at Furiano, province of Messina (Sicily, Italy; 38°3' N, 14°33' E; 5 m a.s.l.). Fruit were hand-picked at mature-green (GR) and mature-ripe (MR) stage, suitable for the fresh fruit market, using skin color as maturity index [5,14,15]. Immediately after harvest weight, firmness, total soluble solids content (TSS) and titratable acidity (TA) were measured on 6 replicates of 5 fruit.
Mango fruit imported from abroad (cv Keitt, Kent and Osteen) were collected from 2 different large-scale organized distribution markets. On the same day, fruit with external injuries were eliminated, while the rest were presorted by cultivar, using non-destructive (color index) and destructive (firmness) criteria, into GR and MR categories to facilitate the qualitative and descriptive analysis. Imported mango fruit were analyzed in terms of weight, firmness, total soluble solids content (TSS) and titratable acidity (TA) were measured on 6 replicates of 5 fruit. 50% of GR mango fruits collected from 2 different large-scale organized markets (LD) were immediately analyzed and evaluated; 50% of GR remaining mango fruits were stored at room temperature (20 ℃) for 4–8 days until they reached MR stage and then were submitted to analysis.
Fruit (n = 30) were analyzed at harvest and when were collected from the two large-scale organized distribution market. Fruit weight was determined using a digital scale. Firmness, expressed in Newton (N), was measured on opposite cheeks of each fruit with a digital penetrometer (mod. 53205, Tr Turoni, Forlì, Italy) incorporating an 8 mm diameter probe, after removal of a small piece of peel. A wedge-shaped slice of flesh was taken longitudinally from each fruit and ten fruit wedges were peeled and juiced. Total soluble solids (TSS) were determined by digital refractometer (Palette PR-32, Atago Co., Ltd) and titratable acidity (TA) was measured by titration of 10 mL juice with 0.1 N NaOH to pH 8.1 (mod. S compact titrator, Crison Instruments, Barcelona, Spain) and expressed as % citric acid, which is the major acid in mango fruit [16]. Fruits were also checked for the presence of decay, whose incidence was expressed as a percentage.
Fruits (n = 5) from local grower and imported from abroad were subjected to sensory evaluation at GR and MR stage.
The sensory profile was constructed by a semi-trained panel made of 10 judges that in a few preliminary meetings, by using commercial fruit, generated a list of descriptors [17]. Semi-trained panel is made up of people normally familiar with mango fruit, this kind of panel is capable of discriminating differences and communicating their reactions, though it may not have been formally trained; furthermore, a semi-trained panelist judgement will be closer to that of the average consumer [18].
Sensory analysis was focused on appearance (2 descriptors), tactile handfeel (1 descriptor), aroma (6 descriptors), flavor (6 descriptors), taste and tactile (5 descriptors) and rheological descriptors, focused on juiciness perceived in the mouth (1 descriptor) (Table 1) [5].
| Descriptors | Definition |
| Appearance | |
| Skin color | Predominant color of the main surface of the mango |
| Flesh color | Color of the mango flesh (from yellow to dark and intense orange) |
| Tactile handfeel | |
| Consistency to cut | Resistance of the fruit to the cut, evaluated manually |
| Aroma | |
| Sea odor | Characteristic aroma of sea perceived with the sense of smell |
| Peach odor | Characteristic aroma of peach perceived with the sense of smell |
| Exotic fruit odor | Characteristic aroma of exotic fruit perceived with the sense of smell |
| Medicinal odor | Characteristic aroma of medicinal perceived with the sense of smell |
| Cheese odor | Characteristic aroma of cheese perceived with the sense of smell |
| Burned oil | Characteristic aroma of burned oil perceived with the sense of smell |
| Flavor | |
| Sea flavor | Characteristic aroma of sea perceived with the swallowing |
| Peach flavor | Characteristic aroma of peach perceived with the swallowing |
| Exotic fruit flavor | Characteristic aroma of exotic fruit perceived with the swallowing |
| Medicinal flavor | Characteristic aroma of medicinal perceived with the swallowing |
| Cheese flavor | Characteristic aroma of cheese perceived with the swallowing |
| Burned oil flavor | Characteristic aroma of burned oil perceived with the swallowing |
| Taste and tactile in mouth | |
| Acid | Basic taste on tongue stimulated by acids |
| Fiber in the flesh | Amount of fibers in the sample after a bite |
| Mealiness | Gritty, sandy texture, dry not juicy |
| Bitter | Taste on the tongue stimulated by bitter compounds |
| Sweet | Taste on the tongue stimulated by sugars and high potency sweeteners |
| Rheological | |
| Juiciness | The amount of juice/moisture perceived in the mouth |
 DownLoad: CSV
DownLoad: CSVAbout 50 g sample were dispensed into a small plastic plate with a 3-digit code on the side and served to the judges [5].The different descriptors were quantified using an eight point intensity scale where the digit 1 indicates the descriptor absence while the digit 8 the full intensity. The order of presentation was randomized between judges and water was provided for rinsing between samples [5].
An "in-store" consumer test was conducted on the two maturity stages (GR and MR) of the three mango cultivars [19,20]. Hundred and fifty (n = 150) regular or occasional consumers were surveyed at 2 major large-scale organized distribution market in Palermo (IT). Target population was selected according to socio-demographic and psychographic marketing variables for consumer stratification (50% females, 50% males, range of age between 20 and 75) [21].
The samples (one sample from each cultivar, maturity stage and origin) were served, monadically, in plastic cups coded with 3-digit algorithms, in random order at room temperature (20 ℃). Before tasting the samples, the consumers were asked about any possible allergic reactions to mango fruits. Each sample was subjected to consumer test for external appearance, firmness, taste, sweetness, exotic fruit aroma and overall acceptance; the acceptance was determined using a linear 8-point hedonic scale (1 = dislike extremely to 8 = like extremely) [22]. The order of presentation was randomized between the consumers, water was provided for rinsing between samples.
Data were submitted to analysis of variance (ANOVA); means separation was performed using Tukey's test at P ≤ 0.05. The statistical analysis was carried out using Systat v.10 (Systat, USA).
Local mango fruits of each cultivar showed significantly higher weight in both maturity stage (GR and MR), most likely due to the early harvest of the imported fruits (Table 2).
| Cultivar (Local and imported) | Weight (g) | SE | Firmness (N) | SE | TSS (Brix) | SE | TA (g L-1 citric acid) | SE | ||||||||
| Osteen GR local | 626 | ± | 7 | a | 28.19 | ± | 0.30 | c | 15.75 | ± | 0.59 | a | 0.58 | ± | 0.01 | b |
| Osteen GR LD1 | 556 | ± | 5 | b | 83.84 | ± | 0.16 | a | 8.90 | ± | 0.45 | b | 0.85 | ± | 0.08 | a |
| Osteen GR LD2 | 529 | ± | 4 | b | 74.04 | ± | 0.21 | b | 8.40 | ± | 0.52 | b | 0.79 | ± | 0.07 | a |
| Osteen MR local | 606 | ± | 8 | a | 10.04 | ± | 0.03 | b | 17.98 | ± | 0.42 | a | 0.26 | ± | 0.01 | b |
| Osteen MR LD1 | 506 | ± | 4 | b | 9.80 | ± | 0.05 | b | 11.50 | ± | 0.42 | b | 0.51 | ± | 0.05 | a |
| Osteen MR LD2 | 479 | ± | 4 | c | 15.20 | ± | 0.04 | a | 11.40 | ± | 0.39 | b | 0.45 | ± | 0.05 | a |
| Keitt GR local | 680 | ± | 5 | a | 33.83 | ± | 0.12 | c | 15.90 | ± | 0.29 | a | 0.54 | ± | 0.01 | b |
| Keitt GR LD1 | 573 | ± | 5 | b | 61.98 | ± | 0.13 | a | 9.45 | ± | 0.63 | b | 0.83 | ± | 0.08 | a |
| Keitt GR LD2 | 565 | ± | 6 | b | 56.14 | ± | 0.09 | b | 9.80 | ± | 0.54 | b | 0.86 | ± | 0.06 | a |
| Keitt MR local | 624 | ± | 6 | a | 13.72 | ± | 0.05 | a | 18.80 | ± | 0.26 | a | 0.41 | ± | 0.01 | a |
| Keitt MR LD1 | 554 | ± | 5 | b | 9.90 | ± | 0.04 | b | 11.23 | ± | 0.32 | c | 0.47 | ± | 0.02 | a |
| Keitt MR LD2 | 540 | ± | 5 | b | 4.12 | ± | 0.02 | c | 12.10 | ± | 0.44 | b | 0.32 | ± | 0.01 | b |
| Kent GR local | 686 | ± | 5 | a | 22.65 | ± | 0.08 | c | 14.05 | ± | 0.46 | a | 0.55 | ± | 0.02 | b |
| Kent GR LD1 | 593 | ± | 5 | b | 73.94 | ± | 0.07 | b | 9.20 | ± | 0.65 | b | 0.80 | ± | 0.07 | a |
| Kent GR LD2 | 614 | ± | 5 | c | 87.28 | ± | 0.09 | a | 8.50 | ± | 0.53 | b | 0.74 | ± | 0.08 | a |
| Kent MR local | 653 | ± | 5 | a | 11.77 | ± | 0.05 | a | 15.43 | ± | 0.41 | a | 0.58 | ± | 0.01 | c |
| Kent MR LD1 | 502 | ± | 5 | b | 7.84 | ± | 0.08 | c | 11.32 | ± | 0.65 | b | 0.69 | ± | 0.06 | b |
| Kent MR LD2 | 456 | ± | 5 | c | 9.81 | ± | 0.04 | b | 10.50 | ± | 0.58 | c | 0.85 | ± | 0.10 | a |
| * Values labelled with a different letter in the same column are significantly different for each ripening stage (Tukey's test at P ≤ 0.05). | ||||||||||||||||
DownLoad: CSVIn any case, firmness, TSS and TA were affected by maturity stage (GR and MR) in all mango fruits.
Osteen, Keitt and Kent local mango fruits showed a firmness percentage decrease of 64%, 59% and 48%, respectively, between GR and MR stage (Table 2). Osteen, Keitt and Kent mango imported fruits showed higher firmness percentage decrease between GR and MR than local ones, with values around 87% (Table 2).
GR local mango fruits showed significantly higher values of TSS in each cultivar than imported ones. Indeed, Osteen, Keitt and Kent GR mango local fruits showed TSS values of 45%, 39% and 37% higher than imported ones, respectively. Osteen, Keitt and Kent MR local mango fruits showed a similar behavior with TSS values of 36%, 38% and 29% higher than imported ones (Table 2). GR and MR Osteen, Keitt and Kent imported mango fruit, in most cases, showed higher TA values than the local mango fruits (Table 2). Our data confirm that the early harvest of imported mango fruits improves transportability but affect negatively fruit quality parameters as firmness, TSS and TA.
MR imported mango fruit were affected by flesh disorders, particularly, 30% of MR Keitt imported mango fruits were affected by flesh disorders (browning), losing its marketability (data not shown). Mango imported fruit flesh disorders were probably caused by chilling injuries due to the application of temperature below 10–13 ℃ during long transportation and retail storage [18].
Indeed, local mango fruits were not affected by flesh disorders.
Panelists preferred Osteen, Keitt and Kent local mango fruits at both maturity stages (Figures 1–3); in particular, Osteen mango local fruits get the higher scores in terms of skin color, juiciness, exotic fruit flavor, exotic fruit odor and overall acceptance (Figure 1). Indeed, GR Kent mango imported fruits get the lowest scores in most of the descriptors, particularly in terms of overall acceptance (Figure 3A).
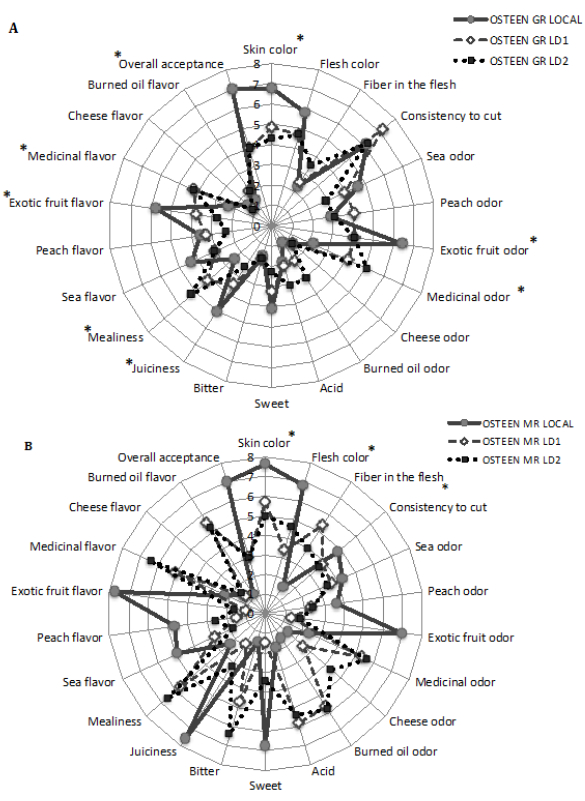 Figure 1. Sensory analysis of mature-green (GR) (A) and mature-ripe (MR) (B) Osteen local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits. Data are Mean of 5 fruit for each ripening stage.
Figure 1. Sensory analysis of mature-green (GR) (A) and mature-ripe (MR) (B) Osteen local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits. Data are Mean of 5 fruit for each ripening stage.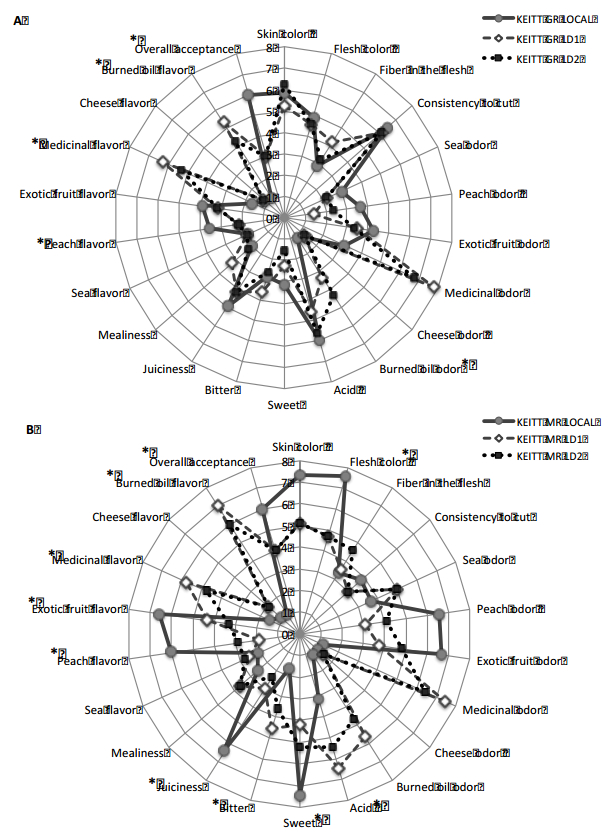 Figure 2. Sensory analysis of mature-green (GR) (A) and mature-ripe (MR) (B) Keitt local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits. Data are Mean of 5 fruit for each ripening stage.
Figure 2. Sensory analysis of mature-green (GR) (A) and mature-ripe (MR) (B) Keitt local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits. Data are Mean of 5 fruit for each ripening stage.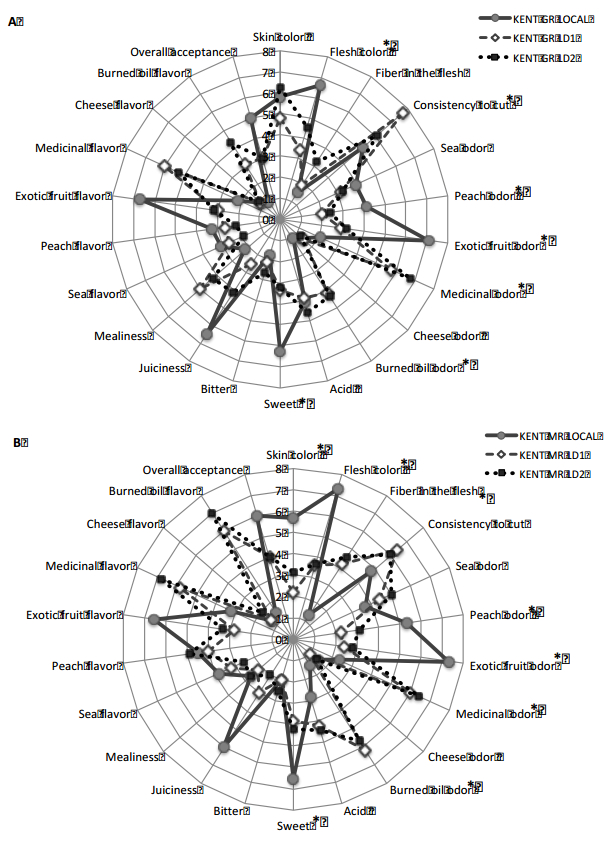 Figure 3. Sensory analysis of mature-green (GR) (A) and mature-ripe(MR) (B) Kent local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits. Data are Mean of 5 fruit for each ripening stage.
Figure 3. Sensory analysis of mature-green (GR) (A) and mature-ripe(MR) (B) Kent local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits. Data are Mean of 5 fruit for each ripening stage.MR Osteen, Keitt and Kent local mango fruits showed higher scores in most of the descriptors, as well as, skin and flesh color, peach flavor and odor, sweetness, juiciness, exotic fruit flavor and odor etc.; and the lowest scores in terms of off-flavor and off-odor, than imported mango fruits (Figures 1B, 2B and 3B).
MR Osteen, Keitt and Kent mango imported fruits showed higher scores in terms of off-flavor (medicinal flavor and burned oil flavor) and off-odor (medicinal odor, burned oil odor), than local ones (Figures 1B, 2B and 3B). Osteen, Keitt and Kent mango imported fruits showed a noticeable increase in terms of medicinal odor, burned oil odor, medicinal flavor and burned oil flavor between GR and MR stage (Figures 1–3).
Sensory analysis was consistent with the analytical measurements, the higher TSS values of MR local mango fruits was perceived by the panelist. MR local mango fruit quality parameters measured were in line with the scores obtained in terms of overall acceptance.
The in-store consumer test population (n = 150) consisted of 50 % female and 50% male; 68% of the consumer population was between 20 and 60 years old and 32% was between 61 and 75 years old [23].
The consumer liking of Osteen, Keitt and Kent local and imported mango fruits was affected by maturity stage (GR and MR) and by cultivar; in any case consumers preferred local mango fruits, result in line with sensory analysis (Figures 4–6). Osteen local mango fruits had the higher consumer acceptance at both maturity stage (GR and MR), with scores of 40% and 47% respectively higher than imported ones, in terms of overall acceptance (Figure 4). The overall acceptance average degree of liking for Osteen, Keitt and Kent local mango fruits was "moderately", indeed, for imported mango fruits was "dislike lightly" (Figures 4–6).
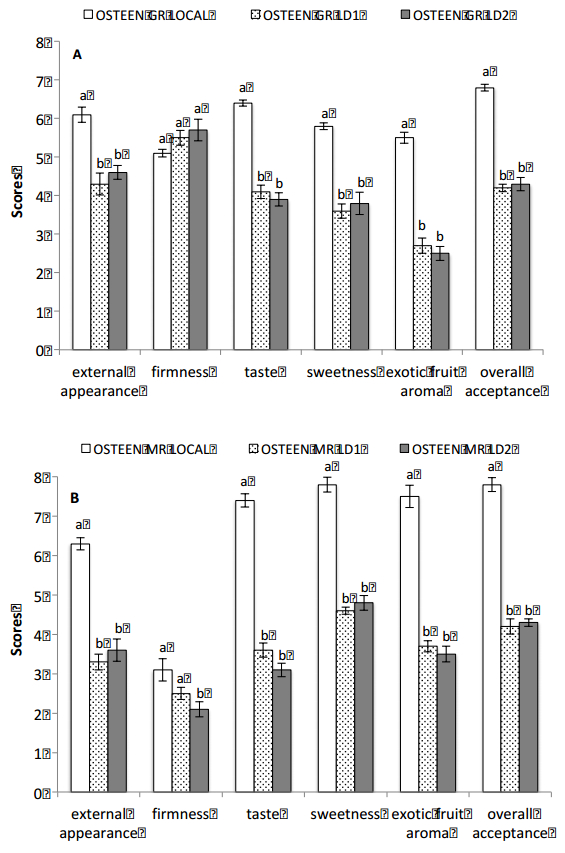 Figure 4. Consumer acceptance of mature-green (GR) (A) and mature-ripe (MR) (B) Osteen local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits.
Figure 4. Consumer acceptance of mature-green (GR) (A) and mature-ripe (MR) (B) Osteen local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits.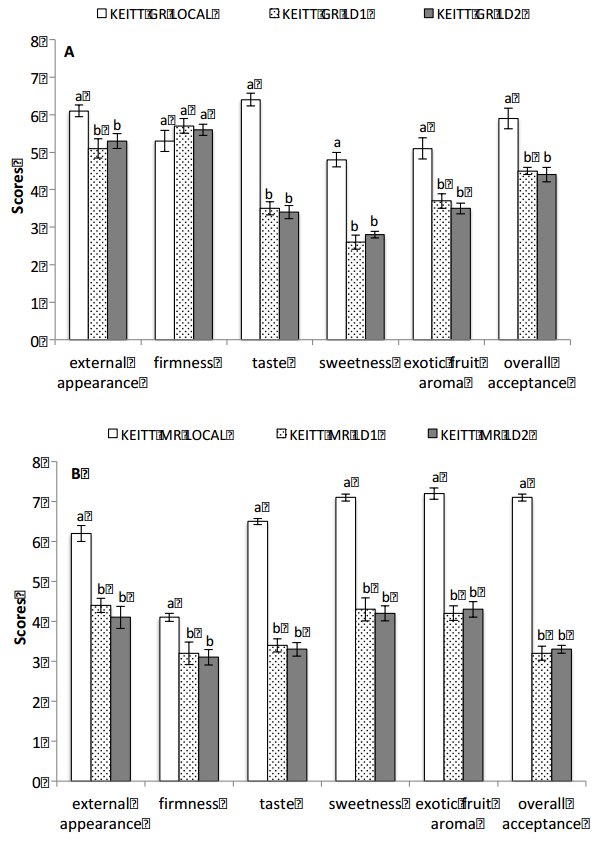 Figure 5. Consumer acceptance of mature-green (GR) (A) and mature-ripe (MR) (B) Keitt local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits.
Figure 5. Consumer acceptance of mature-green (GR) (A) and mature-ripe (MR) (B) Keitt local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits.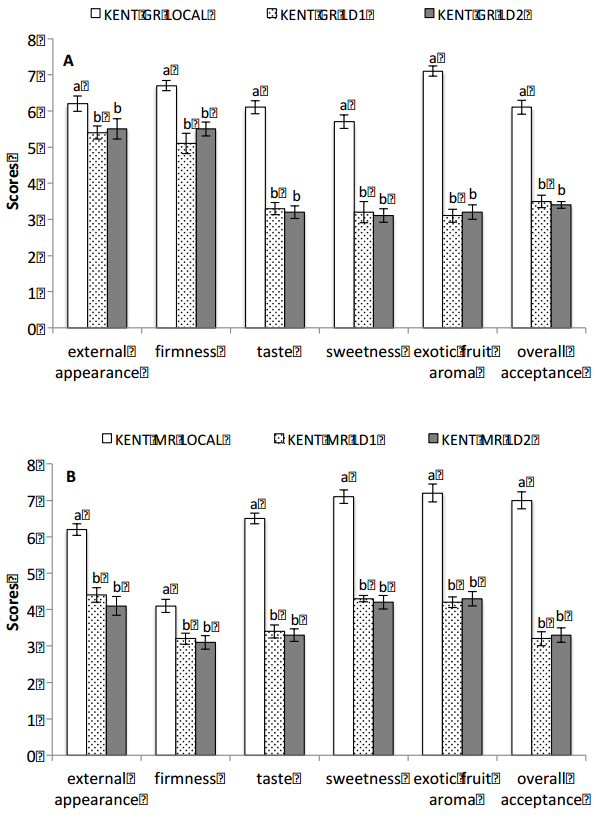 Figure 6. Consumer acceptance of mature-green (GR) (A) and mature-ripe (MR) (B) Kent local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits.
Figure 6. Consumer acceptance of mature-green (GR) (A) and mature-ripe (MR) (B) Kent local and imported (LD1 and LD2) mango (Mangifera indica L.) fruits.Significant differences were observed between MR Osteen, Keitt and Kent local and imported mango fruits in all the descriptors; in GR Osteen and Keitt ones, only the firmness score was not significantly different (Figures 4–6). A noticeable liking increase in terms of overall acceptance was observed in all the mango cultivar (local and imported) between GR and MR stage (Figures 4–6).
Osteen, Keitt and Kent local mango fruits were particularly preferred by consumer with high score for taste and exotic fruit aroma (Figures 4–6).
Our study showed that local fresh mango fruits were preferred by the panelist and the consumers, despite the fruits did not come from their origin tropical countries; probably due to the precociously harvest of imported mango fruits. Furthermore, our data confirm the high potential of Southern Italy for mango fruit production.
Local mango fruits showed higher size; higher level of TSS and the best scores in terms of taste in both maturity stages (GR and MR), in particular the data obtained on MR local mango fruits showed that ripening is strictly correlated to sensory perception of consumers/panelist and influenced consumer preferences and potentially choices.
Sensory experiences play a predominant role in consumers' satisfaction and hence the acceptance of tropical fruit in EU markets. Our study brings out some important factors dealing with the relationship between taste and product acceptance; mango consumer taste scores acceptance resulted strictly connected.
Until now, a large number of consumers are still unfamiliar with fresh local mango fruits and for that reason, producers and retailers should promote educational initiative to inform people about tropical local production and to improve the large potential for the fresh mango market in Italy.
All authors declare no conflicts of interest in this paper.
| [1] | FAO (2016) Food and Agriculture Organization of the United Nations>-FAO Statistics. Rome, Italy. Accessed 2018, October 17. Available from: http://faostat.fao.org/. |
| [2] | Nassur R, Gonzalez-Moscoso S, Crisosto GM et al. (2015) Describing quality and sensory attributes of 3 mango (Mangifera indica L.) cultivars at 3 ripeness stages based on firmness. J Food Sci 80: S2055–S2063. |
| [3] | Tharanathan RN, Hosakote YM, Prabha TN (2006) Mango (Mangifera indica L.), "The king of fruits"-An overview. Food Rev Int 22: 95 |
| [4] | Sortino G, Caviglia V, Liguori G, Quality changes of tropical and subtropical fresh-cut fruits mix in modified atmosphere packaging. Chem Eng Trans 58: 397–402. |
| [5] |
Farina V, Antonio D, Mazzaglia A, et al. (2017) Chemical-physical and nutritional characteristics of mature-green and mature-ripe 'Kensington Pride' mango fruit cultivated in Mediterranean area during cold storage. Fruits 72: 221–229. doi: 10.17660/th2017/72.4.4

|
| [6] | Mossad A, El Helew WK, Elsheshtawy H, et al. (2016) Mass modelling by dimension attributes for Mango (Mangifera indica cv. Zebdia) relevant to post-harvest and food plants engineering. Agric Eng Int CIGR J 18: 219–229. |
| [7] |
Nunes MCN, Emond JP, Brecht JK, et al. (2007) Quality curves for mango fruit stored at chilling and non chilling temperatures. J Food Qual 30: 104–120. doi: 10.1111/j.1745-4557.2007.00109.x
|
| [8] | Medlicott AP, Reynolds SB, New SW, et al. (1988) Harvest maturity effects on mango fruit ripening. Trop Agric 65: 153–157. |
| [9] | Kalra SK, Tandon DK, Singh BP Handbook of fruit science and technology, In: Salunkhe DK, Kadam SS, Production, Composition, Storage and Processing, Eds., Marcel Dekker Inc, New York: 123–170. |
| [10] | FAO (2003) Food and Agriculture Organization of the United Nations-Medium-term prospects for agricultural commodities. FAO commodities and trade technical papers No.1. Rome, Italy: FAO. |
| [11] |
Sabbe S, Verbeke W, Van Damme P (2008) Familiarity and purchasing intention of Belgian consumers for fresh and processed tropical fruit products. Brit Food J 110: 805–818. doi: 10.1108/00070700810893331
|
| [12] |
Sabbe S, Verbeke W, Van Damme P (2009) Confirmation/disconfirmation of consumers' expectations about fresh and processed tropical fruit products. Int J Food Sci Technol 44: 539–551. doi: 10.1111/j.1365-2621.2008.01842.x
|
| [13] | Akhtar S, Mahmood S, Naz S, et al. (2009) Sensory evaluation of mangoes (Mangifera indica L.) grown in different regions of Pakistan. Pakistan J Bot 41: 2821–2829. |
| [14] | Cheema GS, Dani PG (1934) Report on export of mango to Europe in 1932-3. Bombay Dep Agr Bull 170: 259–325. |
| [15] | Palapol Y, Ketsa S, Stevenson D, et al. (2009) Colour development and quality of mangosteen (Garcinia mangostana L.) fruit during ripening and after harvest. Postharv Biol Technol 51: 349–353. |
| [16] | Jain NL, Krishnamurthy GV, Lal GC (1959) Non-volatile organic acids in unripe pickling mangoes and salted mango slices by paper chromatography. Food Sci 3: 115–118. |
| [17] |
Ruiz-Capillas C, Moral A (2003) Use of semitrained panel members in the sensory evaluation of hake (Merluccius merluccius L.) analyzed statistically. J Food Quality 26: 181–195. doi: 10.1111/j.1745-4557.2003.tb00237.x
|
| [18] | Liguori G, Inglese P, Corona O, et al. (2017) Effects of 1-Methylcyclopropene on postharvest quality traits, antioxidant activity and ascorbic acid content of mature-ripe mango fruits. Fruits 72: 238–246. |
| [19] | Crisosto CH, Bremer V, Ferguson L, et al. (2010) Evaluating quality attributes of four fresh fig (Ficus carica L.) cultivars harvested at two maturity stages. HortSci 45: 707–710. |
| [20] | Sortino G, Allegra A, Inglese P, et al. (2016) Influence of an evoked pleasant consumption context on consumers' hedonic evaluation for minimally processed cactus pear (Opuntia ficus-indica) fruit. Acta Hortic 1141: 327–334. |
| [21] | Liguori G, Sortino G, De Pasquale C, et al. (2015) Effects of modified atmosphere packaging on quality parameters of minimally processed table grapes during cold storage. Advances Hort Sci 29: 152–154. |
| [22] | Liguori G, Sortino G, Gentile C, et al. (2018) Quality changes in fresh-cut mango cubes submitted to different gas partial pressure of active MAPs. Acta Hortic 1194: 1181–1186. |
| [23] | Ingrassia M, Chironi S, Allegra A, et al. (2017) Consumer preferences for fig fruit (Ficus carica L.) quality attributes and postharvest storage at low temperature by in-store survey and focus group. Acta Hortic 1173: 383–388. |






Figures(6) / Tables(2)

Giorgia Liguori, Giuseppe Sortino, Giuseppe Gianguzzi, Paolo Inglese, Vittorio Farina. Evaluation of quality attributes and consumer preference of fresh or imported mangoes in Italy[J]. AIMS Agriculture and Food, 2018, 3(4): 426-440. doi: 10.3934/agrfood.2018.4.426

| Descriptors | Definition |
| Appearance | |
| Skin color | Predominant color of the main surface of the mango |
| Flesh color | Color of the mango flesh (from yellow to dark and intense orange) |
| Tactile handfeel | |
| Consistency to cut | Resistance of the fruit to the cut, evaluated manually |
| Aroma | |
| Sea odor | Characteristic aroma of sea perceived with the sense of smell |
| Peach odor | Characteristic aroma of peach perceived with the sense of smell |
| Exotic fruit odor | Characteristic aroma of exotic fruit perceived with the sense of smell |
| Medicinal odor | Characteristic aroma of medicinal perceived with the sense of smell |
| Cheese odor | Characteristic aroma of cheese perceived with the sense of smell |
| Burned oil | Characteristic aroma of burned oil perceived with the sense of smell |
| Flavor | |
| Sea flavor | Characteristic aroma of sea perceived with the swallowing |
| Peach flavor | Characteristic aroma of peach perceived with the swallowing |
| Exotic fruit flavor | Characteristic aroma of exotic fruit perceived with the swallowing |
| Medicinal flavor | Characteristic aroma of medicinal perceived with the swallowing |
| Cheese flavor | Characteristic aroma of cheese perceived with the swallowing |
| Burned oil flavor | Characteristic aroma of burned oil perceived with the swallowing |
| Taste and tactile in mouth | |
| Acid | Basic taste on tongue stimulated by acids |
| Fiber in the flesh | Amount of fibers in the sample after a bite |
| Mealiness | Gritty, sandy texture, dry not juicy |
| Bitter | Taste on the tongue stimulated by bitter compounds |
| Sweet | Taste on the tongue stimulated by sugars and high potency sweeteners |
| Rheological | |
| Juiciness | The amount of juice/moisture perceived in the mouth |
DownLoad: CSV| Cultivar (Local and imported) | Weight (g) | SE | Firmness (N) | SE | TSS (Brix) | SE | TA (g L-1 citric acid) | SE | ||||||||
| Osteen GR local | 626 | ± | 7 | a | 28.19 | ± | 0.30 | c | 15.75 | ± | 0.59 | a | 0.58 | ± | 0.01 | b |
| Osteen GR LD1 | 556 | ± | 5 | b | 83.84 | ± | 0.16 | a | 8.90 | ± | 0.45 | b | 0.85 | ± | 0.08 | a |
| Osteen GR LD2 | 529 | ± | 4 | b | 74.04 | ± | 0.21 | b | 8.40 | ± | 0.52 | b | 0.79 | ± | 0.07 | a |
| Osteen MR local | 606 | ± | 8 | a | 10.04 | ± | 0.03 | b | 17.98 | ± | 0.42 | a | 0.26 | ± | 0.01 | b |
| Osteen MR LD1 | 506 | ± | 4 | b | 9.80 | ± | 0.05 | b | 11.50 | ± | 0.42 | b | 0.51 | ± | 0.05 | a |
| Osteen MR LD2 | 479 | ± | 4 | c | 15.20 | ± | 0.04 | a | 11.40 | ± | 0.39 | b | 0.45 | ± | 0.05 | a |
| Keitt GR local | 680 | ± | 5 | a | 33.83 | ± | 0.12 | c | 15.90 | ± | 0.29 | a | 0.54 | ± | 0.01 | b |
| Keitt GR LD1 | 573 | ± | 5 | b | 61.98 | ± | 0.13 | a | 9.45 | ± | 0.63 | b | 0.83 | ± | 0.08 | a |
| Keitt GR LD2 | 565 | ± | 6 | b | 56.14 | ± | 0.09 | b | 9.80 | ± | 0.54 | b | 0.86 | ± | 0.06 | a |
| Keitt MR local | 624 | ± | 6 | a | 13.72 | ± | 0.05 | a | 18.80 | ± | 0.26 | a | 0.41 | ± | 0.01 | a |
| Keitt MR LD1 | 554 | ± | 5 | b | 9.90 | ± | 0.04 | b | 11.23 | ± | 0.32 | c | 0.47 | ± | 0.02 | a |
| Keitt MR LD2 | 540 | ± | 5 | b | 4.12 | ± | 0.02 | c | 12.10 | ± | 0.44 | b | 0.32 | ± | 0.01 | b |
| Kent GR local | 686 | ± | 5 | a | 22.65 | ± | 0.08 | c | 14.05 | ± | 0.46 | a | 0.55 | ± | 0.02 | b |
| Kent GR LD1 | 593 | ± | 5 | b | 73.94 | ± | 0.07 | b | 9.20 | ± | 0.65 | b | 0.80 | ± | 0.07 | a |
| Kent GR LD2 | 614 | ± | 5 | c | 87.28 | ± | 0.09 | a | 8.50 | ± | 0.53 | b | 0.74 | ± | 0.08 | a |
| Kent MR local | 653 | ± | 5 | a | 11.77 | ± | 0.05 | a | 15.43 | ± | 0.41 | a | 0.58 | ± | 0.01 | c |
| Kent MR LD1 | 502 | ± | 5 | b | 7.84 | ± | 0.08 | c | 11.32 | ± | 0.65 | b | 0.69 | ± | 0.06 | b |
| Kent MR LD2 | 456 | ± | 5 | c | 9.81 | ± | 0.04 | b | 10.50 | ± | 0.58 | c | 0.85 | ± | 0.10 | a |
| * Values labelled with a different letter in the same column are significantly different for each ripening stage (Tukey's test at P ≤ 0.05). | ||||||||||||||||
DownLoad: CSV| Descriptors | Definition |
| Appearance | |
| Skin color | Predominant color of the main surface of the mango |
| Flesh color | Color of the mango flesh (from yellow to dark and intense orange) |
| Tactile handfeel | |
| Consistency to cut | Resistance of the fruit to the cut, evaluated manually |
| Aroma | |
| Sea odor | Characteristic aroma of sea perceived with the sense of smell |
| Peach odor | Characteristic aroma of peach perceived with the sense of smell |
| Exotic fruit odor | Characteristic aroma of exotic fruit perceived with the sense of smell |
| Medicinal odor | Characteristic aroma of medicinal perceived with the sense of smell |
| Cheese odor | Characteristic aroma of cheese perceived with the sense of smell |
| Burned oil | Characteristic aroma of burned oil perceived with the sense of smell |
| Flavor | |
| Sea flavor | Characteristic aroma of sea perceived with the swallowing |
| Peach flavor | Characteristic aroma of peach perceived with the swallowing |
| Exotic fruit flavor | Characteristic aroma of exotic fruit perceived with the swallowing |
| Medicinal flavor | Characteristic aroma of medicinal perceived with the swallowing |
| Cheese flavor | Characteristic aroma of cheese perceived with the swallowing |
| Burned oil flavor | Characteristic aroma of burned oil perceived with the swallowing |
| Taste and tactile in mouth | |
| Acid | Basic taste on tongue stimulated by acids |
| Fiber in the flesh | Amount of fibers in the sample after a bite |
| Mealiness | Gritty, sandy texture, dry not juicy |
| Bitter | Taste on the tongue stimulated by bitter compounds |
| Sweet | Taste on the tongue stimulated by sugars and high potency sweeteners |
| Rheological | |
| Juiciness | The amount of juice/moisture perceived in the mouth |
| Cultivar (Local and imported) | Weight (g) | SE | Firmness (N) | SE | TSS (Brix) | SE | TA (g L-1 citric acid) | SE | ||||||||
| Osteen GR local | 626 | ± | 7 | a | 28.19 | ± | 0.30 | c | 15.75 | ± | 0.59 | a | 0.58 | ± | 0.01 | b |
| Osteen GR LD1 | 556 | ± | 5 | b | 83.84 | ± | 0.16 | a | 8.90 | ± | 0.45 | b | 0.85 | ± | 0.08 | a |
| Osteen GR LD2 | 529 | ± | 4 | b | 74.04 | ± | 0.21 | b | 8.40 | ± | 0.52 | b | 0.79 | ± | 0.07 | a |
| Osteen MR local | 606 | ± | 8 | a | 10.04 | ± | 0.03 | b | 17.98 | ± | 0.42 | a | 0.26 | ± | 0.01 | b |
| Osteen MR LD1 | 506 | ± | 4 | b | 9.80 | ± | 0.05 | b | 11.50 | ± | 0.42 | b | 0.51 | ± | 0.05 | a |
| Osteen MR LD2 | 479 | ± | 4 | c | 15.20 | ± | 0.04 | a | 11.40 | ± | 0.39 | b | 0.45 | ± | 0.05 | a |
| Keitt GR local | 680 | ± | 5 | a | 33.83 | ± | 0.12 | c | 15.90 | ± | 0.29 | a | 0.54 | ± | 0.01 | b |
| Keitt GR LD1 | 573 | ± | 5 | b | 61.98 | ± | 0.13 | a | 9.45 | ± | 0.63 | b | 0.83 | ± | 0.08 | a |
| Keitt GR LD2 | 565 | ± | 6 | b | 56.14 | ± | 0.09 | b | 9.80 | ± | 0.54 | b | 0.86 | ± | 0.06 | a |
| Keitt MR local | 624 | ± | 6 | a | 13.72 | ± | 0.05 | a | 18.80 | ± | 0.26 | a | 0.41 | ± | 0.01 | a |
| Keitt MR LD1 | 554 | ± | 5 | b | 9.90 | ± | 0.04 | b | 11.23 | ± | 0.32 | c | 0.47 | ± | 0.02 | a |
| Keitt MR LD2 | 540 | ± | 5 | b | 4.12 | ± | 0.02 | c | 12.10 | ± | 0.44 | b | 0.32 | ± | 0.01 | b |
| Kent GR local | 686 | ± | 5 | a | 22.65 | ± | 0.08 | c | 14.05 | ± | 0.46 | a | 0.55 | ± | 0.02 | b |
| Kent GR LD1 | 593 | ± | 5 | b | 73.94 | ± | 0.07 | b | 9.20 | ± | 0.65 | b | 0.80 | ± | 0.07 | a |
| Kent GR LD2 | 614 | ± | 5 | c | 87.28 | ± | 0.09 | a | 8.50 | ± | 0.53 | b | 0.74 | ± | 0.08 | a |
| Kent MR local | 653 | ± | 5 | a | 11.77 | ± | 0.05 | a | 15.43 | ± | 0.41 | a | 0.58 | ± | 0.01 | c |
| Kent MR LD1 | 502 | ± | 5 | b | 7.84 | ± | 0.08 | c | 11.32 | ± | 0.65 | b | 0.69 | ± | 0.06 | b |
| Kent MR LD2 | 456 | ± | 5 | c | 9.81 | ± | 0.04 | b | 10.50 | ± | 0.58 | c | 0.85 | ± | 0.10 | a |
| * Values labelled with a different letter in the same column are significantly different for each ripening stage (Tukey's test at P ≤ 0.05). | ||||||||||||||||





