Citation: Dipo Aldila, Meksianis Z. Ndii, Brenda M. Samiadji. Optimal control on COVID-19 eradication program in Indonesia under the effect of community awareness[J]. Mathematical Biosciences and Engineering, 2020, 17(6): 6355-6389. doi: 10.3934/mbe.2020335

| [1] | WorldMeter, COVID-19 CORONAVIRUS PANDEMIC, available from: https://www.worldometers.info/coronavirus/#countries, accessed 02 July 2020. |
| [2] | Kementerian Kesehatan Republik Indonesia, Data Sebaran, available from: https://covid19.go.id/, accessed 02 July 2020. |
| [3] |
A. Abidemi, M. I. Abd. Aziz, R. Ahmad, Vaccination and vector control effect on dengue virus transmission dynamics: Modelling and simulation, Chaos Solitons Fractals, 133 (2020), 109648. doi: 10.1016/j.chaos.2020.109648

|
| [4] | N. Ganegoda, T. Gotz, K. P. Wijaya, An age-dependent model for dengue transmission: Analysis and comparison to field data, Appl. Math. Comput., 388 (2021), 125538. |
| [5] | A. Bustamam, D. Aldila, A. Yuwanda, Understanding Dengue Control for Short- and Long-Term Intervention with a Mathematical Model Approach, J. Appl. Math., 2018 (2018), 9674138. |
| [6] |
J. Mohammad-Awel, A. B. Gumel, Mathematics of an epidemiology-genetics model for assessing the role of insecticides resistance on malaria transmission dynamics, Math. Biosci., 312 (2019), 33-49. doi: 10.1016/j.mbs.2019.02.008
|
| [7] |
F. B. Agusto, S. Y. D. Valle, K. W. Blayneh, C. N. Ngonghala, M. J. Goncalves, N. Li, et al., The impact of bed-net use on malaria prevalence, J. Theor. Biol., 320 (2013), 58-65. doi: 10.1016/j.jtbi.2012.12.007
|
| [8] |
L. Cai, X. Li, N. Tuncer, M. Martcheva, A. A. Lashari, Optimal control of a malaria model with asymptomatic class and superinfection, Math. Biosci., 288 (2017), 94-108. doi: 10.1016/j.mbs.2017.03.003
|
| [9] |
S. Kim, A. Aurelio, E. Jung, Mathematical model and intervention strategies for mitigating tuberculosis in the Philippines, J Theor Biol., 443 (2018), 100-112. doi: 10.1016/j.jtbi.2018.01.026
|
| [10] | D. K. Das, S. Khajanci, T. K. Kar, The impact of the media awareness and optimal strategy on the prevalence of tuberculosis, Appl. Math. Comput., 366 (2020), 124732. |
| [11] |
G. O. Agaba, Y. N. Kyrychko, K. B. Blyuss, Mathematical model for the impact of awareness on the dynamics of infectious diseases, Math. Biosci., 286 (2017), 22-30. doi: 10.1016/j.mbs.2017.01.009
|
| [12] |
R. K. Rai, A. K. Misra, Y. Takeuchi, Modeling the impact of sanitation and awareness on the spread of infectious diseases, Math. Biosci. Eng., 16 (2019), 667-700. doi: 10.3934/mbe.2019032
|
| [13] |
A. K. Misra, R. K. Rai, Y. Takeuchi, Modeling the control of infectious diseases: Effects of TV and social media advertisements, Math. Biosci. Eng., 15 (2018), 1315-1343. doi: 10.3934/mbe.2018061
|
| [14] | K. Leung, J. T. Wu, D. Liu, G. M. Leung, First-wave covid-19 transmissibility and severity in china outside hubei after control measures, and second-wave scenario planning: a modelling impact assessment, The Lancet, 395 (2020), 1382-1393. |
| [15] |
A. J. Kucharski, T. W. Russell, C. Diamond, Y. Liu, J. Edmunds, S. Funk, et al., Early dynamics of transmission and control of covid-19: a mathematical modelling study, Lancet Infect. Dis., 20 (2020), 553-558. doi: 10.1016/S1473-3099(20)30144-4
|
| [16] | K. Prem, Y. Liu, T. W. Russell, A. J. Kucharski, R. M. Eggo, N. Davies, et al., The effect of control strategies to reduce social mixing on outcomes of the covid-19 epidemic in wuhan, china: a modelling study, Lancet Public Health, 5 (2020), e261-e270. |
| [17] | E. Soewono, On the analysis of covid-19 transmission in wuhan, diamond princess and jakartacluster, Commun. Biomath. Sci., 3 (2020), 9-18. |
| [18] | M. Z. Ndii, P. Hadisoemarto, D. Agustian, A. Supriatna, An analysis of covid-19 transmission in indonesia and saudi arabia, Commun. Biomath. Sci., 3 (2020), 19-27. |
| [19] |
S. E. Eikenberry, M. Mancuso, E. Iboi, T. Phan, K. Eikenberry, Y. Kuang, et al., To mask or not to mask: Modeling the potential for face mask use by the general public to curtail the covid-19 pandemic, Infect. Disease Model., 5 (2020), 293-308. doi: 10.1016/j.idm.2020.04.001
|
| [20] |
G. Giordano, F. Blanchini, R. Bruno, P. Colaneri, A. Di Filippo, A. Di Matteo, et al., Modelling the COVID-19 epidemic and implementation of population-wide interventions in Italy, Nat. Med., 26 (2020), 855-860. doi: 10.1038/s41591-020-0883-7
|
| [21] |
D. Aldila, S. H. Khoshnaw, E. Safitri, Y. R. Anwar, A. R. Bakry, B. M. Samiadji, et al., A mathematical study on the spread of covid-19 considering social distancing and rapid assessment: The case of jakarta, indonesia, Chaos Solitons Fractals, 139 (2020), 110042. doi: 10.1016/j.chaos.2020.110042
|
| [22] |
R. Li, S. Pei, B. Chen, Y. Song, T. Zhang, W. Yang, et al., Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2), Science, 368 (2020), 489-493. doi: 10.1126/science.abb3221
|
| [23] | The world bank: Awareness Campaigns Help Prevent Against COVID-19 in Afghanistan. Available from: https://www.worldbank.org/en/news/feature/2020/06/28/awareness-campaigns-help-prevent-against-covid-19-in-afghanistan. (Accessed 15 July 2020). |
| [24] |
M. S. Wolf, M. Serper, L. Opsasnick, R. M. O'Conor, L. M. Curtis, J. Y. Benavente, et al., Awareness, Attitudes, and Actions Related to COVID-19 Among Adults With Chronic Conditions at the Onset of the U.S. Outbreak: A Cross-sectional Survey, Ann. Intern. Med., 173 (2020), 100-109. doi: 10.7326/M20-1239
|
| [25] | Worldometer, COVID-19 CORONAVIRUS PANDEMIC, available from: https://www.worldometers.info/coronavirus/#countries (Accessed 25 August 2020). |
| [26] | Z. Feng, J. X. Velasco-Hernández, Competitive exclusion in a vector-host model for the dengue fever, J. Math. Biol., 35 (1997), 523-544. |
| [27] |
A. Davies, K. A. Thompson, K. Giri, G. Kafatos, J. Walker, A. Bennett, Testing the efficacy of homemade masks: would they protect in an influenza pandemic?, Disaster. Med. Public Health Prep., 7 (2013), 413-418. doi: 10.1017/dmp.2013.43
|
| [28] | N. M. Ferguson, D. Laydon, G. Nedjati-Gilani, N. Imai, K. Ainslie, M. Baguelin, et al., Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand, vol. 16, Imperial College COVID-19 Response Team, London, 2020. |
| [29] |
R. Li, S. Pei, B. Chen, Y. Song, T. Zhang, W. Yang, et al., Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-cov2), Science, 368 (2020), 489-493. doi: 10.1126/science.abb3221
|
| [30] |
Q. Li, X. Guan, P. Wu, X. Wang, L. Zhou, Y. Tong, et al., Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia, New Engl. J. Med., 382 (2020), 1199-1207. doi: 10.1056/NEJMoa2001316
|
| [31] |
S. A. Lauer, K. H. Grantz, Q. Bi, F. K. Jones, Q. Zheng, H. R. Meredith, et al., The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application, Ann. Int. Med., 172 (2020), 577-582. doi: 10.7326/M20-0504
|
| [32] |
C.-C. Lai, T.-P. Shih, W.-C. Ko, H.-J. Tang, P.-R. Hsueh, Severe acute respiratory syndrome coronavirus 2 (SARS-cov-2) and corona virus disease-2019 (COVID-19): The epidemic and the challenges, Int. J. Antimicrob. Ag., 55 (2020), 105924. doi: 10.1016/j.ijantimicag.2020.105924
|
| [33] |
C. del Rio, P. N. Malani, COVID-19-new insights on a rapidly changing epidemic, JAMA, 323 (2020), 1339-1340. doi: 10.1001/jama.2020.3072
|
| [34] |
R. M. Anderson, H. Heesterbeek, D. Klinkenberg, T. D. Hollingsworth, How will country-based mitigation measures influence the course of the COVID-19 epidemic?, Lancet, 395 (2020), 931-934. doi: 10.1016/S0140-6736(20)30567-5
|
| [35] | World Health Organization, Coronavirus disease 2019 (COVID-19): Situation report, 46, WHO (2020). |
| [36] |
B. Tang, X. Wang, Q. Li, N. L. Bragazzi, S. Tang, Y. Xiao, et al., Estimation of the transmission risk of the 2019-nCoV and its implication for public health interventions, J. Clin. Med., 9 (2020), 462. doi: 10.3390/jcm9020462
|
| [37] |
L. Zou, F. Ruan, M. Huang, L. Liang, H. Huang, Z. Hong, et al., SARS-CoV-2 viral load in upper respiratory specimens of infected patients, New Engl. J. Med., 382 (2020), 1177-1179. doi: 10.1056/NEJMc2001737
|
| [38] | G. Grasselli, A. Pesenti, M. Cecconi, Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: early experience and forecast during an emergency response, JAMA, 323 (2020), 1545-1546. |
| [39] |
C. N. Ngonghala, E. Iboi, S. Eikenberry, M. Scotch, C. R. Maclntyre, M. H. Bonds, et al., Mathematical assessment of the impact of non-pharmaceutical interventions on curtailing the 2019 novel Coronavirus, Math. Biosci., 325 (2020), 108364. doi: 10.1016/j.mbs.2020.108364
|
| [40] | O. Diekmann, J. A. Heesterbeek, M. G. Roberts, The construction of next-generation matrices for compartmental epidemic models, J. R. Soc. Interface, 4 (2010), 873-885. |
| [41] |
P. Van den Driessche, J. Watmough, Reproduction numbers and sub-threshold endemic equilibria for compartmental models of disease transmission, Math. Biosci., 180 (2002), 29-48. doi: 10.1016/S0025-5564(02)00108-6
|
| [42] | O. Diekmann, J. A. Heesterbeek, J. A. Metz, On the definition and the computation of the basic reproduction ratio R0 in models for infectious diseases in heterogeneous populations, J. Math. Biol., 28 (1990), 365-382. |
| [43] |
K. P. Wijaya, J. P. Chavez, D. Aldila, An epidemic model highlighting humane social awareness and vector-host lifespan ratio variation, Commun. Nonlinear Sci. Numer. Simulat., 90 (2020), 105389. doi: 10.1016/j.cnsns.2020.105389
|
| [44] | B. D. Handari, F. Vitra, R. Ahya, D. Aldila, Optimal control in a malaria model: intervention of fumigation and bed nets, Adv. Differ. Equations, 497 (2019), 497. |
| [45] |
D. Aldila, T. Götz, E. Soewono, An optimal control problem arising from a dengue disease trans-mission model, Math. Biosci., 242 (2013), 9-16. doi: 10.1016/j.mbs.2012.11.014
|
| [46] | D. Aldila, H. Seno, A Population Dynamics Model of Mosquito-Borne Disease Transmission, Focusing on Mosquitoes' Biased Distribution and Mosquito Repellent Use, Bull. Math. Biol., 81 (2020), 4977-5008. |
| [47] | S. M. Garba, A. B. Gumel, M. R. Abu Bakar, Backward bifurcations in dengue transmission dynamics, Math. Biosci., 215 (2008), 11-25. |
| [48] |
T. C. Reluga, J. Medlock, A. S. Perelson, Backward bifurcations and multiple equilibria in epidemic models with structured immunity, J. Theor. Biol., 252 (2008), 155-165. doi: 10.1016/j.jtbi.2008.01.014
|
| [49] | D. H. Knipl, G. Röst, Backward bifurcation in SIVS Model with immigration of Non-infectives, Biomath., 2 (2013), 1-14. |
| [50] |
C. Castillo-Chavez, B. Song, Dynamical models of tuberculosis and their applications, Math. Biosci. Eng., 1 (2004), 361-404. doi: 10.3934/mbe.2004.1.361
|
| [51] | L. S. Pontryagin, V. G. Boltyanskii, R. V. Gamkrelidze, E. F. Mishchenko, The mathematical theory of optimal processes, New York/London 1962. John Wiley & Sons. |
| [52] | F. B. Agusto, I. M. Elmojtaba, Optimal control and cost-effective analysis of malaria/visceral leishmaniasis co-infection, PLoS One, 12 (2017), e0171102. |
| [53] |
A. Kumar, P. K. Srivastava, Y. Dong, Y. Takeuchi, Optimal control of infectious disease: Information-induced vaccination and limited treatment, Physica A, 542 (2020), 123196. doi: 10.1016/j.physa.2019.123196
|
| [54] | H. R. Joshi, S. Lenhart, S. Hota, F. Agusto, Optimal control of an SIR model with changing behavior through an education campaign, Electron. J. Differ. Eq., 50 (2015), 1-14. |
| [55] |
M. Z. Ndii, F. R. Berkanis, D. Tambaru, M. Lobo, B. S. Djahi, Optimal control strategy for the effects of hard water consumption on kidney-related diseases, BMC Res. Notes, 13 (2020), 201. doi: 10.1186/s13104-020-05043-z
|
| [56] | Jakarta responses to COVID-19 official website. Available from: https://corona.jakarta.go.id/id |
| [57] | East Java responses to COVID-19 official website. Available from: http://infocovid19.jatimprov.go.id |
| [58] | Information center and coordination for COVID-19, West Java, official website. Available from: https://pikobar.jabarprov.go.id |
| [59] |
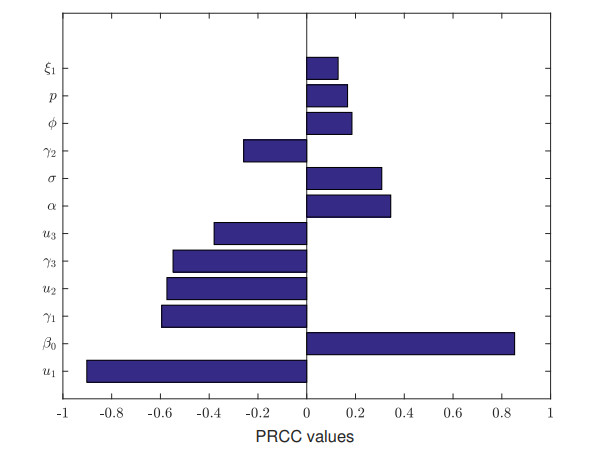
S. Marino, I. B. Hogue, C. J. Ray, D. E. Kirschner, A methodology for performing global uncertainty and sensitivity analysis in systems biology, J. Theor. Biol., 254 (2008), 178-196. doi: 10.1016/j.jtbi.2008.04.011
|
| [60] | M. Z. Ndii, B. S. Djahi, N. D. Rumlaklak, A. K. Supriatna, Determining the important parameters of mathematical models of the propagation of malware, in: M. A. Othman, M. Z. A. Abd Aziz, M. S. Md Saat, M. H. Misran (Eds.), Proceedings of the 3rd International Symposium of Information and Internet Technology (SYMINTECH 2018), Springer International Publishing, Cham, 2019, pp. 1-9. |
| [61] | S. Lenhart, J. T. & Workman Optimal control applied to biological models. CRC Press, 2007. |
Figures(10) / Tables(1)

Dipo Aldila, Meksianis Z. Ndii, Brenda M. Samiadji. Optimal control on COVID-19 eradication program in Indonesia under the effect of community awareness[J]. Mathematical Biosciences and Engineering, 2020, 17(6): 6355-6389. doi: 10.3934/mbe.2020335







 DownLoad:
DownLoad: