Non-tuberculous mycobacteria (NTM)-induced nodules following botulinum toxin injections are increasingly being reported. These infections can present as persistent nodules or abscesses, posing significant diagnostic and therapeutic challenges.
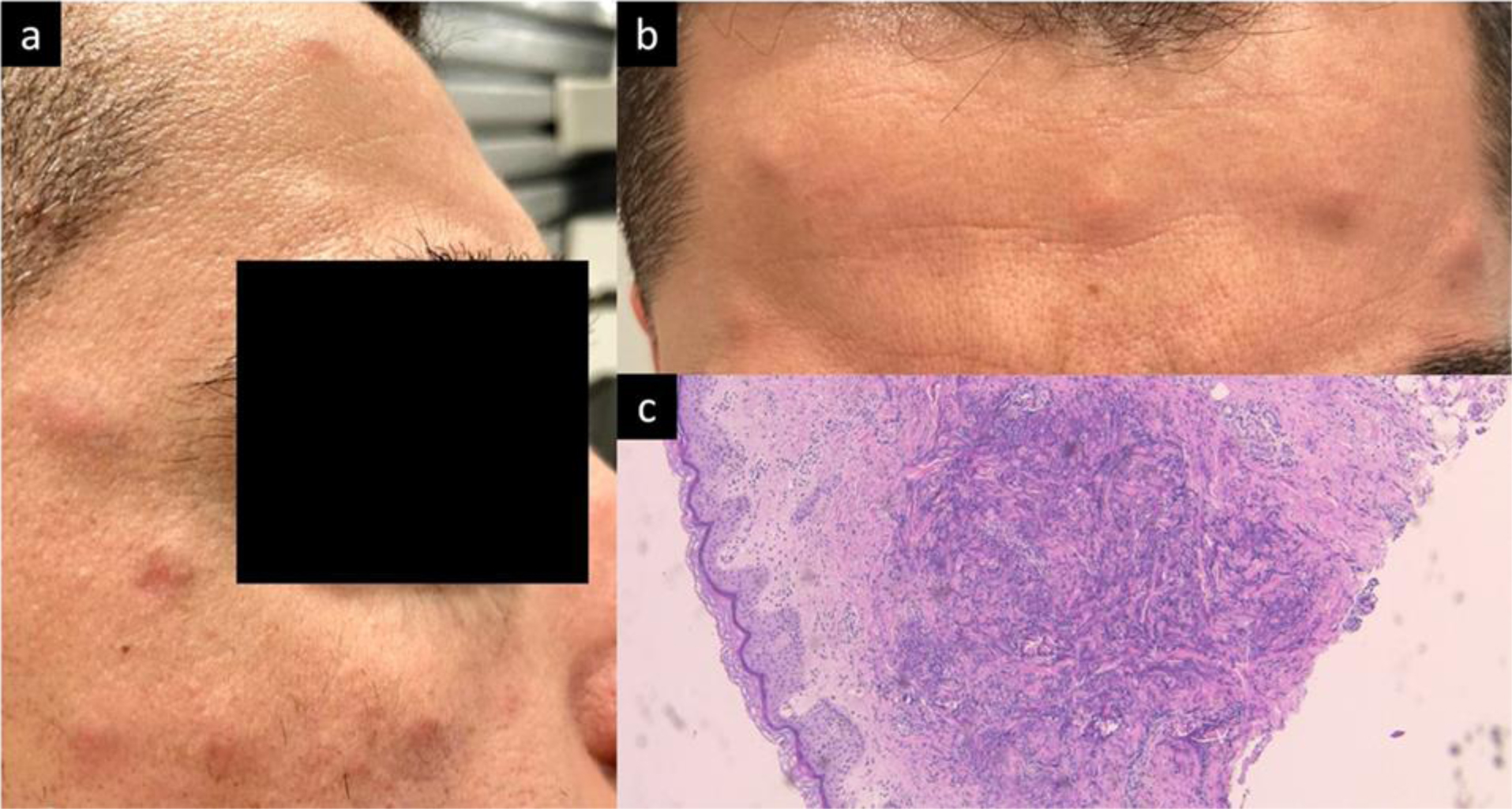
We report a case of a 35-year-old healthy male who developed multiple tender and painful nodules localized at injection sites on the forehead and periorbital areas three weeks after receiving Onabotulinum toxin injections from an untrusted provider. Initial treatment with oral steroids and empiric antibiotics was ineffective. Biopsy and NTM PCR confirmed the presence of Mycobacterium chelonae. The patient was successfully treated with a six-month regimen of oral clarithromycin, levofloxacin, and trimethoprim/sulfamethoxazole, resulting in complete remission without relapse at the eight-month follow-up.
A comprehensive review of the literature revealed eight reported cases of NTM-induced granulomatous nodules following botulinum toxin injections. These cases predominantly involved female patients and were associated with Mycobacterium abscessus, Mycobacterium immunogenum, and unidentified NTM species. This case is the first reported instance of Mycobacterium chelonae as an etiological agent in such a context. Effective management involves early biopsy, accurate microbiological diagnosis, and tailored antimicrobial therapy.
This case emphasizes the need for clinicians to consider NTM infections in patients with persistent nodules post-botulinum toxin injections, especially when initial treatments fail. To prevent such infections, it is crucial for patients to seek treatment from trusted and licensed providers who use authentic products and maintain sterile environments during procedures.
Citation: Joe Khodeir, Paul Ohanian, Ali Awwad. Mycobacterium chelonae-induced granulomatous nodules following botulinum toxin injections: A case report and literature review[J]. AIMS Allergy and Immunology, 2024, 8(4): 296-302. doi: 10.3934/Allergy.2024018
Non-tuberculous mycobacteria (NTM)-induced nodules following botulinum toxin injections are increasingly being reported. These infections can present as persistent nodules or abscesses, posing significant diagnostic and therapeutic challenges.
We report a case of a 35-year-old healthy male who developed multiple tender and painful nodules localized at injection sites on the forehead and periorbital areas three weeks after receiving Onabotulinum toxin injections from an untrusted provider. Initial treatment with oral steroids and empiric antibiotics was ineffective. Biopsy and NTM PCR confirmed the presence of Mycobacterium chelonae. The patient was successfully treated with a six-month regimen of oral clarithromycin, levofloxacin, and trimethoprim/sulfamethoxazole, resulting in complete remission without relapse at the eight-month follow-up.
A comprehensive review of the literature revealed eight reported cases of NTM-induced granulomatous nodules following botulinum toxin injections. These cases predominantly involved female patients and were associated with Mycobacterium abscessus, Mycobacterium immunogenum, and unidentified NTM species. This case is the first reported instance of Mycobacterium chelonae as an etiological agent in such a context. Effective management involves early biopsy, accurate microbiological diagnosis, and tailored antimicrobial therapy.
This case emphasizes the need for clinicians to consider NTM infections in patients with persistent nodules post-botulinum toxin injections, especially when initial treatments fail. To prevent such infections, it is crucial for patients to seek treatment from trusted and licensed providers who use authentic products and maintain sterile environments during procedures.

| [1] | Saeb-Lima M, Solis-Arreola GV, Fernandez-Flores A (2015) Mycobacterial infection after cosmetic procedure with botulinum toxin a. J Clin Diagn Res JCDR 9: WD01-WD02. https://doi.org/10.7860/JCDR/2015/11741.5756 |
| [2] | Chen X, Jin Y, Torres KMT, et al. (2019) Mycobacterium abscessus cutaneous infection secondary to botulinum toxin injection: A report of 2 cases. JAAD Case Rep 5: 982-984. https://doi.org/10.1016/j.jdcr.2019.09.017 |
| [3] | Deng L, Luo YZ, Liu F, et al. (2022) Subcutaneous infection caused by Mycobacterium abscessus following cosmetic injections of botulinum toxin: A case report. World J Clin Cases 10: 6141-6147. https://doi.org/10.12998/wjcc.v10.i18.6141 |
| [4] | Li C, Shen C, Zhang W (2024) Infectious granuloma with Mycobacterium abscessus after facial injection of botulinum toxin: A case report. J Craniofac Surg 35: e48-e50. https://doi.org/10.1097/SCS.0000000000009790 |
| [5] | Ou Y, Liu D, Feng J, et al. (2024) Subcutaneous infection caused by Mycobacterium abscessus following botulinum toxin injections: A case report and literature review. J Cosmet Dermatol 23: 1527-1532. https://doi.org/10.1111/jocd.16170 |
| [6] | Thanasarnaksorn W, Rattakul B, Suvanasuthi S, et al. (2019) Botulinum toxin type a injection-related suppurative granuloma: A case report. J Cosmet Laser Ther 21: 422-424. https://doi.org/10.1080/14764172.2019.1690663 |
| [7] | Yeon J, Chan RC, Fallah H (2021) Infection with Mycobacterium immunogenum following botulinum toxin injection. Australas J Dermatol 62: 79-80. https://doi.org/10.1111/ajd.13406 |
| [8] | Giavina-Bianchi P, Giavina-Bianchi M (2020) Granulomas induced by botulinum toxin. J Allergy Clin Immunol Pract 8: 1710-1711. https://doi.org/10.1016/j.jaip.2019.12.010 |
| [9] | Anabtawi M, Wege J, Mahmood H, et al. (2020) Nodular eruptions as a rare complication of botulinum neurotoxin type-A: Case series and review of literature. Cureus 12: e10175. https://doi.org/10.7759/cureus.10175 |
| [10] | Souza CL, Nascimento GG, Castellan CC, et al. (2023) Reactional nodule caused by the use of botulinum toxin and resulting in atrophic scars. in 32ND European Academy of Dermatology and Venereology (EADV) Congress 2023, Berlin, Germany . |
| [11] | Assmann T, Krahl D, Mang R (2013) Cutaneous sarcoidal granuloma after botulinum toxin type a injection. J Am Acad Dermatol 69: e247-e249. https://doi.org/10.1016/j.jaad.2013.04.060 |
| [12] | Herbert VG, Blödorn-Schlicht N, Böer-Auer A, et al. (2015) Cutaneous granulomatous reactions at botulinum neurotoxin A injection sites: First manifestation of systemic sarcoidosis. Hautarzt 66: 863-866. https://doi.org/10.1007/s00105-015-3651-8 |
| [13] | Ahbib S, Lachapelle JM, Marot L (2006) Granulomes sarcoïdosiques après injections de toxine botulique a (Botox®) pour correction de rides. Ann Dermatol Vénéréologie 133: 43-45. https://doi.org/10.1016/S0151-9638(06)70842-0 |
| [14] | Yun WJ, Kim JK, Kim BW, et al. (2013) The first documented case of true botulinum toxin granuloma. J Cosmet Laser Ther 15: 345-347. https://doi.org/10.3109/14764172.2013.795089 |
| [15] | George M (2023) Cutaneous non-tuberculous mycobacterial infections: An update. J Skin Sex Transm Dis 5: 90-97. https://doi.org/10.25259/JSSTD_52_2022 |
| [16] | Chirasuthat P, Triyangkulsri K, Rutnin S, et al. (2020) Cutaneous nontuberculous mycobacterial infection in Thailand: A 7-year retrospective review. Medicine (Baltimore) 99: e19355. https://doi.org/10.1097/MD.0000000000019355 |
| [17] | Li JJ, Beresford R, Fyfe J, et al. (2017) Clinical and histopathological features of cutaneous nontuberculous mycobacterial infection: A review of 13 cases. J Cutan Pathol 44: 433-443. https://doi.org/10.1111/cup.12903 |
Figures(1) / Tables(1)

Joe Khodeir, Paul Ohanian, Ali Awwad. Mycobacterium chelonae-induced granulomatous nodules following botulinum toxin injections: A case report and literature review[J]. AIMS Allergy and Immunology, 2024, 8(4): 296-302. doi: 10.3934/Allergy.2024018







 DownLoad:
DownLoad: