Abdominal pregnancy is very rare, with only a few gynecologists being fortunate to encounter it all through their professional careers. It makes up only 1% of all ectopic pregnancies but has very high perinatal and maternal mortality of 95% and 18% respectively. Hemorrhagic and infectious complications account for these. Removal of the placenta at laparotomy is a big dilemma as torrential bleeding may ensue.
We report the case of an undergraduate teenager who was referred with features of septicemia and anemia following unsafe vaginal instrumentation by a patent medicine dealer (a person without formal training in pharmacy but sells orthodox medications on retail basis) in a bid to terminate an extrauterine pregnancy. Ultrasonography confirmed a nonviable abdominal pregnancy of 20 weeks.
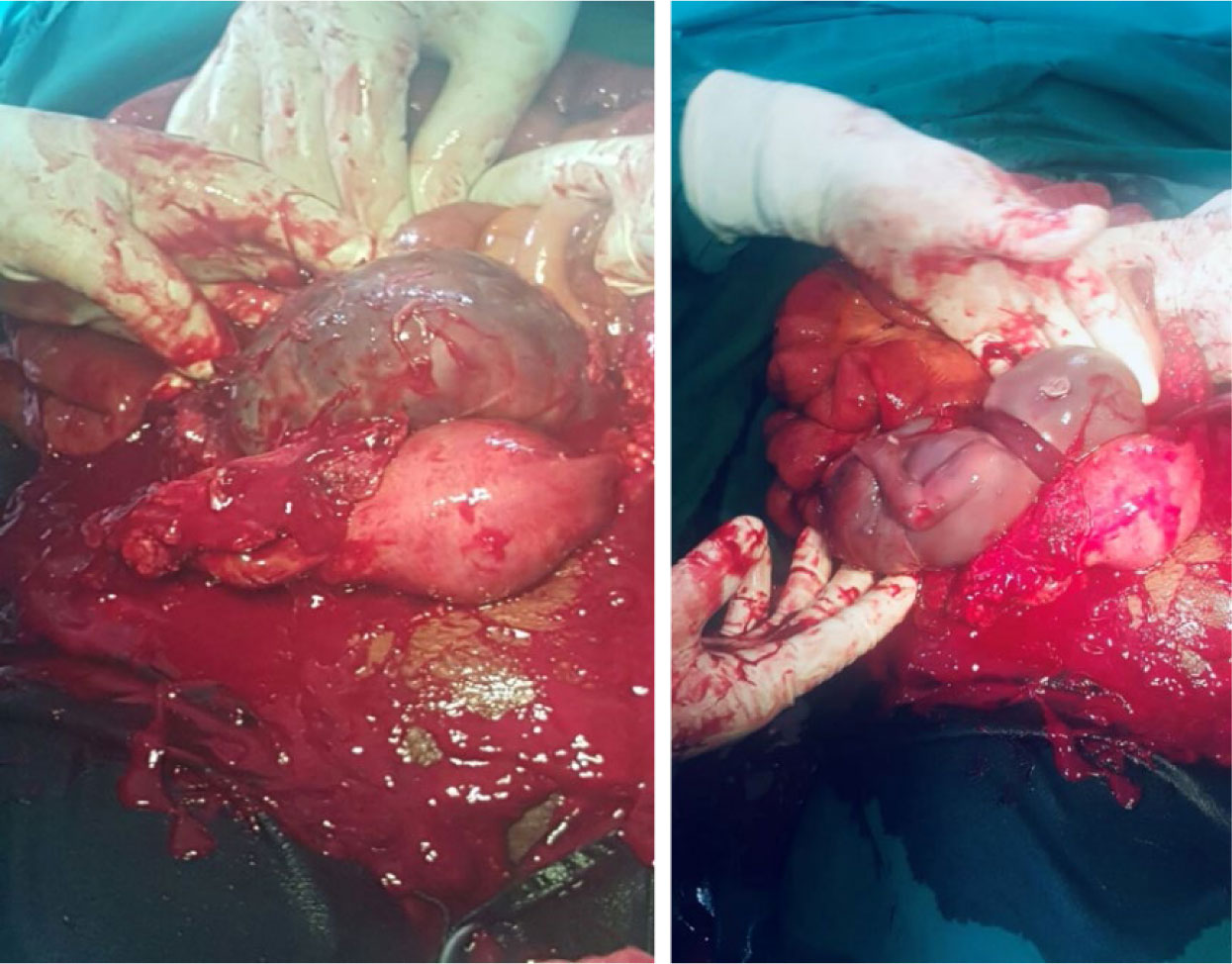
She had exploratory laparotomy with the evacuation of the dead fetus and successful complete removal of the placenta. Her postoperative recovery was uneventful.
In view of the grave complications like a pelvic abscess, disseminated intravascular coagulation and bowel obstruction that may accompany retention of the placenta in advanced abdominal pregnancy, optimal placental removal at surgery is recommended whenever feasible.
Citation: Victor Okey Dinwoke, Michael Oluchukwu Amara, Linda Uzo Amara. Abdominal pregnancy—a diagnosis never to miss[J]. AIMS Medical Science, 2022, 9(2): 342-347. doi: 10.3934/medsci.2022015
Abdominal pregnancy is very rare, with only a few gynecologists being fortunate to encounter it all through their professional careers. It makes up only 1% of all ectopic pregnancies but has very high perinatal and maternal mortality of 95% and 18% respectively. Hemorrhagic and infectious complications account for these. Removal of the placenta at laparotomy is a big dilemma as torrential bleeding may ensue.
We report the case of an undergraduate teenager who was referred with features of septicemia and anemia following unsafe vaginal instrumentation by a patent medicine dealer (a person without formal training in pharmacy but sells orthodox medications on retail basis) in a bid to terminate an extrauterine pregnancy. Ultrasonography confirmed a nonviable abdominal pregnancy of 20 weeks.
She had exploratory laparotomy with the evacuation of the dead fetus and successful complete removal of the placenta. Her postoperative recovery was uneventful.
In view of the grave complications like a pelvic abscess, disseminated intravascular coagulation and bowel obstruction that may accompany retention of the placenta in advanced abdominal pregnancy, optimal placental removal at surgery is recommended whenever feasible.

| [1] |
Dahiya K, Sharma D (2007) Advanced abdominal pregnancy: a diagnostic and management dilemma. J Gynecol Surg 23: 69-72. https://doi.org/10.1089/gyn.2007.B-02259-1 
|
| [2] |
Jurkovic D (2012) Ectopic pregnancy. Dewhurst's Textbook of Obstetrics and Gynaecology for Postgraduates . Wiley-Blackwell 76-86. https://doi.org/10.1002/9781119979449.ch9
|
| [3] | Delke I, Veridiano NP, Tancer ML (1982) Abdominal pregnancy: review of current management and addition of 10 cases. Obstet Gynecol 60: 200-204. |
| [4] |
Mengistu Z, Getachew A, Adefris M (2015) Term abdominal pregnancy: a case report. J Med Case Rep 9: 168. https://doi.org/10.1186/s13256-015-0635-3
|
| [5] | Huang K, Song L, Wang L, et al. (2014) Advanced abdominal pregnancy: an increasingly challenging clinical concern for obstetricians. Int J Clin Exp Pathol 7: 5461-5472. |
| [6] | Kwawukume EY, Ekele BA, Idrisa A (2015) Ectopic pregnancy. Comprehensive Obstetrics in the Tropics 282-286. |
| [7] | Glob Libr Women's Med, Stubblefield P, Averbach S, Septic Abortion: Prevention and Management, 2014. Available from: https://doi.org/10.3843/GLOWM.10438 |
| [8] |
Mahbuba M, Fatema K, Saha RK (2013) Advanced abdominal pregnancy with a full-term live fetus: case report. Faridpur Med College J 8: 40-43. https://doi.org/10.3329/fmcj.v8i1.16898
|
| [9] |
Hallatt JG, Grove JA (1985) Abdominal pregnancy: A study of twenty-one consecutive cases. Am J Obstet Gynecol 152: 444-449. https://doi.org/10.1016/S0002-9378(85)80155-1
|
| [10] |
Rahaman J, Berkowitz R, Mitty H, et al. (2004) Minimally invasive management of an advanced abdominal pregnancy. Obstet Gynecol 103: 1064-1068. https://doi.org/10.1097/01.AOG.0000127946.14387.48
|
| [11] |
Kunwar S, Khan T, Srivastava K (2015) Abdominal pregnancy: Methods of hemorrhage control. Intractable Rare Dis Res 4: 105-107. https://doi.org/10.5582/irdr.2015.01006
|
| [12] |
Singh A, Mishra V, Arum D, et al. (2014) Management dilemma in case of abdominal pregnancy: a case report. Open J Obstet Gynaecol 4: 899-902. https://doi.org/10.4236/ojog.2014.414126
|
| [13] | Rahman MS, Al-Suleiman SA, Rahman J, et al. (1982) Advanced abdominal pregnancy—observations in 10 cases. Obstet Gynecol 59: 366-372. |

Figures(2)

Victor Okey Dinwoke, Michael Oluchukwu Amara, Linda Uzo Amara. Abdominal pregnancy—a diagnosis never to miss[J]. AIMS Medical Science, 2022, 9(2): 342-347. doi: 10.3934/medsci.2022015







 DownLoad:
DownLoad: