Citation: Lynda M. Hegarty, Jacqueline L. Mair, Karen Kirby, Elaine Murtagh, Marie H. Murphy. School-based Interventions to Reduce Sedentary Behaviour in Children: A Systematic Review[J]. AIMS Public Health, 2016, 3(3): 520-541. doi: 10.3934/publichealth.2016.3.520

| [1] | Sedentary Behaviour Research Network. What is sedentary behavior? 28 October 2014. Available from: http://www.sedentarybehaviour.org/what-is-sedentary-behaviour/. |
| [2] | Biddle SJ, Gorely T and Stensel DJ (2004) Health-enhancing physical activity and sedentary behaviour in children and adolescents. J Sports Sci 22(8): 679-701. |
| [3] | Cale L and Harris J (2013) “Every child (of every size) matters” in physical education! Physical education’s role in childhood obesity. Sport Educ Soc 18(4): 433-452. |
| [4] | Healy GN, Clark BK, Winkler EA, et al. (2011) Measurement of adults' sedentary time in population-based studies. Am J Prev Med 41(2): 216-227. |
| [5] | Brug J and Chinapaw M (2015) Determinants of engaging in sedentary behavior across the lifespan; lessons learned from two systematic reviews conducted within DEDIPAC. Int J Behav Nutr Phys Act 12(1): 134. |
| [6] | Prentice-Dunn H and Prentice-Dunn S (2012) Physical activity, sedentary behavior, and childhood obesity: a review of cross-sectional studies. Psychol Health Med 17(3): 255-273. |
| [7] | Katzmarzyk PT, Barreira TV, Broyles ST, et al. (2015) Physical activity, sedentary time, and obesity in an international sample of children. Med Sci Sports Exercise 47(10): 2062-9. |
| [8] | Tremblay MS, LeBlanc AG, Kho ME, et al. (2011) Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act 8(1): 98. |
| [9] | Basterfield L, Adamson AJ, Frary JK, et al. (2011) Longitudinal study of physical activity and sedentary behavior in children. Pediatrics 127(1): e24-e30. |
| [10] |
Verloigne M, Bere E, Van Lippevelde W, et al. (2012) The effect of the UP4FUN pilot intervention on objectively measured sedentary time and physical activity in 10–12 year old children in Belgium: the ENERGY-project. BMC Public Health 12: 805. doi: 10.1186/1471-2458-12-805

|
| [11] | Biddle SJ, Pearson N, Ross GM et al. (2010) Tracking of sedentary behaviours of young people: a systematic review. Prev Med 51(5): 345-351. |
| [12] | Jones RA, Hinkley T, Okely AD, et al. (2013) Tracking Physical Activity and Sedentary Behavior in Childhood: A Systematic Review. Am J Prev Med 44(6): 651-658. |
| [13] | Colley RC, Garriguet D, Janssen I, et al. (2011) Physical activity of Canadian children and youth: accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep 22(1): 15. |
| [14] | Saunders TJ, Chaput JP and Tremblay MS (2014) Sedentary behaviour as an emerging risk factor for cardiometabolic diseases in children and youth. Can J Diabetes 38(1): 53-61. |
| [15] |
Sandercock GR, Alibrahim M and Bellamy M (2016) Media device ownership and media use: Associations with sedentary time, physical activity and fitness in English youth. Prev Med Rep 4: 162-168. doi: 10.1016/j.pmedr.2016.05.013
|
| [16] | Bradley RH, McRitchie S, Houts RM, et al. (2011) Parenting and the decline of physical activity from age 9 to 15. Int J Behav Nutr Phys Act 8(1): 33. |
| [17] | Chu AHY, Ng SHX, Tan CS, et al. (2016) A systematic review and meta‐analysis of workplace intervention strategies to reduce sedentary time in white‐collar workers. Obesity Rev 17(5): 467-481. |
| [18] | Yıldırım M, Verloigne M, De Bourdeaudhuij I (2011) Study protocol of physical activity and sedentary behaviour measurement among schoolchildren by accelerometry-Cross-sectional survey as part of the ENERGY-project. BMC Public Health 11(1): 182. |
| [19] | Rush E, Coppinger T, Obolonkin V, et al. (2012) Use of pedometers to identify less active children and time spent in moderate to vigorous physical activity in the school setting. J Sci Med Sport 15(3): 226-230. |
| [20] | van Stralen MM, Yıldırım M, Wulp A, et al. (2014) Measured sedentary time and physical activity during the school day of European 10-to 12-year-old children: The ENERGY project. J Sci Med Sport 17(2): 201-206. |
| [21] | Kastorini CM, Lykou A, Yannakoulia M, et al. (2016) The influence of a school-based intervention programme regarding adherence to a healthy diet in children and adolescents from disadvantaged areas in Greece: the DIATROFI study. J Epidemiol Community Health, doi:10.1136/jech-2015-205680. |
| [22] |
Vander Ploeg KA, Maximova K, McGavock J, et al. (2014) Do school-based physical activity interventions increase or reduce inequalities in health? Soc Sci Med 112: 80-87. doi: 10.1016/j.socscimed.2014.04.032
|
| [23] | Nyberg G, Norman Å, Sundblom E, et al. (2016) Effectiveness of a universal parental support programme to promote health behaviours and prevent overweight and obesity in 6-year-old children in disadvantaged areas, the Healthy School Start Study II, a cluster-randomised controlled trial. Int J Behav Nutr Phys Act 13(1): 4. |
| [24] | van Grieken A, Ezendam NP, Paulis WD, et al. (2012) Primary prevention of overweight in children and adolescents: a meta-analysis of the effectiveness of interventions aiming to decrease sedentary behaviour. Int J Behav Nutr Phys Act 9 (1): 1-11. |
| [25] | Grant PM, Ryan CG, Tigbe WW, et al. (2006) The validation of a novel activity monitor in the measurement of posture and motion during everyday activities. Br J Sports Med 40(12): 992-997. |
| [26] | Reilly JJ, Penpraze V, Hislop J, et al. (2008) Objective measurement of physical activity and sedentary behaviour: review with new data. Arch Dis Child 93(7): 614-619. |
| [27] | Yang CC and Hsu YL (2010) A review of accelerometry-based wearable motion detectors for physical activity monitoring. Sensors 10(8): 7772-7788. |
| [28] | Hardy LL, Hills AP, Timperio A, et al. (2013) A hitchhiker's guide to assessing sedentary behaviour among young people: Deciding what method to use. J Sci Med Sport 16(1): 28-35. |
| [29] |
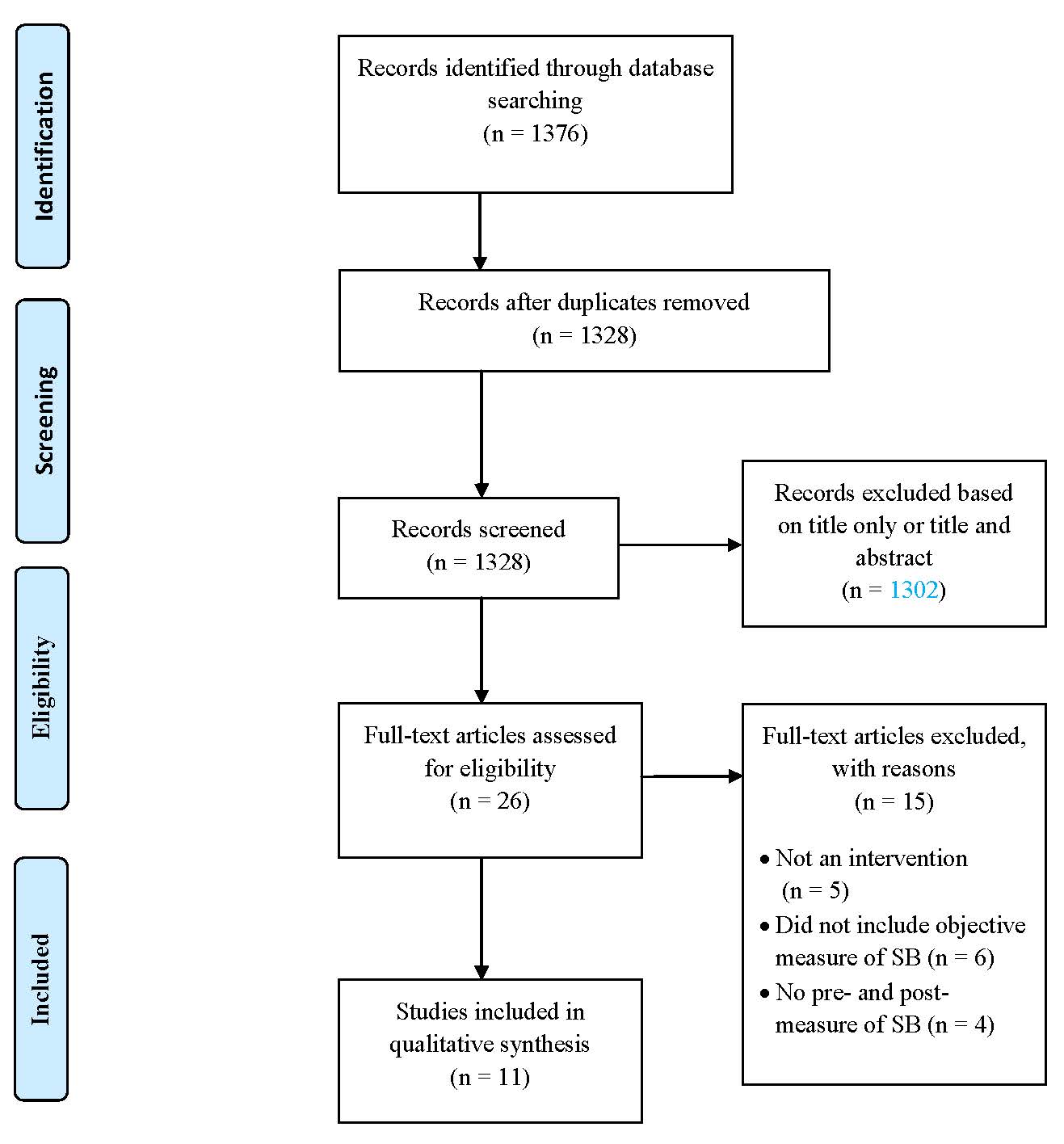
Moher D, Liberati A, Tetzlaff J, et al. (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339: b2535. doi: 10.1136/bmj.b2535
|
| [30] |
Higgins JP, Altman DG, Gøtzsche PC, et al. (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343: d5928. doi: 10.1136/bmj.d5928
|
| [31] | PROSPERO International prospective register of systematic reviews. CRD, 42015025724, Available from: http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015025724. |
| [32] | Breslin G, Brennan D, Rafferty R, et al. (2012) The effect of a healthy lifestyle programme on 8–9 year olds from social disadvantage. Arch Dis Child 97(7): 618-624. |
| [33] |
Fairclough SJ, Hackett AF, Davies IG, et al. (2013) Promoting healthy weight in primary school children through physical activity and nutrition education: a pragmatic evaluation of the CHANGE! Randomised intervention study. BMC Public Health 13: 626. doi: 10.1186/1471-2458-13-626
|
| [34] |
Kipping RR, Howe LD, Jago R, et al. (2014) Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: active for Life Year 5 (AFLY5) school based cluster randomised controlled trial. BMJ 348: g3256. doi: 10.1136/bmj.g3256
|
| [35] |
Carson V, Salmon J, Arundell L, et al. (2013) Examination of mid-intervention mediating effects on objectively assessed sedentary time among children in the Transform-Us! cluster-randomized controlled trial. Int J Behav Nutr Phys Act 10: 62. doi: 10.1186/1479-5868-10-62
|
| [36] | Yildirim M, Arundell L, Cerin E, et al. (2014) What helps children to move more at school recess and lunchtime? Mid-intervention results from Transform-Us! cluster-randomised controlled trial. Br J Sports Med 48(3): 271-277. |
| [37] | Aminian S and Hinckson EA (2012) Examining the validity of the ActivPAL monitor in measuring posture and ambulatory movement in children. International J Behav Nutr Phys Act 9(1): 119. |
| [38] | Hinckson EA, Aminian S, Ikeda E, et al. (2013) Acceptability of standing workstations in elementary schools: a pilot study. Prev Med 56(1): 82-85. |
| [39] |
Verloigne M, Bere E, Van Lippevelde W, et al. (2012) The effect of the UP4FUN pilot intervention on objectively measured sedentary time and physical activity in 10–12 year old children in Belgium: the ENERGY-project. BMC Public Health 12: 805. doi: 10.1186/1471-2458-12-805
|
| [40] | Verloigne M, Ridgers ND, Chinapaw M, et al. (2015) The UP4FUN Intervention Effect on Breaking Up Sedentary Time in 10-to 12-Year-Old Belgian Children: The ENERGY Project. Pediatr Exerc Sci 27(2). |
| [41] | Vik FN, Lien N, Berntsen S, et al. (2015) Evaluation of the UP4FUN intervention: a cluster randomized trial to reduce and break up sitting time in European 10–12-year-old children. PloS One 10(3): p.e0122612. |
| [42] | Clemes SA, Barber SE, Bingham DD, et al. (2015) Reducing children's classroom sitting time using sit-to-stand desks: findings from pilot studies in UK and Australian primary schools. J Public Health p.fdv084. |
| [43] | Bandura A (1986) Social Foundations of Thought and Action: A Social Cognitive Theory. New Jersey: Prentice Hall. |
| [44] | Lawlor DA. AFLY5 Study [Internet]. Message to: Lynda Hegarty. 2016 Feb 10 [cited 2016 Feb 29]. [1 paragraph]. |
| [45] | Russ LB, Webster CA, Beets MW, et al. (2015) Systematic Review and Meta-Analysis of Multi-Component Interventions Through Schools to Increase Physical Activity. J Phys Act Health 12(10). |
| [46] | Shirley K, Rutfield R, Hall N, et al. (2015) Combinations of obesity prevention strategies in US elementary schools: a critical review. J Prim Prev 36(1): 1-20. |
| [47] | Amini M, Djazayery A, Majdzadeh R, et al (2015) Effect of school-based interventions to control childhood obesity: a review of reviews. Int J Prev Med 6, doi:10.4103/2008-7802.162059 |
| [48] | Biddle SJ, O'Connell S and Braithwaite RE (2011) Sedentary behaviour interventions in young people: a meta-analysis. Br J Sports Med 45(11): 937-942. |
| [49] | Chastin SF, Egerton T, Leask C, et al. (2015) Meta‐analysis of the relationship between breaks in sedentary behavior and cardiometabolic health. Obesity 23(9): 1800-1810. |
| [50] | Machin D, Campbell MJ, Tan SB et al. (2011) Sample size tables for clinical studies. John Wiley & Sons. |
| [51] | Button KS, Ioannidis JP, Mokrysz C, et al. (2013) Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci 14(5): 365-376. |
| [52] | JanssenX, Basterfield L, Parkinson KN, et al. (2015) Objective measurement of sedentary behavior: impact of non-wear time rules on changes in sedentary time. BMC Public Health 15(1): 1. |
| [53] | Carr LJ and Mahar MT (2012) Accuracy of intensity and inclinometer output of three activity monitors for identification of sedentary behavior and light-intensity activity. J Obes, doi:10.1155/2012/460271. |
| [54] | Breslin G and Brennan D (2012) A healthy lifestyle intervention delivered by aspiring physical education teachers to children from social disadvantage: study protocol and preliminary findings. Child Care Pract 18(3): 207-225. |
| [55] | Koepp GA, Snedden BJ, Flynn L, et al. (2012) Feasibility analysis of standing desks for sixth graders. ICAN Infant Child Adolesc Nutr 4(2): 89-92. |
| [56] | British Heart Foundation. Sedentary behaviour, 2012. Available from: http://www.bhf.org.uk/thinkfit/default.aspx?page=1304 (Accessed 22 May 2013). |
| [57] | World Health Organization. Health education: theoretical concepts, effective strategies and core competencies. 2012. Available from: http://applications.emro.who.int/dsaf/EMRPUB_2012_EN_1362.pdf (Accessed 26 October 2014). |
| [58] | Bronfenbrenner U (1994) Ecological models of human development. Read Dev Child 2: 37-43. |
| [59] | Sallis J, Owen N. Ecological Models of Health Behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health behavior: Theory, research, and practice. San Francisco, CA: Jossey-Bass; 2015. p. 43-64. |
| [60] | Waters E, de Silva-Sanigorski A, Hall BJ, et al. (2011) Interventions for preventing obesity in children. Cochrane Database Syst Rev 132(12): 428-432. |
| [61] | Shrestha N, Kukkonen‐Harjula KT, Verbeek JH, et al. (2016) Workplace interventions for reducing sitting at work. Cochrane Database of Systematic Reviews 2016, Issue 3. Art. No.: CD010912. DOI: 10.1002/14651858.CD010912.pub3. |
| [62] | LeBlanc AG, Broyles ST, Chaput JP, et al. (2015) Correlates of objectively measured sedentary time and self-reported screen time in Canadian children. Int J Behav Nutr Phys Act 12(1): 1. |
Figures(1) / Tables(4)

Lynda M. Hegarty, Jacqueline L. Mair, Karen Kirby, Elaine Murtagh, Marie H. Murphy. School-based Interventions to Reduce Sedentary Behaviour in Children: A Systematic Review[J]. AIMS Public Health, 2016, 3(3): 520-541. doi: 10.3934/publichealth.2016.3.520







 DownLoad:
DownLoad: