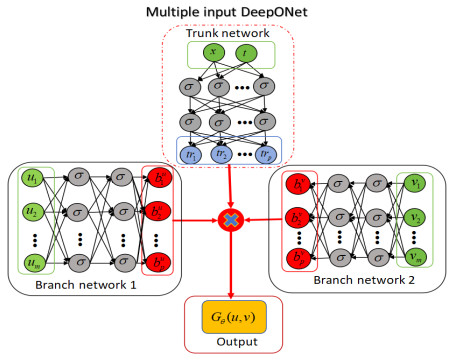
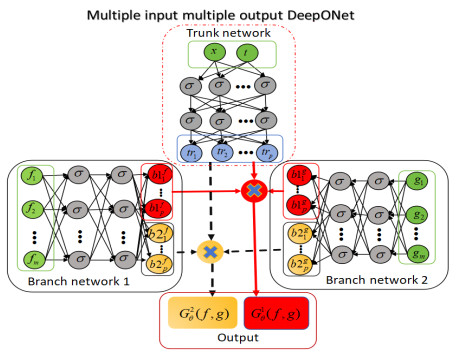
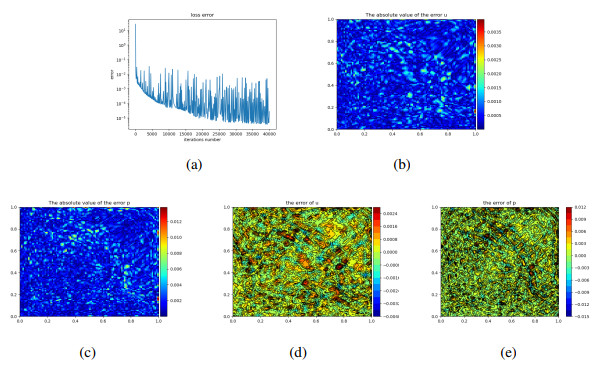
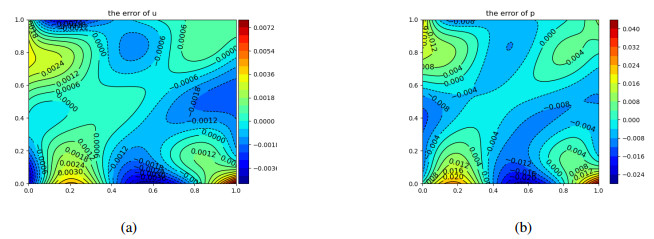
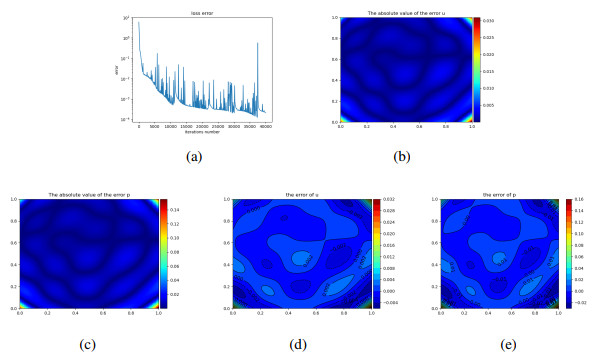
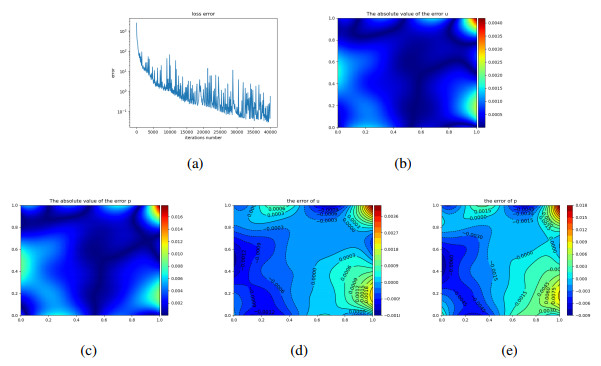
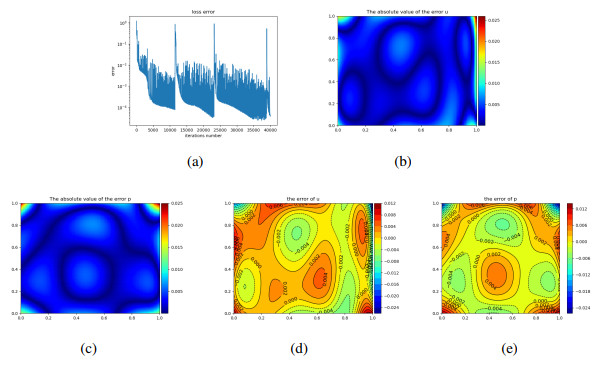
Deep operator networks is a popular machine learning approach. Some problems require multiple inputs and outputs. In this work, a multi-input and multi-output operator neural network (MIMOONet) for solving optimal control problems was proposed. To improve the accuracy of the numerical solution, a physics-informed MIMOONet was also proposed. To test the performance of the MIMOONet and the physics-informed MIMOONet, three examples, including elliptic (linear and semi-linear) and parabolic problems, were presented. The numerical results show that both methods are effective in solving these types of problems, and the physics-informed MIMOONet achieves higher accuracy due to its incorporation of physical laws.
Citation: Jinjun Yong, Xianbing Luo, Shuyu Sun. Deep multi-input and multi-output operator networks method for optimal control of PDEs[J]. Electronic Research Archive, 2024, 32(7): 4291-4320. doi: 10.3934/era.2024193
Deep operator networks is a popular machine learning approach. Some problems require multiple inputs and outputs. In this work, a multi-input and multi-output operator neural network (MIMOONet) for solving optimal control problems was proposed. To improve the accuracy of the numerical solution, a physics-informed MIMOONet was also proposed. To test the performance of the MIMOONet and the physics-informed MIMOONet, three examples, including elliptic (linear and semi-linear) and parabolic problems, were presented. The numerical results show that both methods are effective in solving these types of problems, and the physics-informed MIMOONet achieves higher accuracy due to its incorporation of physical laws.

| [1] |
G. Fabbri, Heat transfer optimization in corrugated wall channels, Int. J. Heat Mass Transfer, 43 (2000), 4299–4310. https://doi.org/10.1016/S0017-9310(00)00054-5 doi: 10.1016/S0017-9310(00)00054-5

|
| [2] | G. Cornuéjols, J. Peña, R. Tütüncü, Optimization Methods in Finance, 2$^{nd}$, Cambridge University Press, New York, 2018. |
| [3] |
J. C. De los Reyes, C. B. Schönlieb, Image denoising: learning the noise model via nonsmooth PDE-constrained optimization, Inverse Probl. Imaging, 7 (2013), 1183–1214. https://doi.org/10.3934/ipi.2013.7.1183 doi: 10.3934/ipi.2013.7.1183
|
| [4] | J. Sokolowski, J. P. Zolésio, Introduction to Shape Optimization, Springer-Verlag, Berlin, 1992. https://doi.org/10.1007/978-3-642-58106-9_1 |
| [5] | J. Haslinger, R. A. E. Mäkinen, Introduction to Shape Optimization: Theory, Approximation, and Computation, SIAM, Philadelphia, 2003. https://doi.org/10.1137/1.9780898718690 |
| [6] |
R. M. Hicks, P. A. Henne, Wing design by numerical optimization, J. Aircr., 15 (1978), 407–412. https://doi.org/10.2514/3.58379 doi: 10.2514/3.58379
|
| [7] |
P. D. Frank, G. R. Shubin, A comparison of optimization-based approaches for a model computational aerodynamics design problem, J. Comput. Phys., 98 (1992), 74–89. https://doi.org/10.1016/0021-9991(92)90174-W doi: 10.1016/0021-9991(92)90174-W
|
| [8] |
J. Ng, S. Dubljevic, Optimal boundary control of a diffusion-convection-reaction PDE model with time-dependent spatial domain: Czochralski crystal growth process, Chem. Eng. Sci., 67 (2012), 111–119. https://doi.org/10.1016/j.ces.2011.06.050 doi: 10.1016/j.ces.2011.06.050
|
| [9] | S. P. Chakrabarty, F. B. Hanson, Optimal control of drug delivery to brain tumors for a distributed parameters model, in Proceedings of the 2005, American Control Conference, 2 (2005), 973–978. https://doi.org/10.1109/ACC.2005.1470086 |
| [10] | W. B. Liu, N. N. Yan, Adaptive Finite Element Methods for Optimal Control Governed by PDEs, Science Press, Beijing, 2008. |
| [11] |
Y. P. Chen, F. L. Huang, N. Yi, W. B. Liu, A Legendre Galerkin spectral method for optimal control problems governed by Stokes equations, SIAM J. Numer. Anal., 49 (2011), 1625–1648. https://doi.org/10.1137/080726057 doi: 10.1137/080726057
|
| [12] | A. Borzì, V. Schulz, Computational Optimization of Systems Governed by Partial Differential Equations, SIAM, Philadelphia, 2011. |
| [13] |
X. Luo, A priori error estimates of Crank-Nicolson finite volume element method for a hyperbolic optimal control problem, Numer. Methods Partial Differ. Equations, 32 (2016), 1331–1356. https://doi.org/10.1002/num.22052 doi: 10.1002/num.22052
|
| [14] | M. Raissi, P. Perdikaris, G. E. Karniadakis, Physics informed deep learning (part Ⅰ): data-driven solutions of nonlinear partial differential equations, preprint, arXiv: 1711.10561. |
| [15] |
S. Wang, H. Zhang, X. Jiang, Physics-informed neural network algorithm for solving forward and inverse problems of variable-order space-fractional advection-diffusion equations, Neurocomputing, 535 (2023), 64–82. https://doi.org/10.1016/j.neucom.2023.03.032 doi: 10.1016/j.neucom.2023.03.032
|
| [16] |
J. Sirignano, K. Spiliopoulos, DGM: a deep learning algorithm for solving partial differential equations, J. Comput. Phys., 375 (2018), 1339–1364. https://doi.org/10.1016/j.jcp.2018.08.029 doi: 10.1016/j.jcp.2018.08.029
|
| [17] |
W. N. E, B. Yu, The deep Ritz method: a deep-learning based numerical algorithm for solving variational problems, Commun. Math. Stat., 6 (2018), 1–12. https://doi.org/10.1007/s40304-018-0127-z doi: 10.1007/s40304-018-0127-z
|
| [18] |
Y. L. Liao, P. B. Ming, Deep Nitsche method: deep Ritz method with essential boundary conditions, Commun. Comput. Phys., 29 (2021), 1365–1384. https://doi.org/10.4208/cicp.OA-2020-0219 doi: 10.4208/cicp.OA-2020-0219
|
| [19] |
L. Lu, P. Z. Jin, G. F. Pang, Z. Q. Zhang, G. E. Karniadakis, Learning nonlinear operators via DeepONet based on the universal approximation theorem of operators, Nat. Mach. Intell., 3 (2021), 218–229. https://doi.org/10.1038/s42256-021-00302-5 doi: 10.1038/s42256-021-00302-5
|
| [20] |
C. Moya, S. Zhang, G. Lin, M. Yue, DeepONet-grid-UQ: a trustworthy deep operator framework for predicting the power grid's post-fault trajectories, Neurocomputing, 535 (2023), 166–182. https://doi.org/10.1016/j.neucom.2023.03.015 doi: 10.1016/j.neucom.2023.03.015
|
| [21] | Z. Li, N. Kovachki, K. Azizzadenesheli, B. Liu, K. Bhattacharya, A. Stuart, et al., Neural operator: graph kernel network for partial differential equations, preprint, arXiv: 2003.03485. |
| [22] | Z. Li, N. Kovachki, K. Azizzadenesheli, B. Liu, K. Bhattacharya, A. Stuart, et al., Fourier neural operator for parametric partial differential equations, preprint, arXiv: 2010.08895. |
| [23] |
S. F. Wang, H. W. Wang, P. Perdikaris, Learning the solution operator of parametric partial differential equations with physics-informed DeepOnets, Sci. Adv., 7 (2021), eabi8605. https://doi.org/10.1126/sciadv.abi8605 doi: 10.1126/sciadv.abi8605
|
| [24] |
P. Jin, S. Meng, L. Lu, MIONet: learning multiple-input operators via tensor product, SIAM J. Sci. Comput., 44 (2022), A3490–A3514. https://doi.org/10.1137/22M1477751 doi: 10.1137/22M1477751
|
| [25] |
C. J. García-Cervera, M. Kessler, F. Periago, Control of partial differential equations via physics-informed neural networks, J. Optim. Theory Appl., 196 (2023), 391–414. https://doi.org/10.1007/s10957-022-02100-4 doi: 10.1007/s10957-022-02100-4
|
| [26] |
S. Mowlavi, S. Nabib, Optimal control of PDEs using physics-informed neural networks, J. Comput. Phys., 473 (2023), 111731. https://doi.org/10.1016/j.jcp.2022.111731 doi: 10.1016/j.jcp.2022.111731
|
| [27] | J. Barry-Straume, A. Sarsha, A. A. Popov, A. Sandu, Physics-informed neural networks for PDE-constrained optimization and control, preprint, arXiv: 2205.03377. |
| [28] | S. F. Wang, M. A. Bhouri, P. Perdikaris, Fast PDE-constrained optimization via self-supervised operator learning, preprint, arXiv: 2110.13297. |
| [29] | J.L. Lions, Optimal Control of Systems Governed by Partial Differential Equations, Springer-Verlag, Berlin, 1971. |
| [30] |
T. P. Chen, H. Chen, Universal approximation to nonlinear operators by neural networks with arbitrary activation functions and its application to dynamical systems, IEEE Trans. Neural Networks, 6 (1995), 911–917. https://doi.org/10.1109/72.392253 doi: 10.1109/72.392253
|
| [31] | I. Lasiecka, Mathematical Control Theory of Coupled PDEs, SIAM, Philadelphia, 2001. https://doi.org/10.1137/1.9780898717099 |
| [32] | A. Miranville, The Cahn-Hilliard Equation: Recent Advances and Applications, SIAM, Philadelphia, 2019. https://doi.org/10.1137/1.9781611975925 |

Figures(25) / Tables(8)
Jinjun Yong, Xianbing Luo, Shuyu Sun. Deep multi-input and multi-output operator networks method for optimal control of PDEs[J]. Electronic Research Archive, 2024, 32(7): 4291-4320. doi: 10.3934/era.2024193







 DownLoad:
DownLoad: