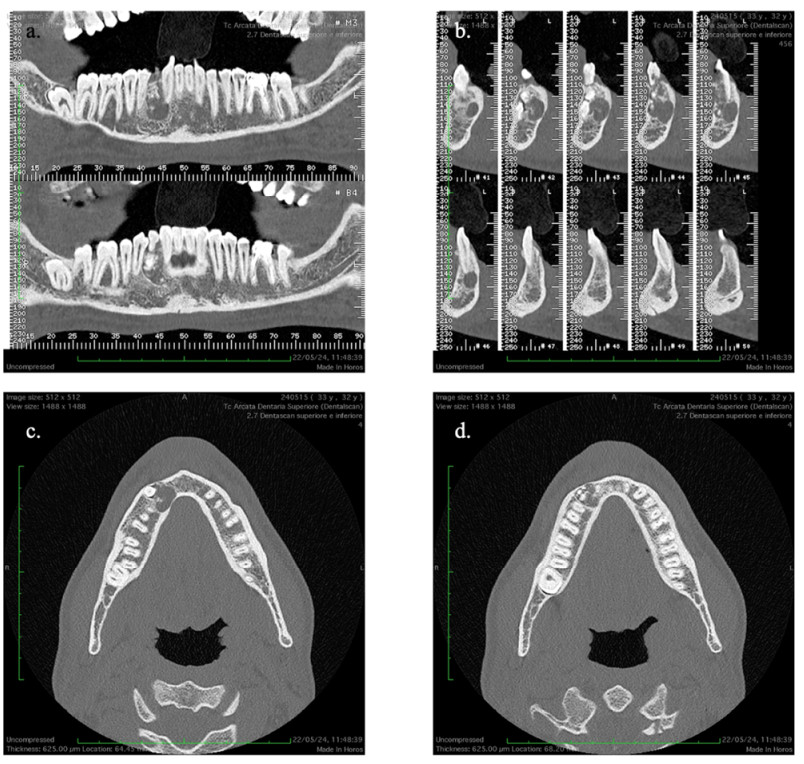
Odontomas account for a significant proportion of benign odontogenic tumors, often found incidentally due to their asymptomatic nature. This case report details a unique presentation of a mandibular compound odontoma in a 32-year-old male, resulting in the impaction of the mandibular right canine (tooth 4.3) and retention of the primary canine (tooth 8.3). Radiographic evaluation, including cone-beam computed tomography (CBCT), showed a radiopaque mixed lesion near the mandibular canal and the roots of adjacent teeth. Surgical management included the excision of the odontoma and extraction of the retained deciduous canine under local anesthesia, using rotary instruments to preserve adjacent structures. Postoperative healing was uneventful, with histopathological analysis confirming the lesion as a compound odontoma. This case underscores the significance of advanced imaging techniques in diagnosing and managing odontogenic lesions. It emphasizes the necessity for further research into alternative surgical methods and genetic factors influencing odontoma development.
Citation: Cesare D'Amico, Ankita Mathur, Rosaria Moscara, Aida Meto, Luca Fiorillo. A peculiar case of odontoma and impacted mandibular canine[J]. Journal of Dentistry and Multidisciplinary Sciences, 2025, 1(1): 4-12. doi: 10.3934/jdms.2025002
Odontomas account for a significant proportion of benign odontogenic tumors, often found incidentally due to their asymptomatic nature. This case report details a unique presentation of a mandibular compound odontoma in a 32-year-old male, resulting in the impaction of the mandibular right canine (tooth 4.3) and retention of the primary canine (tooth 8.3). Radiographic evaluation, including cone-beam computed tomography (CBCT), showed a radiopaque mixed lesion near the mandibular canal and the roots of adjacent teeth. Surgical management included the excision of the odontoma and extraction of the retained deciduous canine under local anesthesia, using rotary instruments to preserve adjacent structures. Postoperative healing was uneventful, with histopathological analysis confirming the lesion as a compound odontoma. This case underscores the significance of advanced imaging techniques in diagnosing and managing odontogenic lesions. It emphasizes the necessity for further research into alternative surgical methods and genetic factors influencing odontoma development.

| [1] |
M. A. Alarcón-Sánchez, G. Luna-Bonilla, S. Romero-Servin, A. Heboyan, Podoplanin immunoexpression in odontogenic lesions: a systematic review, meta-analysis, and integrated bioinformatic analysis, Diagn. Pathol., 19 (2024), 115. https://doi.org/10.1186/s13000-024-01540-y doi: 10.1186/s13000-024-01540-y

|
| [2] |
M. Cicciù, G. Cervino, L. Fiorillo, C. D'Amico, G. Oteri, G. Troiano, et al., Early diagnosis on oral and potentially oral malignant lesions: A systematic review on the Velscope® fluorescence method, Dent. J., 7 (2019), 93. https://doi.org/10.3390/dj7030093 doi: 10.3390/dj7030093
|
| [3] |
M. Mazur, G. Di Giorgio, A. Ndokaj, M. Jedliński, D. Corridore, B. Marasca, et al., Characteristics, diagnosis and treatment of compound odontoma associated with impacted teeth, Children (Basel) 9 (2022), 1509. https://doi.org/10.3390/children9101509 doi: 10.3390/children9101509
|
| [4] |
A. B. Rajendra Santosh, O. E. Ogle, Odontogenic tumors, Dent. Clin. North Am., 64 (2020), 121–138. https://doi.org/10.1016/j.cden.2019.08.008 doi: 10.1016/j.cden.2019.08.008
|
| [5] |
P. Tyagi, S. Singla, Complex composite odontoma, Int. J. Clin. Pediatr. Dent., 3 (2010), 117–120. https://doi.org/10.5005/jp-journals-10005-1066 doi: 10.5005/jp-journals-10005-1066
|
| [6] |
C. M. Ribeiro, T. T. Santos, S. R. de Castro, M. L. de Carli, F. F. Sperandio, J. A. Hanemann, et al., Extensive mandibular ameloblastic fibro-odontoma, J. Craniofac. Surg., 27 (2016), e563–565. https://doi.org/10.1097/scs.0000000000002869 doi: 10.1097/scs.0000000000002869
|
| [7] |
A. Liu, M. Wu, X. Guo, H. Guo, Z. Zhou, K. Wei, et al., Clinical, pathological, and genetic evaluations of Chinese patient with otodental syndrome and multiple complex odontoma: Case report, Medicine (Baltimore), 96 (2017), e6014. https://doi.org/10.1097/MD.0000000000006014 doi: 10.1097/MD.0000000000006014
|
| [8] |
P. W. Kämmerer, D. Schneider, E. Schiegnitz, S. Schneider, C. Walter, B. Frerich, et al., Clinical parameter of odontoma with special emphasis on treatment of impacted teeth—a retrospective multicentre study and literature review, Clin. Oral Investig., 20 (2016), 1827–1835. https://doi.org/10.1007/s00784-015-1673-3 doi: 10.1007/s00784-015-1673-3
|
| [9] |
F. Ide, S. Sakamoto, Y. Miyazaki, M. Nishimura, T. Muramatsu, K. Kikuchi, Revisiting the history of odontoma, with special reference to its original illustration, Head Neck Pathol., 17 (2023), 976–983. https://doi.org/10.1007/s12105-023-01593-3 doi: 10.1007/s12105-023-01593-3
|
| [10] | M. Kumar, M. Goyal, A. Kaur, A. D. Jain, A. Maheshwari, Orthodontic management after unilateral extraction of a compound odontoma and an impacted canine, J. Clin. Orthod., 57 (2023), 101–109. |
| [11] |
M. Terauchi, S. Akiya, J. Kumagai, Y. Ohyama, S. Yamaguchi, An analysis of dentigerous cysts developed around a mandibular third molar by panoramic radiographs, Dent. J. (Basel), 7 (2019), 13. https://doi.org/10.3390/dj7010013 doi: 10.3390/dj7010013
|
| [12] |
A. Vitale, S. Battaglia, S. Crimi, C. Ricceri, G. Cervino, M. Cicciù, et al., Spontaneous bone regeneration after enucleation of mandibular cysts: Retrospective analysis of the volumetric increase with a full-3d measurement protocol, Appl. Sci., 11 (2021), 4731. https://doi.org/10.3390/app11114731 doi: 10.3390/app11114731
|
| [13] |
S. K. Marappa Sathyamoorthy, H. Chakrika, M. Dhinakaran, CBCT-guided management of compound odontome, BMJ Case Rep., 14 (2021), e244457. https://doi.org/10.1136/bcr-2021-244457 doi: 10.1136/bcr-2021-244457
|
| [14] |
L. A. A. Aly, Piezoelectric surgery: Applications in oral & maxillofacial surgery, Future Dent. J., 4 (2018), 105–111. https://doi.org/https://doi.org/10.1016/j.fdj.2018.09.002 doi: 10.1016/j.fdj.2018.09.002
|
| [15] |
G. Isola, M. Cicciù, L. Fiorillo, G. Matarese, Association between odontoma and impacted teeth, J. Craniofac. Surg., 28 (2017), 755–758. https://doi.org/10.1097/scs.0000000000003433 doi: 10.1097/scs.0000000000003433
|
| [16] |
J. M. Abrahams, S. A. McClure, Pediatric odontogenic tumors, Oral Maxillofac. Surg. Clin. North Am., 28 (2016), 45–58. https://doi.org/10.1016/j.coms.2015.08.003 doi: 10.1016/j.coms.2015.08.003
|
| [17] |
V. A. da Silva, R. P. Pedreira, F. F. Sperandio, D. A. Nogueira, M. L. de Carli, J. A. Hanemann, Odontomas are associated with impacted permanent teeth in orthodontic patients, J. Clin. Exp. Dent., 11 (2019), e790–e794. https://doi.org/10.4317/jced.56101 doi: 10.4317/jced.56101
|
| [18] |
M. B. Erden Sahin, A. Calis, H. Koca, An unusual case of 177 pieces of mandibular compound odontoma: 10-year follow-up, J. Stomatol. Oral Maxillofac. Surg., 121 (2020), 585–588. https://doi.org/10.1016/j.jormas.2020.03.013 doi: 10.1016/j.jormas.2020.03.013
|
| [19] |
D. Mehta, N. Raval, S. Udhani, V. Parekh, C. Modi, An unusual case report of erupted odontoma, Case Rep. Dent., 2013 (2013), 570954. https://doi.org/10.1155/2013/570954 doi: 10.1155/2013/570954
|
| [20] |
M. Soluk-Tekkesin, R. Bologna-Molina, K. Magliocca, W. van Heerden, L. Robinson, E. A. Bilodeau, et al., Malformations vs. neoplasia in the oral cavity: special emphasis on mixed odontogenic tumors, J. Oral Pathol. Med., 54 (2025), 76–79. https://doi.org/10.1111/jop.13592 doi: 10.1111/jop.13592
|
| [21] |
R. Sorrentino, M. I. Di Mauro, G. Ruggiero, R. Leone, E. Ferrari Cagidiaco, M. Annunziata, et al., Implant-prosthetic rehabilitation of the agenesis of maxillary lateral incisors: a 2-year prospective clinical study with full digital workflow, Prosthesis, 6 (2024), 803–816. https://doi.org/10.3390/prosthesis6040057 doi: 10.3390/prosthesis6040057
|
| [22] |
K. A. DeColibus, D. S. Rasner, O. Okhuaihesuyi, A. A. Owosho, Clinicoradiopathologic analysis of odontomas: a retrospective study of 242 cases, Dent. J., 11 (2023), 253. https://doi.org/10.3390/dj11110253 doi: 10.3390/dj11110253
|



Figures(4)
Cesare D'Amico, Ankita Mathur, Rosaria Moscara, Aida Meto, Luca Fiorillo. A peculiar case of odontoma and impacted mandibular canine[J]. Journal of Dentistry and Multidisciplinary Sciences, 2025, 1(1): 4-12. doi: 10.3934/jdms.2025002







 DownLoad:
DownLoad: