Citation: Milena T. Pelegrino, Amedea B. Seabra. Chitosan-Based Nanomaterials for Skin Regeneration[J]. AIMS Medical Science, 2017, 4(3): 352-381. doi: 10.3934/medsci.2017.3.352

| [1] | Gantwerker EA, Hom DB (2011) Skin: histology and physiology of wound healing. Facial Plast Surg Clin N Am 19: 441-453. |
| [2] | Sorg H, Tilkorn DJ, Hager S, et al. (2017) Skin wound healing: An update on the current knowledge and concepts. Eur Surg Res 58: 81-94. |
| [3] | Gonzalez ACD, Costa TF, Andrade ZD, et al. (2016) Wound healing-A literature review. An Bras Dermatol 91: 614-620. |
| [4] | Ahmed S, Ikram S (2016) Chitosan based scaffolds and their applications in wound healing. Achievements Life Sci 10: 27-37. |
| [5] | Azuma K, Izumi R, Osaki T, et al. (2015) Chitin, chitosan, and its derivatives for wound healing: Old and new materials. J Funct Biomater 6: 104-142. |
| [6] | Cortivo R, Vindigni V, Iacobellis L, et al. (2010) Nanoscale particle therapy for wounds and ulcers. Nanomedicine 5: 641-656. |
| [7] | Andrews JP, Marttala J, Macarak E, et al. (2016) Keloids: The paradigm of skin fibrosis – Pathomechanisms and treatment. Matrix Biol 51: 37-46. |
| [8] | Mari W, Alsabri SG, Tabal N, et al. (2015) Novel insights on understanding of keloid scar: Article review. J Am Coll Clin Wound Spec 7: 1-7. |
| [9] | Mordorski B, Prow T (2016) Nanomaterials for wound healing. Curr Dermatol Rep 5: 278-286. |
| [10] | Ahmadi F, Oveisi Z, Samani M, et al. (2015) Chitosan based hydrogels: characteristics and pharmaceutical applications. Res Pharm Sci 10: 1-16. |
| [11] | Elgadir MA, Uddin MS, Ferdosh S, et al. (2015) Impact of chitosan composites and chitosan nanoparticle composites on various drug delivery systems: A review. J Food Drug Anal 23: 619-629. |
| [12] | Patel S, Goyal A (2017) Chitin and chitinase: Role in pathogenicity, allergenicity and health. Int J Biol Macromolec 97: 331-338. |
| [13] | Baldrick P (2010) The safety of chitosan as a pharmaceutical excipient. Regul Toxicol Pharmacol 56: 290-299. |
| [14] | Dutta PK (2016) Chitin and chitosan for regenerative medicine. Springer India: 2511-2519. |
| [15] | Chaudhari AA, Vig K, Baganizi DR (2016) Future prospects for scaffolding methods and biomaterials in skin tissue engineering: A review. Int J Mol Sci 17: 1974. |
| [16] | Parani M, Lokhande G, Singh A, et al. (2016) Engineered nanomaterials for infection control and healing acute and chronic wounds. ACS Appl Mater Interfaces 8: 10049-10069. |
| [17] | Siravam AJ, Rajitha P, Maya S, et al. (2015) Nanogels for delivery, imaging and therapy. WIREs Nanomed Nanobiotechnol 7: 509-533. |
| [18] | Kean T, Thanou M (2010) Biodegradation biodistribution and toxicity of chitosan. Adv Drug Deliv Rev 62: 3-11. |
| [19] | Moura MJ, Brochado J, Gil MH, et al. (2017) In situ forming chitosan hydrogels: Preliminary evaluation of the in vivo inflammatory response. Mater Sci Eng C 75: 279-285. |
| [20] | Zhao Y, Qiu Y, Wang H, et al. (2016) Preparation of nanofibers with renewable polymers and their application in wound dressing. Int J Polym Sci. Article ID 4672839. doi: http://dx.doi.org/10.1155/2016/4672839. |
| [21] | Jayakumar R, Menon D, Manzoor K, et al. (2010) Biomedical applications of chitin and chitosan based nanomaterials-A short review. Carbohydr Polym 82: 227-232. |
| [22] |
|
| [23] | Yildirimer L, Thanh NTK, Seifalian AM (2012) Skin regeneration scaffolds: a multimodal bottom-up approach. Trends Biotechnol 30: 638-648. |
| [24] | Chen JP, Chang GY, Chen JK (2008) Electrospun collagen/chitosan nanofibrous membrane as wound dressing. Colloids Surf A 313-314: 183-188. |
| [25] | Sun K, Li ZH (2011) Preparations, properties and applications of chitosan based nanofibers fabricated by electrospinning. Express Polym Lett 5: 342-361. |
| [26] | Muzzarelli RAA, Mehtedi ME, Mattioli-Belmonte M (2014) Emerging biomedical applications of nano-chitins and nano-chitosans obtained via advanced eco-Friendly technologies from marine resources. Mar Drugs 12: 5468-5502. |
| [27] | Oyarzun-Ampuero F, Vidal A, Concha M, et al. (2015) Nanoparticles for the treatment of wounds. Curr Pharm Des 221: 4329-4341. |
| [28] | Manchanda R, Surendra N (2010) Controlled size chitosan nanoparticles as an efficient. Biocompatible oligonucleotides delivery system. J Appl Polym Sci 118: 2071-2077. |
| [29] | Brunel F, Véron L, David L, et al. (2008) A novel synthesis of chitosan nanoparticles in reverse emulsion. Langmuir 24: 11370-11377. |
| [30] | Tokumitsu H, Ichikawa H, Fukumori Y, et al. (1999) Preparation of gadopentetic acid- loaded chitosan microparticles for gadoliniumneutron-capture therapy of cancer by a novel emulsion-droplet coalescence technique. Chem Pharm Bull 47: 838-842. |
| [31] | Agnihotri S, Aminabhavi TM (2007) Chitosan nanoparticles for prolonged delivery of timolol maleate. Drug Dev Ind Pharm 33: 1254-1262. |
| [32] | El-Shabouri MH (2002) Positively charged nanoparticles for improving theoral bioavailability of cyclosporin-A. Int J Pharm 249: 101-108. |
| [33] | Cardozo VF, Lancheros CAC, Narciso AM, et al. (2041) Evaluation of antibacterial activity of nitric oxide-releasing polymeric particles against Staphylococcus aureus from bovine mastitis. Int J Pharm 473: 20-29. |
| [34] | Pelegrino MT, Silva LC, Watashi CM, et al (2017) Nitric oxide-releasing nanoparticles: synthesis, characterization, and cytotoxicity to tumorigenic cells. J Nanopart Res 19: 57. |
| [35] | Pelegrino MT, Weller RB, Chen X, et al. (2017) Chitosan nanoparticles for nitric oxide delivery in human skin. Med Chem Comm 4: 713-719. |
| [36] | Bugnicourt L, Ladavière C (2016) Interests of chitosan nanoparticles ionically cross-linked with tripolyphosphate for biomedical applications. Prog Polym Sci 60: 1-17. |
| [37] | Soni KS, Desale SS, Bronich TK (2016) Nanogels: An overview of properties, biomedical applications and obstacles to clinical translation. J Control Release 240: 109-126. |
| [38] | Caló E, Khutoryanskiy V (2015) Biomedical applications of hydrogels: A review of patents and commercial products. Eur Polym J 65: 252-267. |
| [39] | Huang R, Li W, Lv X, et al. (2015) Biomimetic LBL structured nanofibrous matrices assembled by chitosan/collagen for promoting wound healing. Biomaterials 53: 58-75. |
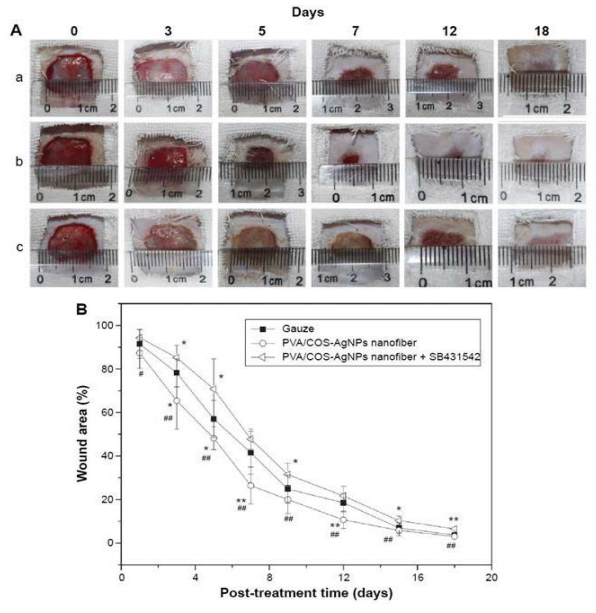
| [40] | Li CW, Wang Q, Li J, et al. (2016) Silver nanoparticles/chitosan oligosaccharide/poly(vinyl alcohol) nanofiber promotes wound healing by activating TGFβ1/Smad signaling pathway. Int J Nanomedicine 11: 373-387. |
| [41] | Liu M, Shen Y, Ao P, et al. (2014) The improvement of hemostatic and wound healing property of chitosan by halloysite nanotubes. RSC Adv 4: 23540-23553. |
| [42] |
Mahdavi M, Mahmoudi N, Anaran FR, et al. (2016) Electrospinning of nanodiamond-modified polysaccharide nanofibers with physico-mechanical properties close to natural skins. Mar Drugs 14: 128. doi: 10.3390/md14070128

|
| [43] | Georgii JL, Amadeu TP, Seabra AB, et al. (2011). Topical S-nitrosoglutathione-releasing hydrogel improves healing of rat ischemic wounds. J Tissue Eng Regen Med 5: 612-619. |
| [44] | Zhou X, Wang H, Zhang J, et al. (2017) Functional poly(ε-caprolactone)/chitosan dressings with nitric oxide-releasing property improve wound healing. Acta Biomater 54: 128-137. |
| [45] | Veleirinho B, Coelho DS, Dias PF, et al. (2012) Nanofibrous poly(3-hydroxybutyrate-co-3-hydroxyvalerate)/chitosan scaffolds for skin regeneration. Int J Biol Macromolec 51: 343-350. |
| [46] | Archana D, Dutta J, Dutta PK (2013) Evaluation of chitosan nano dressing for wound healing: Characterization, in vitro and in vivo studies. Int J Biol Macromolec 57: 193-203. |
| [47] | Cao H, Chen MM, Liu Y, et al. (2015) Fish collagen-based scaffold containing PLGA microspheres for controlled growth factor delivery in skin tissue engineering. Colloids Surf B Biointerfaces 136: 1098-1106. |
| [48] | Gharatape A, Milani M, Rasta SH, et al. (2016) A novel strategy for low level laser-induced plasmonic photothermal therapy: the efficient bactericidal effect of biocompatible AuNPs@(PNIPAAM-co-PDMAEMA, PLGA and chitosan). RSC Adv 6: 110499-110510. |
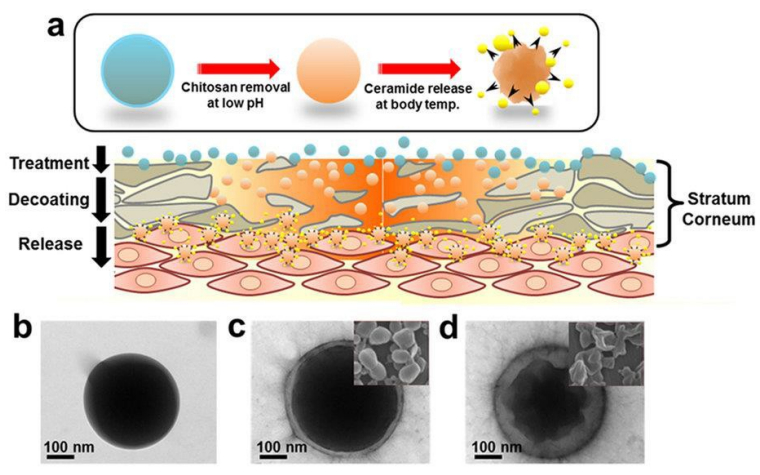
| [49] | Jung SM, Yoon GH, Lee HC, et al. (2015) Thermodynamic insights and conceptual design of skin sensitive chitosan coated ceramide/PLGA nanodrug for regeneration of Stratum corneum on atopic dermatitis. Sci Rep 5: 18089. |
| [50] | Seabra AB, Kitice NA, Pelegrino MT, et al. (2015) Nitric oxide-releasing polymeric nanoparticles against Trypanosoma cruzi. J Phys: Conf Series 617: 012020. |
| [51] | Seabra AB, Duran N (2012) Nanotechnology allied to nitric oxide release materials for dermatological applications. Curr Nanosci 8: 520-525. |
| [52] | Seabra AB, Duran N (2017) Nanoparticulated nitric oxide donors and their biomedical applications. Mini Rev Med Chem 17: 216-223. |
| [53] | Han G, Martinez LR, Mihu MR, et al. (2009) Nitric oxide releasing nanoparticles are therapeutic for Staphylococcus aureus abscesses in a murine model of infection. PLoS One 4: e7804. |
| [54] | Shome S, Das TA, Choudhury MD, et al. (2016) Curcumin as potential therapeutic natural product: a nanobiotechnological perspective. J Pharm Pharmacol 68: 1481-1500. |
| [55] | Karri VV, Kuppusamy G, Talluri SV, et al. (2016) Curcumin loaded chitosan nanoparticles impregnated into collagen-alginate scaffolds for diabetic wound healing. Int J Biol Macromol 93: 1519-1529. |
| [56] | SeabraAB, Pankotai E, Feher M, et al. (2007) S-nitrosoglutathione-containing hydrogel increases dermal blood flow in streptozotocin-induced diabetic rats. Br J Dermatol 156: 814-818. |
| [57] | Lin YH, Lin JH, Hong YS (2017). Development of chitosan/poly-g-glutamic acid/pluronic/curcumin nanoparticles in chitosan dressings for wound regeneration. J Biomed Mater Res Part B 105B: 81-90. |
| [58] | Lin YH, Lin JH, Li TS, et al. (2016) Dressing with epigallocatechin gallate nanoparticles for wound regeneration. Wound Repair Regen 24: 287-301. |
| [59] | Nawaz A, Wong TW (2017) Microwave as skin permeation enhancer for transdermal drugdelivery of chitosan-5-fluorouracil nanoparticles. Carbohydr Polym 157: 906-919. |
| [60] | Piras AM, Maisetta G, SandreschiS, et al. (2015) Chitosan nanoparticles loaded with the antimicrobial peptide temporin B exert a long-term antibacterial activity in vitroagainst clinical isolates of Staphylococcus epidermidis. Front Microbiol 6: 372. |
| [61] | Ramasamy T, Kim JO, Yong CS, et al. (2015) Novel core–shell nanocapsules for the tunable delivery of bioactive rhEGF: Formulation, characterization and cytocompatibility studies. J Biomater Tissue Eng 5: 730-743. |
| [62] | Romić MD, Klarić MŠ, Lovrić J, et al. (2016) Melatonin-loaded chitosan/Pluronic® F127 microspheres as in situforming hydrogel: An innovative antimicrobial wound dressing. Eur J Pharm Biopharm 107: 67-79. |
| [63] | Abureesh MA, Oladipo AA, Gazi M (2016) Facile synthesis of glucose-sensitive chitosan-poly(vinyl alcohol) hydrogel: Drug release optimization and swelling properties. Int J Biol Macromol 90: 75-80. |
| [64] | Zhao X, Zou X, Ye L (2016) Controlled pH-and glucose-responsive drug release behavior of cationic chitosan based nano-composite hydrogels by using graphene oxide as drug nanocarrier. J Ind Eng Chem: 1-10. |
| [65] | Neufeld L, Bianco-Peled H (2017) Pectin–chitosan physical hydrogels as potential drug delivery vehicles. Int J Biol Macromol 101: 852-861. |
| [66] | Rogina A, Ressler A, Matic I, et al. (2017) Cellular hydrogels based on pH-responsive chitosan-hydroxyapatite system. Carbohydr Polym 166: 173-182. |
| [67] | Sapru S, Ghosh AK, Kundu SC (2017) Non-immunogenic, porous and antibacterial chitosan and Antheraea mylitta silk sericin hydrogels as potential dermal substitute. Carbohydr Polym 167: 196-209. |
| [68] | Wahid F, Wang HS, Zhong C, et al. (2017) Facile fabrication of moldable antibacterial carboxymethyl chitosan supramolecular hydrogels cross-linked by metal ions complexation. Carbohydr Polym 165: 455-461. |
| [69] | Yu S, Zhang X, Tan G, et al. (2017) A novel pH-induced thermosensitive hydrogel composed of carboxymethyl chitosan and poloxamer cross-linked by glutaraldehyde for ophthalmic drug delivery. Carbohydr Polym 155: 208-217. |
| [70] | Mohan N, Mohanan PV, Sabareeswaran A (2017) Chitosan-hyaluronic acid hydrogel for cartilage repair. Int J Biol Macromol. |
| [71] | Mozalewska W, Czechowska-Biskup R, Olejnik AK, et al. (2017) Chitosan-containing hydrogel wound dressings prepared by radiation technique. Radiat Phys Chem134: 1-7. |
| [72] | Croisier F, Jérôme C (2013) Chitosan-based biomaterials for tissue engineering. Eur Polym J 49: 780-792. |
| [73] | Carvalho IC, Mansur HS (2017) Engineered 3D-scaffolds of photocrosslinked chitosan-gelatin hydrogel hybrids for chronic wound dressings and regeneration. Mater Sci 93: 1519-1529. |
| [74] | Mohan N, Mohanan PV, Sabareeswaran A (2017) Chitosan-hyaluronic acid hydrogel for cartilage repair. Int J Biol Macromol. |
| [75] | Mozalewska W, Czechowska-Biskup R, Olejnik AK, et al. (2017) Chitosan-containing hydrogel wound dressings prepared by radiation technique. Radiat Phys Chem 134: 1-7. |
| [76] | Giri TK, Thakur A, Alexander A, et al. (2012) Modified chitosan hydrogels as drug delivery and tissue engineering systems: present status and applications. Acta Pharm Sin B 2: 439-449. |
| [77] |
Santos JCC, Mansur AAP, Mansur HS (2013) One-step biofunctionalization of quantum dots with chitosan and n-palmitoyl chitosan for potential biomedical applications. Molecules 18: 6550-6572. doi: 10.3390/molecules18066550
|
| [78] | Medeiros FGLB, Mansur AAP, Chagas P, et al. (2015) O-carboxymethyl functionalization of chitosan: Complexation and adsorption of Cd (II) and Cr (VI) as heavy metal pollutant ions. React Funct Polym 97: 37-47. |
| [79] | Yu P, Bao R-Y, Shi X-J, et al. (2017) Self-assembled high-strength hydroxyapatite/graphene oxide/chitosan composite hydrogel for bone tissue engineering. Carbohydr Polym 155: 507-515. |
| [80] | Liu X, Chen Y, Huang Q, et al. (2014) A novel thermo-sensitive hydrogel based on thiolated chitosan/ hydroxyapatite/beta-glycerophosphate. Carbohydr Polym 110: 62-69. |
| [81] | Song K, Li L, Yan X, et al. (2017) Characterization of human adipose tissue-derived stem cells in vitro culture and in vivo differentiation in a temperature-sensitive chitosan/B- glycerophosphate/collagen hybrid hydrogel. Mater Sci Eng C 70: 231-240. |
| [82] | Bao Z, Jiang C, Wang Z, et al. (2017) The influence of solvent formulations on thermosensitive hydroxybutyl chitosan hydrogel as a potential delivery matrix for cell therapy. Carbohydr Polym 170: 80-88. |
| [83] | Zhang Y, Dang Q, Liu C, et al. (2017) Synthesis, characterization, and evaluation of poly(aminoethyl) modified chitosan and its hydrogel used as antibacterial wound dressing. Int J Biol Macromol 102: 457-467. |
| [84] | Rabea EI, Badawy MET, Stevens C V, et al. (2003) Chitosan as antimicrobial agent: Applications and mode of action. Biomacromolecules 4: 1457-1465. |
| [85] | Zakrzewska A, Boorsma A, Delneri D, et al. (2007) Cellular processes and pathways that protect Saccharomyces cerevisiae cells against the plasma membrane-perturbing compound chitosan. Eukaryot Cell 6: 600-608. |
| [86] | Song Y, Zhang D, Lv Y, et al. (2016) Microfabrication of a tunable collagen/alginate-chitosan hydrogel membrane for controlling cell-cell interactions. Carbohydr Polym 153 :652-662. |
| [87] | Dang Q, Liu K, Zhang Z, et al. (2017) Fabrication and evaluation of thermosensitivechitosan/collagen/α, β-glycerophosphate hydrogels for tissue regeneration. Carbohydr Polym 167: 145-157. |
| [88] | Heris HK, Latifi N, Vali H, et al (2015) Investigation of Chitosan-glycol/glyoxal as an injectable biomaterial for vocal fold tissue engineering. Procedia Eng 110: 143-150. |
| [89] | Yap LS, Yang MC (2016) Evaluation of hydrogel composing of Pluronic F127 and carboxymethyl hexanoyl chitosan as injectable scaffold for tissue engineering applications. Colloids Surf B 146: 204-211. |
| [90] | Malli S, Bories C, Pradines B, et al. (2017) In situ forming Pluronic® F127/chitosan hydrogel limits metronidazole transmucosal absorption. Eur J Pharm Biopharm 112: 143-147. |
| [91] | Molina MM, Seabra AB, de Oliveira MG, et al. (2013) Nitric oxide donor superparamagnetic ironoxide nanoparticles. Mater Sci Eng C Mater Biol Appl 33: 746-751. |
| [92] | Ong SY, Wu J, Moochhala SM, et al. (2008) Development of a chitosan-based wound dressing with improved hemostatic and antimicrobial properties. Biomaterials 29: 4323-4332. |
| [93] | Zhou Y, Zhao Y, Wang L, et al. (2012) Radiation synthesis and characterization of nanosilver/gelatin/carboxymethyl chitosan hydrogel. Radiat Phys Chem 81: 553-560. |
| [94] | Sudheesh KPT, Lakshmanan VK, Anilkumar TV, et al. (2012) Flexible and microporous chitosan hydrogel/nano ZnO composite bandages for wound dressing: In vitroand in vivoevaluation. ACS Appl Mater Interfaces 4: 2618-2629. |
| [95] | Yang JA, Yeom J, Hwang BW, et al. (2014) In situ-forming injectable hydrogels for regenerative medicine. Prog Polym Sci 39: 1973-1986. |
| [96] | Hoffman AS (2012) Hydrogels for biomedical applications. Adv Drug DelivRev 64: 18-23. |
| [97] | Cheng NC, Lin WJ, Ling TY, et al. (2017) Sustained release of adipose-derived stem cells by thermosensitive chitosan/gelatin hydrogel for therapeutic angiogenesis. Acta Biomater 51: 258-267. |
| [98] | Zhang D, Zhou W, Wei B, et al. (2015) Carboxyl-modified poly(vinyl alcohol)-crosslinked chitosan hydrogel films for potential wound dressing. Carbohydr Polym 125: 189-199. |
| [99] | Duran N, Duran M, de Jesus MB, et al. (2016) Silver nanoparticles: A new view on mechanistic aspects on antimicrobial activity. Nanomedicine 12: 789-799. |
Figures(4) / Tables(3)

Milena T. Pelegrino, Amedea B. Seabra. Chitosan-Based Nanomaterials for Skin Regeneration[J]. AIMS Medical Science, 2017, 4(3): 352-381. doi: 10.3934/medsci.2017.3.352







 DownLoad:
DownLoad: