Onodi cells (OC) are important for rhinologists because they contain the optic canal, and are close to the optic nerve and internal carotid artery. Therefore, any pathologic processes within OCs, including infectious or inflammatory sinusitis, fungus ball, inverted papilloma, mucocele, or sino-nasal malignancy can cause devastating ophthalmologic complications. We aimed to define the different optic neuropathy conditions related to isolated OC mucoceles, determine the different symptoms of each condition and its risk factors, and explore the efficacy of the relevant diagnostic tools and treatment strategies.
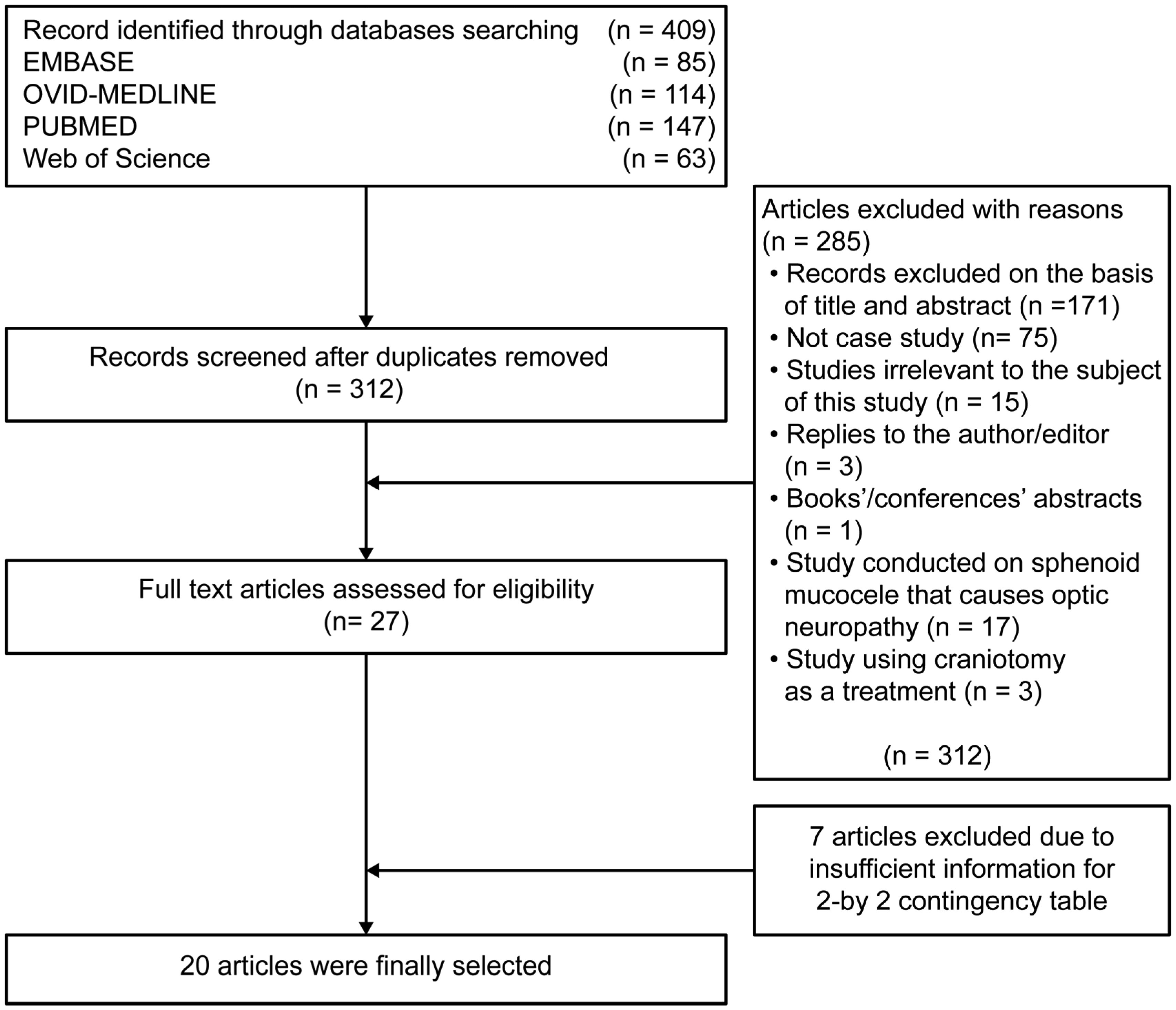
A comprehensive electronic search with time and language restrictions was conducted. Several known databases were included: PubMed, The Cochrane Library, and Web of Science from 1990 to 2020. We combined the search terms and limited the study to the English language. We removed duplicates, and the articles were screened based on title, abstract, and full text according to the PRISMA checklist.
The electronic search strategy conducted in this review resulted in 409 hits. After removing duplicate studies and studies with inadequate information, 20 case studies were finally included in this analysis, 65% of which presented men (n = 13), and seven presented women (35%). The mean age reported in these studies was 54.75 with a standard deviation of 14.62 years. We found that visual disturbances that can lead to visual loss were present in most cases (75% of cases). Other symptoms included headache (35%) and eye pain (30%). The risk factors for developing optic neuropathy conditions related to OC mucoceles include being Asian and elderly with a history of either nasal or eye conditions. Our findings showed that the mean time between the onset of symptoms and intervention was 16.8 ± 21.8 days. Most patients underwent endoscopic sinus surgery to remove the OC mucocele (18/20; 90%) with a success rate of 77%. Pharmacologic intervention as a solo treatment (IV corticosteroids or /and antibiotic) was used in only six patients, with a success rate of only 33%. Computed tomography (CT) and magnetic resonance imaging (MRI) is the most commonly used diagnostic tools, with diagnostic success rates of 40% and 82.3%, respectively.
Optic neuropathy conditions related to OC mucoceles are very rare. However, a higher incidence of these conditions was observed in elderly Asian patients with a history of nasal or optic conditions. Visual disturbances are the most common symptoms accompanying any type of eye condition. Endoscopic sinus surgery is considered an effective and safe intervention for these patients, and the period between the onset of symptoms and surgery does not affect the outcomes of the surgery. Furthermore, treatment with corticosteroids and/or antibiotics cannot replace surgery and it can also worsen the condition. Moreover, MRI is superior to CT scans for demonstrating this abnormality, and both are superior to other diagnostic tools. Finally, further investigations should be conducted to study the causes of the low incidence of these conditions in the eastern region.
Citation: Turki M. Bin Mahfoz, Ahmad K. Alnemare. Optic neuropathy related to Onodi cell mucocele: a systematic review and meta-analysis of randomized controlled trials[J]. AIMS Medical Science, 2021, 8(3): 203-223. doi: 10.3934/medsci.2021018
Onodi cells (OC) are important for rhinologists because they contain the optic canal, and are close to the optic nerve and internal carotid artery. Therefore, any pathologic processes within OCs, including infectious or inflammatory sinusitis, fungus ball, inverted papilloma, mucocele, or sino-nasal malignancy can cause devastating ophthalmologic complications. We aimed to define the different optic neuropathy conditions related to isolated OC mucoceles, determine the different symptoms of each condition and its risk factors, and explore the efficacy of the relevant diagnostic tools and treatment strategies.
A comprehensive electronic search with time and language restrictions was conducted. Several known databases were included: PubMed, The Cochrane Library, and Web of Science from 1990 to 2020. We combined the search terms and limited the study to the English language. We removed duplicates, and the articles were screened based on title, abstract, and full text according to the PRISMA checklist.
The electronic search strategy conducted in this review resulted in 409 hits. After removing duplicate studies and studies with inadequate information, 20 case studies were finally included in this analysis, 65% of which presented men (n = 13), and seven presented women (35%). The mean age reported in these studies was 54.75 with a standard deviation of 14.62 years. We found that visual disturbances that can lead to visual loss were present in most cases (75% of cases). Other symptoms included headache (35%) and eye pain (30%). The risk factors for developing optic neuropathy conditions related to OC mucoceles include being Asian and elderly with a history of either nasal or eye conditions. Our findings showed that the mean time between the onset of symptoms and intervention was 16.8 ± 21.8 days. Most patients underwent endoscopic sinus surgery to remove the OC mucocele (18/20; 90%) with a success rate of 77%. Pharmacologic intervention as a solo treatment (IV corticosteroids or /and antibiotic) was used in only six patients, with a success rate of only 33%. Computed tomography (CT) and magnetic resonance imaging (MRI) is the most commonly used diagnostic tools, with diagnostic success rates of 40% and 82.3%, respectively.
Optic neuropathy conditions related to OC mucoceles are very rare. However, a higher incidence of these conditions was observed in elderly Asian patients with a history of nasal or optic conditions. Visual disturbances are the most common symptoms accompanying any type of eye condition. Endoscopic sinus surgery is considered an effective and safe intervention for these patients, and the period between the onset of symptoms and surgery does not affect the outcomes of the surgery. Furthermore, treatment with corticosteroids and/or antibiotics cannot replace surgery and it can also worsen the condition. Moreover, MRI is superior to CT scans for demonstrating this abnormality, and both are superior to other diagnostic tools. Finally, further investigations should be conducted to study the causes of the low incidence of these conditions in the eastern region.

| [1] |
Ónodi A (1904) III. Die Sehstörungen und Erblindung nasalen Ursprunges, bedingt durch Erkrankungen der hinteren Nebenhöhlen. Ophthalmologica 12: 23-46. doi: 10.1159/000290212

|
| [2] |
Kitagawa K, Hayasaka S, Shimizu K, et al. (2003) Optic neuropathy produced by a compressed mucocele in an Onodi cell. Am J Ophthalmol 135: 253-254. doi: 10.1016/S0002-9394(02)01941-4
|
| [3] | Kennedy D, Bolger W, Zinreich S Diseases of the sinuses: diagnosis and management (2001) . |
| [4] |
Fukuda Y, Chikamatsu K, Ninomiya H, et al. (2006) Mucocele in an Onodi cell with simultaneous bilateral visual disturbance. Auris Nasus Larynx 33: 199-202. doi: 10.1016/j.anl.2005.11.024
|
| [5] |
Nonaka M, Fukumoto A, Nonaka R, et al. (2007) A case of a mucocele in an Onodi cell. J Nippon Med Sch 74: 325-328. doi: 10.1272/jnms.74.325
|
| [6] | Lim SA, Sitoh YY, Lim TC, et al. (2008) Clinics in diagnostic imaging (120). Right rhinogenic optic neuritis secondary to mucocoele of the Onodi cell. Singapore Med J 49: 84-87. |
| [7] |
Moeller CW, Welch KC (2010) Prevention and management of complications in sphenoidotomy. Otolaryngol Clin North Am 43: 839-854. doi: 10.1016/j.otc.2010.04.009
|
| [8] |
Yoon KC, Park YG, Kim HD, et al. (2006) Optic neuropathy caused by a mucocele in an Onodi cell. Jpn J Ophthalmol 50: 296-298. doi: 10.1007/s10384-005-0299-4
|
| [9] |
Yamaguchi K, Ohnuma I, Takahashi S, et al. (1997) Magnetic resonance imaging in acute optic neuropathy by sphenoidal mucocele. Int Ophthalmol 21: 9-11. doi: 10.1023/A:1005889203677
|
| [10] |
Zukin LM, Hink EM, Liao S, et al. (2017) Endoscopic management of paranasal sinus mucoceles: meta-analysis of visual outcomes. Otolaryngol Head Neck Surg 157: 760-766. doi: 10.1177/0194599817717674
|
| [11] |
Victores A, Foroozan R, Takashima M (2012) Recurrent Onodi cell mucocele: rare cause of 2 different ophthalmic complications. Otolaryngol Head Neck Surg 146: 338-339. doi: 10.1177/0194599811415806
|
| [12] |
Evans C (1981) Aetiology and treatment of fronto-ethmoidal mucocele. J Laryngol Otol 95: 361-375. doi: 10.1017/S0022215100090836
|
| [13] |
Klink T, Pahnke J, Hoppe F, et al. (2000) Acute visual loss by an Onodi cell. Br J Ophthalmol 84: 801-802. doi: 10.1136/bjo.84.7.799d
|
| [14] |
Toh ST, Lee JCY (2007) Onodi cell mucocele: rare cause of optic compressive neuropathy. Arch Otolaryngol Head Neck Surg 133: 1153-1156. doi: 10.1001/archotol.133.11.1153
|
| [15] |
Chmielik LP, Chmielik A (2017) The prevalence of the Onodi cell - Most suitable method of CT evaluation in its detection. Int J Pediatr Otorhinolaryngol 97: 202-205. doi: 10.1016/j.ijporl.2017.04.001
|
| [16] |
Thanaviratananich S, Chaisiwamongkol K, Kraitrakul S, et al. (2003) The prevalence of an Onodi cell in adult Thai cadavers. Ear Nose Throat J 82: 200-204. doi: 10.1177/014556130308200314
|
| [17] |
Anniko M, Bernal-Sprekelsen M, Bonkowsky V, et al. (2010) Otorhinolaryngology, Head and Neck Surgery Berlin Heidelberg: Springer-Verlag New York. doi: 10.1007/978-3-540-68940-9
|
| [18] | Lim CC, Dillon WP, McDermott MW (1999) Mucocele involving the anterior clinoid process: MR and CT findings. AJNR Am J Neuroradiol 20: 287-290. |
| [19] |
Nickerson JP, Lane AP, Subramanian PS, et al. (2011) Onodi cell mucocele causing acute vision loss: radiological and surgical correlation. Clin Neuroradiol 21: 245-248. doi: 10.1007/s00062-011-0056-7
|
| [20] |
Ogata Y, Okinaka Y, Takahashi M (1998) Isolated mucocele in an Onodi cell. ORL J Otorhinolaryngol Relat Spec 60: 349-352. doi: 10.1159/000027623
|
| [21] |
Jones NS, Strobl A, Holland I (1997) A study of the CT findings in 100 patients with rhinosinusitis and 100 controls. Clin Otolaryngol Allied Sci 22: 47-51. doi: 10.1046/j.1365-2273.1997.00862.x
|
| [22] |
Chee E, Looi A (2009) Onodi sinusitis presenting with orbital apex syndrome. Orbit 28: 422-424. doi: 10.3109/01676830903177419
|
| [23] |
Bockmühl U, Kratzsch B, Benda K, et al. (2005) Paranasal sinus mucoceles: surgical management and long term results. Laryngorhinootologie 84: 892-898. (Article in German). doi: 10.1055/s-2005-870572
|
| [24] | Josepphson JS, Herrera A Mucocele of the paranasal sinuese: endoscopic diagnosis and treatment in Advanced Endoscopic Sinus Surgery (1995) .51-59. |
| [25] |
Lee JM, Au M (2016) Onodi cell mucocele: case report and review of the literature. Ear Nose Throat J 95: E4-8. doi: 10.1177/014556131609500905
|
| [26] |
Nathe C, Shen E, Crow RW (2018) Complete orbital apex syndrome from an onodi cell mucocele: a case report. Clin Ophthalmol 2: 63-66. doi: 10.35841/clinical-ophthalmology.2.2.63-66
|
| [27] |
Chafale VA, Lahoti SA, Pandit A, et al. (2015) Retrobulbar optic neuropathy secondary to isolated sphenoid sinus disease. J Neurosci Rural Pract 6: 238-240. doi: 10.4103/0976-3147.153233
|
| [28] | Tzamalis A, Diafas A, Riga P, et al. (2020) Onodi cell mucocele-associated optic neuropathy: a rare case report and review of the literature. J Curr Ophthalmol 32: 107-113. |
| [29] |
Kwon KW, Oh JS, Kim JW, et al. (2019) Onodi cell mucocele causing isolated trochlear nerve palsy: a case report. Medicine (Baltimore) 98: e15475. doi: 10.1097/MD.0000000000015475
|
| [30] |
Cheon YI, Hong SL, Roh HJ, et al. (2014) Fungal ball within Onodi cell mucocele causing visual loss. J Craniofac Surg 25: 512-514. doi: 10.1097/SCS.0000000000000678
|
| [31] | Wu W, Sun MT, Cannon PS, et al. (2010) Recovery of visual function in a patient with an onodi cell mucocele compressive optic neuropathy who had a 5-Week interval between onset and surgical intervention: a case report. J Ophthalmol 2010: 483056. |
| [32] |
Fukuda H, Fukumitsu R, Andoh M, et al. (2010) Small Onodi cell mucocele causing chronic optic neuropathy: case report. Neurol Med Chir (Tokyo) 50: 953-955. doi: 10.2176/nmc.50.953
|
| [33] | Eça TF, Rodrigues PC, Dinis PB (2018) Surgical drainage plus optic nerve decompression in acute optic neuropathy by an Onodi cell mucocele. BAOJ Surg 4: 33. |
| [34] | Fleissig E, Spierer O, Koren I, et al. (2014) Blinding orbital apex syndrome due to Onodi cell mucocele. Case Rep Ophthalmol Med 2014: 453789. |
| [35] | Kashii S, Arakawa N, Taguch HKN Acute visual loss caused by an Onodi cell mucocele (2016) .14. |
| [36] | Yen Nee See W, Sumugam K, Subrayan V (2016) Compressive optic neuropathy due to a large Onodi air cell: a case report and literature review. Allergy Rhinol (Providence) 7: 223-226. |
| [37] |
Loo JL, Looi ALG, Seah LL (2009) Visual outcomes in patients with paranasal mucoceles. Ophthal Plast Reconstr Surg 25: 126-129. doi: 10.1097/IOP.0b013e318198e78e
|
| [38] |
Kim YS, Kim K, Lee JG, et al. (2011) Paranasal sinus mucoceles with ophthalmologic manifestations: a 17-year review of 96 cases. Am J Rhinol Allergy 25: 272-275. doi: 10.2500/ajra.2011.25.3624
|
| [39] |
Kimakura M, Oishi A, Miyamoto K, et al. (2009) Sphenoethmoidal mucocele masquerading as trochlear palsy. J AAPOS 13: 598-599. doi: 10.1016/j.jaapos.2009.09.003
|
Figures(1) / Tables(4)

Turki M. Bin Mahfoz, Ahmad K. Alnemare. Optic neuropathy related to Onodi cell mucocele: a systematic review and meta-analysis of randomized controlled trials[J]. AIMS Medical Science, 2021, 8(3): 203-223. doi: 10.3934/medsci.2021018







 DownLoad:
DownLoad: