Research on the relationship between drugs and targets is the key to precision medicine. Ion channel is a kind of important drug targets. Aiming at the urgent needs of corona virus disease 2019 (COVID-19) treatment and drug development, this paper designed a mixed graph network model to predict the affinity between ion channel targets of COVID-19 and drugs. According to the simplified molecular input line entry specification (SMILES) code of drugs, firstly, the atomic features were extracted to construct the point sets, and edge sets were constructed according to atomic bonds. Then the undirected graph with atomic features was generated by RDKit tool and the graph attention layer was used to extract the drug feature information. Five ion channel target proteins were screened from the whole SARS-CoV-2 genome sequences of NCBI database, and the protein features were extracted by convolution neural network (CNN). Using attention mechanism and graph convolutional network (GCN), the extracted drug features and target features information were connected. After two full connection layers operation, the drug-target affinity was output, and model was obtained. Kiba dataset was used to train the model and determine the model parameters. Compared with DeepDTA, WideDTA, graph attention network (GAT), GCN and graph isomorphism network (GIN) models, it was proved that the mean square error (MSE) of the proposed model was decreased by 0.055, 0.04, 0.001, 0.046, 0.013 and the consistency index (CI) was increased by 0.028, 0.016, 0.003, 0.03 and 0.01, respectively. It can predict the drug-target affinity more accurately. According to the prediction results of drug-target affinity of SARS-CoV-2 ion channel targets, seven kinds of small molecule drugs acting on five ion channel targets were obtained, namely SCH-47112, Dehydroaltenusin, alternariol 5-o-sulfate, LPA1 antagonist 1, alternariol, butin, and AT-9283.These drugs provide a reference for drug repositioning and precise treatment of COVID-19.
Citation: Xianfang Wang, Qimeng Li, Yifeng Liu, Zhiyong Du, Ruixia Jin. Drug repositioning of COVID-19 based on mixed graph network and ion channel[J]. Mathematical Biosciences and Engineering, 2022, 19(4): 3269-3284. doi: 10.3934/mbe.2022151
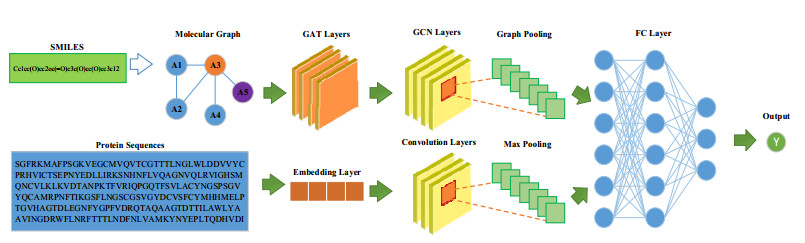
Research on the relationship between drugs and targets is the key to precision medicine. Ion channel is a kind of important drug targets. Aiming at the urgent needs of corona virus disease 2019 (COVID-19) treatment and drug development, this paper designed a mixed graph network model to predict the affinity between ion channel targets of COVID-19 and drugs. According to the simplified molecular input line entry specification (SMILES) code of drugs, firstly, the atomic features were extracted to construct the point sets, and edge sets were constructed according to atomic bonds. Then the undirected graph with atomic features was generated by RDKit tool and the graph attention layer was used to extract the drug feature information. Five ion channel target proteins were screened from the whole SARS-CoV-2 genome sequences of NCBI database, and the protein features were extracted by convolution neural network (CNN). Using attention mechanism and graph convolutional network (GCN), the extracted drug features and target features information were connected. After two full connection layers operation, the drug-target affinity was output, and model was obtained. Kiba dataset was used to train the model and determine the model parameters. Compared with DeepDTA, WideDTA, graph attention network (GAT), GCN and graph isomorphism network (GIN) models, it was proved that the mean square error (MSE) of the proposed model was decreased by 0.055, 0.04, 0.001, 0.046, 0.013 and the consistency index (CI) was increased by 0.028, 0.016, 0.003, 0.03 and 0.01, respectively. It can predict the drug-target affinity more accurately. According to the prediction results of drug-target affinity of SARS-CoV-2 ion channel targets, seven kinds of small molecule drugs acting on five ion channel targets were obtained, namely SCH-47112, Dehydroaltenusin, alternariol 5-o-sulfate, LPA1 antagonist 1, alternariol, butin, and AT-9283.These drugs provide a reference for drug repositioning and precise treatment of COVID-19.

| [1] |
K. Huang, T. Fu, L. M. Glass, M. Zitnik, C. Xiao, J. Sun, DeepPurpose: a deep learning library for drug–target interaction prediction, Bioinformatics, 36 (2020), 5545–5547. https://doi.org/10.1093/bioinformatics/btaa1005 doi: 10.1093/bioinformatics/btaa1005

|
| [2] |
T. U. Singh, S. Parida, M. C. Lingaraju, M. Kesavan, D. Kumar, R. K. Singh, Drug repurposing approach to fight COVID-19, Pharmacol. Rep., 72 (2020), 1479–1508. https://doi.org/10.1007/s43440-020-00155-6 doi: 10.1007/s43440-020-00155-6
|
| [3] |
R. Yan, Y. Zhang, Y. Li, L. Xia, Y. Guo, Q. Zhou, Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2, Science, 367 (2020), 1444–1448. https://doi.org/10.1126/science.abb2762 doi: 10.1126/science.abb2762
|
| [4] | A. Elfiky, N. S. Ibrahim, Anti-SARS and anti-HCV drugs repurposing against the Papain-like protease of the newly emerged coronavirus (2019-nCoV), preprint. https://doi.org/10.21203/rs.2.23280/v1 |
| [5] | R. Arya, A. Das, V. Prashar, M. Kumar, Potential inhibitors against papain-like protease of novel coronavirus (COVID-19) from FDA approved drugs, preprint, chemrXiv. https://doi.org/10.26434/chemrxiv.11860011 |
| [6] |
D. Zhang, K. Wu, X. Zhang, S. Deng, B. Peng, In silico screening of Chinese herbal medicines with the potential to directly inhibit 2019 novel coronavirus, J. Integr. Med., 18 (2020), 152–158. https://doi.org/10.1016/j.joim.2020.02.005 doi: 10.1016/j.joim.2020.02.005
|
| [7] |
A. S. Hauser, M. M. Attwood, M. Rask-Andersen, H. B. Schiöth, D. E. Gloriam, Trends in GPCR drug discovery: new agents, targets and indications, Nat. Rev. Drug Discovery, 16 (2017), 829–842. https://doi.org/10.1038/nrd.2017.178 doi: 10.1038/nrd.2017.178
|
| [8] | N. Wang, Y. Li, S. Liu, L. Gao, C. Liu, X. Bao, et al., Bioinformatics analysis and validation of differentially expressed microRNAs with their target genes involved in GLP-1RA facilitated osteogenesis, Curr. Bioinf., 16 (2021), 928–942. https://dx.doi.org/10.2174/1574893615999200508091615 |
| [9] |
D. Weininger, SMILES: a chemical language and information system, J. Chem. Inf. Comput. Sci., 28 (1988), 31–36. https://doi.org/10.1021/ci00057a005 doi: 10.1021/ci00057a005
|
| [10] |
B. R. Beck, B. Shin, Y. Choi, S. Park, K. Kang, Predicting commercially available antiviral drugs that may act on the novel coronavirus (SARS-CoV-2) through a drug-target interaction deep learning model, Comput. Struct. Biotechnol. J., 18 (2020), 784–790. https://doi.org/10.1016/j.csbj.2020.03.025 doi: 10.1016/j.csbj.2020.03.025
|
| [11] | T. N. Kipf, M. Welling, Semi-supervised classification with graph convolutional networks, in Proceedings of the International Conference on Learning Representations (ICLR), (2017). https://arXiv.org/abs/1609.02907 |
| [12] |
H. Jiang, P. Cao, M. Xu, J. Yang, Z. Osmar, Hi-GCN: a hierarchical graph convolution network for graph embedding learning of brain network and brain disorders prediction, Comput. Biol. Med., 127 (2020), 104096. https://doi.org/10.1016/j.compbiomed.2020.104096. doi: 10.1016/j.compbiomed.2020.104096
|
| [13] | P. Veličković, G. Cucurull, A. Casanova, A. Romero, P Liò, Y. Bengio, Graph attention networks, in Proceedings of the International Conference on Learning Representations (ICLR), (2018). https://doi.org/10.17863/CAM.48429 |
| [14] |
C. Yang, P. Wang, J. Tan, Q. Liu, X. Li, Autism spectrum disorder diagnosis using graph attention network based on spatial-constrained sparse functional brain networks, Comput. Biol. Med., 139 (2021), 104963–104963. https://doi.org/10.1016/j.compbiomed.2021.104963 doi: 10.1016/j.compbiomed.2021.104963
|
| [15] | K. Xu, W. Hu, J. Leskovec, S. Jegelka, How powerful are graph neural networks?, in Proceedings of the International Conference on Learning Representations (ICLR), 2019. https://arXiv.org/abs/1810.00826 |
| [16] |
H. Öztürk, A. Özgür, E. Ozkirimli, DeepDTA: deep drug-target binding affinity prediction, Bioinformatics, 34 (2018), 821–829. https://doi.org/10.1093/bioinformatics/bty593 doi: 10.1093/bioinformatics/bty593
|
| [17] | H. Öztürk, E. Ozkirimli, A. Özgür, WideDTA: prediction of drug-target binding affinity, preprint, arXiv: 1902.04166. https://arXiv.org/abs/1902.04166v1 |
| [18] | X. Guo, W. Zhou, B. Shi, et al., An efficient multiple kernel support vector regression model for assessing dry weight of hemodialysis patients, Curr. Bioinf., 16 (2021), 284–293. https://dx.doi.org/10.2174/1574893615999200614172536 |
| [19] |
N. J. Reynolds, S. W. Mccombie, B. B. Shankar, W. R. Bishop, G. J. Fisher, SCH 47112, a novel staurosporine derivative, inhibits 12-O-tetradecanoylphorbol-13-acetate-induced inflammation and epidermal hyperplasia in hairless mouse skin, Arch. Dermatol. Res., 289 (19979), 540–546. https://doi.org/10.1007/s004030050236 doi: 10.1007/s004030050236
|
| [20] |
I. Kruman, Q. Guo, M. P. Mattson, Calcium and reactive oxygen species mediate staurosporine-induced mitochondrial dysfunction and apoptosis in PC12 cells, J. Neurosci. Res., 51 (1998), 293–308. https://doi.org/10.1002/(SICI)1097-4547(19980201)51:3<293::AID-JNR3>3.0.CO;2-B doi: 10.1002/(SICI)1097-4547(19980201)51:3<293::AID-JNR3>3.0.CO;2-B
|
| [21] |
Y. Mizushina, N. Maeda, I. Kuriyama, H. Yoshida, Dehydroaltenusin is a specific inhibitor of mammalian DNA polymerase α, Expert Opin. Invest. Drugs, 20 (2011), 1523. https://doi.org/10.1517/13543784.2011.619977 doi: 10.1517/13543784.2011.619977
|
| [22] |
E Fliszár-Nyúl, B. Lemli, S. Kunsági-Máté, L. Dellafiora, C. Dall'Asta, G. Cruciani, et al., Interaction of mycotoxin alternariol with serum albumin, Int. J. Mol. Sci., 20 (2019), 2352. https://doi.org/10.3390/ijms20092352 doi: 10.3390/ijms20092352
|
| [23] |
J. Duan, Y. Guan, F. Mu, C. Guo, E. Zhang, Y. Yin, et al., Protective effect of butin against ischemia/reperfusion-induced myocardial injury in diabetic mice: involvement of the AMPK/GSK-3β/Nrf2 signaling pathway, Sci. Rep., 7 (2017), 41491. https://doi.org/10.1038/srep41491 doi: 10.1038/srep41491
|
| [24] |
S. Howard, V. Berdini, J. A. Boulstridge, M. G. Carr, D. M. Cross, J. Curry, et al., Fragment-based discovery of the pyrazol-4-yl urea (AT9283), a multitargeted kinase inhibitor with potent aurora kinase activity, J. Med. Chem., 52 (2009), 379–388. https://doi.org/10.1021/jm800984v doi: 10.1021/jm800984v
|
| [25] |
H. Li, Y. Gong, Y. Liu, H. Lin, G. Wang, Detection of transcription factors binding to methylated DNA by deep recurrent neural network, Briefings Bioinf., 2021 (2021), https://doi.org/10.1093/bib/bbab533. doi: 10.1093/bib/bbab533
|
| [26] |
L. Zhang, Y. Yang, L. Chai, Q. Li, J. Liu, H. Lin, et al., A deep learning model to identify gene expression level using co-binding transcription factor signals, Briefings Bioinf., 2021 (2021), https://doi.org/10.1093/bib/bbab501 doi: 10.1093/bib/bbab501
|
| [27] |
H. Lv, L. Shi, J. W. Berkenpas, F. Y. Dao, H. Zulfiqar, H. Ding, et al., Application of artificial intelligence and machine learning for COVID-19 drug discovery and vaccine design, Briefings Bioinf., 22 (2021), 1–10. https://doi.org/10.1093/bib/bbab320 doi: 10.1093/bib/bbab320
|
| [28] | Z. Chen, Q. Zhou, A. Khan, J. Jill, R. Xiong, X. Liu, New trends of deep learning in clinical cardiology, Curr. Bioinf., 16 (2021), 954–962. https://dx.doi.org/10.2174/1574893615999200719234517 |


Figures(3) / Tables(7)

Xianfang Wang, Qimeng Li, Yifeng Liu, Zhiyong Du, Ruixia Jin. Drug repositioning of COVID-19 based on mixed graph network and ion channel[J]. Mathematical Biosciences and Engineering, 2022, 19(4): 3269-3284. doi: 10.3934/mbe.2022151







 DownLoad:
DownLoad: