




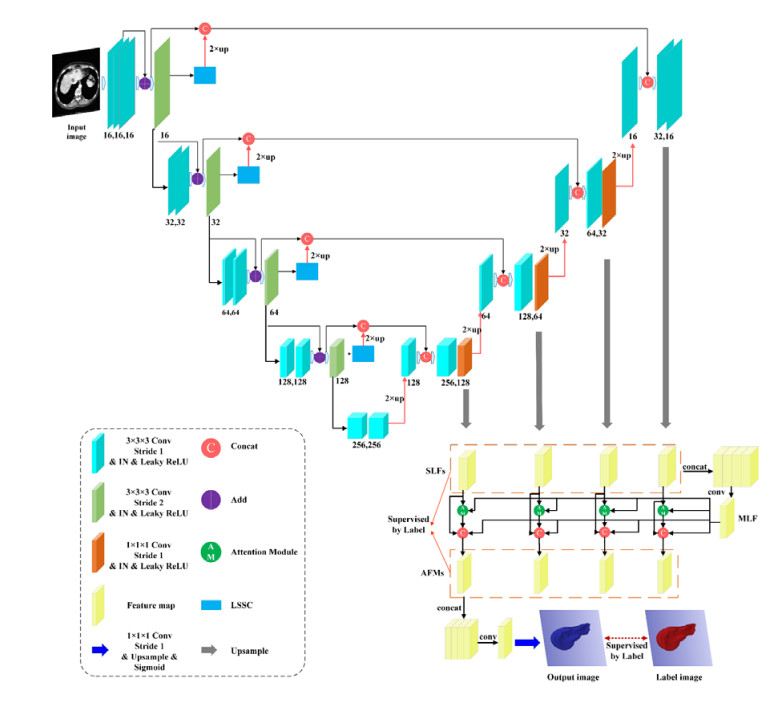
Figure 1.
The proposed MAD-UNet framework.
Citation: Hassan Shirzeh, Fazel Naghdy, Philip Ciufo, Montserrat Ros. Stochastic energy balancing in substation energy management[J]. AIMS Energy, 2015, 3(4): 810-837. doi: 10.3934/energy.2015.4.810
| [1] | Jinzhu Yang, Meihan Fu, Ying Hu . Liver vessel segmentation based on inter-scale V-Net. Mathematical Biosciences and Engineering, 2021, 18(4): 4327-4340. doi: 10.3934/mbe.2021217 |
| [2] | Jun Liu, Zhenhua Yan, Chaochao Zhou, Liren Shao, Yuanyuan Han, Yusheng Song . mfeeU-Net: A multi-scale feature extraction and enhancement U-Net for automatic liver segmentation from CT Images. Mathematical Biosciences and Engineering, 2023, 20(5): 7784-7801. doi: 10.3934/mbe.2023336 |
| [3] | Yu Li, Meilong Zhu, Guangmin Sun, Jiayang Chen, Xiaorong Zhu, Jinkui Yang . Weakly supervised training for eye fundus lesion segmentation in patients with diabetic retinopathy. Mathematical Biosciences and Engineering, 2022, 19(5): 5293-5311. doi: 10.3934/mbe.2022248 |
| [4] | Rongrong Bi, Chunlei Ji, Zhipeng Yang, Meixia Qiao, Peiqing Lv, Haiying Wang . Residual based attention-Unet combing DAC and RMP modules for automatic liver tumor segmentation in CT. Mathematical Biosciences and Engineering, 2022, 19(5): 4703-4718. doi: 10.3934/mbe.2022219 |
| [5] | Wencong Zhang, Yuxi Tao, Zhanyao Huang, Yue Li, Yingjia Chen, Tengfei Song, Xiangyuan Ma, Yaqin Zhang . Multi-phase features interaction transformer network for liver tumor segmentation and microvascular invasion assessment in contrast-enhanced CT. Mathematical Biosciences and Engineering, 2024, 21(4): 5735-5761. doi: 10.3934/mbe.2024253 |
| [6] | Zhuang Zhang, Wenjie Luo . Hierarchical volumetric transformer with comprehensive attention for medical image segmentation. Mathematical Biosciences and Engineering, 2023, 20(2): 3177-3190. doi: 10.3934/mbe.2023149 |
| [7] | Mingju Chen, Sihang Yi, Mei Yang, Zhiwen Yang, Xingyue Zhang . UNet segmentation network of COVID-19 CT images with multi-scale attention. Mathematical Biosciences and Engineering, 2023, 20(9): 16762-16785. doi: 10.3934/mbe.2023747 |
| [8] | Xiaoli Zhang, Kunmeng Liu, Kuixing Zhang, Xiang Li, Zhaocai Sun, Benzheng Wei . SAMS-Net: Fusion of attention mechanism and multi-scale features network for tumor infiltrating lymphocytes segmentation. Mathematical Biosciences and Engineering, 2023, 20(2): 2964-2979. doi: 10.3934/mbe.2023140 |
| [9] | Zhaoxuan Gong, Jing Song, Wei Guo, Ronghui Ju, Dazhe Zhao, Wenjun Tan, Wei Zhou, Guodong Zhang . Abdomen tissues segmentation from computed tomography images using deep learning and level set methods. Mathematical Biosciences and Engineering, 2022, 19(12): 14074-14085. doi: 10.3934/mbe.2022655 |
| [10] | M Nisha, T Kannan, K Sivasankari . A semi-supervised deep neuro-fuzzy iterative learning system for automatic segmentation of hippocampus brain MRI. Mathematical Biosciences and Engineering, 2024, 21(12): 7830-7853. doi: 10.3934/mbe.2024344 |
Liver segmentation from abdominal CT plays an essential role in various clinical applications. However, radiologists still predominantly perform this task in a slice-by-slice fashion, which is labor-intensive and prone to errors due to observer dependence. Therefore, automatic and accurate liver segmentation technology is highly desirable in the clinical environment.
Currently, automatic liver segmentation methods can be divided into classical machine learning-based and deep learning-based approaches. The former mainly includes thresholding [1], region growing [2], superpixel [3], level sets [4], sparse [5], atlas [6], etc. However, although machine learning-based methods significantly improved the segmentation accuracy, they still require artificial feature engineering intervention, resulting in unsatisfactory robustness.
Thanks to its remarkable feature learning ability, the deep learning-based method has attracted many scholars to the medical image process. Long et al. [7] first proposed the fully convolutional networks (FCN), which replaced the fully connected layer of VGG16 [8] with a convolutional layer. They restored the image to the original resolution through deconvolution, realizing the pixel-level prediction. Then, Ronneberger et al. [9] proposed the U-Net with a fully symmetric encoder and decoder based on FCN, which can obtain more refined results through gradual upsampling. Due to its excellent performance in medical image segmentation, scholars have successively developed various improved methods, including three categories: 1) 2D-based, 2) 3D-based, and 3) 2.5D-based methods.
The 2D-based methods require the least memory. Liu et al. [10] introduced the residual module [11] into U-Net and designed a cascaded liver segmentation model to alleviate the gradient vanishment. Xi et al. [12] proposed U-ResNets for liver and tumor segmentation. To address the imbalance issue of image category, they evaluated the model with five different loss functions. Oktay et al. [13] proposed Attention U-Net, which adds the attention gate to the skip connection of UNet. The attention gate can automatically distinguish the shape and size of the target so that the network pays more attention to the area of interest while suppressing the irrelevant area. Hong et al. [14] proposed the quartet attention UNet (QAUNet). They use quartet attention to capture the intrinsic and cross-dimensional features between channels and spatial locations. They verified the effectiveness of the network in segmenting liver and tumor through extensive experiments. Finally, Cao et al. [15] suggested a dual-attention model for liver tumor segmentation and introduced an attention gate into DenseUNet to reduce the response of irrelevant regions. In addition, the attention in the bidirectional Long Short Term Memory (LSTM) appropriately adjusts the weights of the two types of features according to their contributions to the improvement of encoding and upsampling.
For 3D-based approaches, Ji et al. [16] developed a 3D convolutional neural network (CNN) that extracts features from both spatial and temporal dimensions via 3D convolutions. Based on U-Net and 3D CNN, Cicek et al. [17] proposed 3D UNet, which replaced all 2D operations with 3D processes. Milletari et al. [18] proposed VNet. It deepened the network's depth, replaced the downsampling pooling with convolution, and achieved superior performance compared to 3D UNet. In addition, Liu et al. [19] proposed an improved 3D UNet combined with graph cutting for liver segmentation. Lei et al. [20] designed a lightweight VNet. During the training phase, they employed 3D deep supervision to improve the loss function, which showed great discriminative ability in dealing with liver and non-liver regions. Zhou et al. [21] proposed a novel memory-augmented network, the Volumetric Memory Network (VMN), for interactive segmentation of volumetric medical data. It solves the task by sequential label propagation while considering the rich 3D structures, thus avoiding costly 3D operations. Extensive experiments showed superior performance compared with a reasonable number of user interactions. Finally, Jin et al. [22] proposed a 3D hybrid residual attention-aware segmentation approach, which combines low- and high-level feature information and achieves Dice of 0.961/0.977 for liver segmentation on LiTS17/3DIRCADb datasets, respectively.
The 2.5D-based methods can significantly reduce the memory requirement by utilizing part of the inter-slice information of 3D data. Han et al. [23] developed a deep CNN that takes the stack of adjacent slices as input and generates a segmentation map corresponding to the central slice, realizing the 2.5D mode of the network. Li et al. [24] proposed H-DenseUNet based on 2D and 3D intra- and inter-slice information for liver and liver tumor segmentation. The network first extracts the image information through the 2D network. It then associates the pixel probability generated by the 2D network with the original 3D volume. Lv et al. [25] proposed a 2.5D light liver segmentation network. They leverage the techniques from the residual and Inception theories, reducing the number of parameters by 70% compared with UNet.
Nevertheless, each of the methods mentioned above cannot be used straightforwardly to generate a satisfactory result in certain challenging cases, which can be outlined as follows: (i) There are other issues around the liver or organs with similar intensity; (ii) There are multiple discrete small liver regions; (iii) The edge of the liver contains tumors.
To effectively alleviate the above issues, we developed an end-to-end 3D network framework, MAD-UNet, to aggregate multi-scale attention and combined it with deep supervision. The main contributions are summarized as follows:
 Use LSSC to avoid redundant processing of low-resolution information and improve the feature fusion of low- and high-resolution information.
Use LSSC to avoid redundant processing of low-resolution information and improve the feature fusion of low- and high-resolution information.
Employ attention mechanism to aggregate multi-scale features, making full use of the contextual spatial information at different scales.
Combine the binary cross-entropy loss with Dice loss, and apply deep supervision to the features of different levels to improve the accuracy.
Validate the proposed method on three publicly available datasets.
The rest of this paper is organized as follows. Section 2 introduces the related work; Section 3 describes the proposed network framework; Section 4 gives the experimental results and analysis in detail, and the last section provides the conclusions of this paper.
Since ordinary convolution operations often failed to highlight the target features and suppress the hidden layer's noise, the attention mechanism was proposed and found to be an effective model for alleviating such problems. For example, Squeeze-and-Excitation (SE) Block [26] could optimize the quality of representations by modeling the inter-dependencies between convolutional feature channels and thus significantly improve the performance of existing networks at a slightly increased computational cost. Woo et al. [27] developed the Convolutional Block Attention Module (CBAM). Given an intermediate feature map, the module first infers attention maps sequentially along two separate dimensions, channel and spatial. Then, the attention maps are multiplied to the input feature map for adaptive feature refinement. The CBAM can also be seamlessly integrated into any CNN architecture.
In addition, Li et al. [28] applied 3D channel attention and 3D spatial attention modules in the decoder to extract features from different scales and achieve competitive performance in spine segmentation. Zhou et al. [29] proposed a novel Motion-Attentive Transition Network (MATNet) for zero-shot video object segmentation. They designed an asymmetric attention block called Motion-Attentive Transition (MAT) in a two-stream encoder, which can convert appearance features to motion-attentive representations at each convolution stage. This design has the benefit of allowing the encoder to be deeply interleaved and to allow a tight hierarchical interaction between object motion and appearance. Wang et al. [30] adopted a multi-resolution attention module to combine local deep attention features (DAF) with global background for prostate segmentation on ultrasound images. They combined the local and global features in a simple attention module and then produced an attention map through the sigmoid function to model long-range dependencies.
Lee et al. [31] first proposed the deeply supervised network. They improve CNN's convergence speed and recognition ability in image classification by supervising the training of hidden layers. For medical image segmentation, effectively segmenting organs in volumetric images requires deep networks to extract features. However, training a deep network may cause gradient vanishment or explosion problems, resulting in ineffective backpropagation of loss.
To address this issue, Dou et al. [32] proposed to utilize direct supervision to train hidden layers in 3D FCN. They use deconvolution to upscale the low- and mid-level features and then exert a softmax function on these upscaled features to obtain ultra-dense predictions. Finally, they calculated the classification errors of the prediction results of these branches and ground truth and verified the effectiveness of deep supervision on the SLiver07 dataset. Wang et al. [33] introduced deep supervision into 3D FCNs. It effectively alleviated the gradient exploding and vanishing problem, which is commonly encountered in deep model training, thereby forcing the update process of hidden layer filters to be conducive to high-resolution features. Yang et al. [34] developed a dual-path deep supervision mechanism. One is to generate multiple predictions from multiple semantic layers and average them to produce accurate segmentation. The other is to adjust the weight of the layer by monitoring the local depth of the learned features. Their deeply supervised approach achieves good performance in lung tumor segmentation.
The proposed MAD-UNet1 network framework is shown in Figure 1. The overall framework consists of 3D UNet, multiple attention modules, and deep supervision operations. In the encoder, ordinary convolutions are replaced by residual blocks to prevent gradients vanishment. In the downsampling, to retain more feature information, convolution with a kernel size of 3 × 3 × 3 and a stride of 2 is used to replace the pooling operation. In the skip connection stage, LSSC (Figure 2) is used instead of ordinary skip connections to avoid the repetition of low-resolution feature information. In the decoder, the number of features channels before each upsampling is first halved to reduce the number of parameters. At the same time, the features of different resolutions of the decoder are upsampled to the same resolution size to form multiple SLFs (single-layer feature). Then MLFs (Multi-Layer Feature) are formed through splicing and convolution. Finally, the multi-scale fusion of MLF and SLF maps of different resolutions is used to extract regions of interest through the attention module (Figure 3), and multiple AFM (Attentive Feature Maps) are obtained. Then the liver segmentation is generated by concatenation, convolution, and the Sigmoid activation on these four AFMs. In this process, the small-scale feature maps have low resolution but a high level of semantic information. On the contrary, the large-scale feature maps have high resolution but rich details. MLFs are used to effectively deal with liver regions of different sizes and complex shapes. And four SLFs, four AFMs, and the final output image are deeply supervised.


1 Our source code is available at https://github.com/ZhangXY-123/Model/blob/master/MAD-UNet.py
The convolutional and pooling operations in U-Net can obtain deeper semantic features while reducing the image resolution. However, pooling often hinders the downward transmission of shallow features such as edges, resulting in most low-resolution semantic features being transmitted without enough edge information or small target features. Therefore, in this paper, we employed LSSC to improve this part of the problem.
In Figure 2, we detailed the LSSC modules of the transition stage between the encoder and the decoder. "Lth" represents the transition layer between the encoder and decoder, and "L-1th" is the last transition layer, while "L+1th" represents the next level of the transition layer. We use a residual module to avoid the repetition of the low-resolution feature. The residual module consists of deconvolution and an activation function. It is added after downsampling. The deconvolution of the residual path is first restored to the feature size before downsampling. Then, the obtained target features are directly passed to the decoder through skip connections. To help the network obtain edge features that are ignored in ordinary skip connections, an extra set of convolution blocks is added to each skip connection, consisting of a convolution, a batch normalization, and an activation function. Compared with ordinary skip connections, LSSC can effectively retain the edge features of the target and meanwhile avoid repeated input features.
Attention mechanisms have been applied in various image-processing tasks. For example, SENet [26] improves the representative ability of the network by establishing interdependencies between convolutional feature channels. CBAM [27] fuses channel attention and spatial attention, enabling seamless integration into any CNN network.
In the task of liver segmentation, the shallow feature map contains detailed information about the liver, and many non-liver regions as well. On the other hand, the deep feature map can obtain semantic details on the location information of the liver but may lose the points of the liver edge. To refine the information of each layer, we employed the deep attention module to generate refined features. The proposed attention module explores the effect of the hierarchical attention mechanism in liver segmentation, selectively using complementary features at all scales to refine features at different levels, thereby boosting segmentation accuracy. Its structure is shown in Figure 3.
First, the SLF and the MLF are concatenated as $ {F}_{x} $, and then the attention weight $ {W}_{x} $ is generated by 3 $ {f}_{a} $ operations,
| $ {W}_{x} = {f}_{a}({F}_{x};\theta ) $ |
where θ represents the learning parameters of $ {f}_{a} $, which contains three convolution layers consisting of two 3 × 3 × 3 convolutions and one 1 × 1 × 1 convolution. Each convolutional layer consists of one convolutional, one group normalization, and one PReLU. These convolution operations can select useful multi-level information according to the features of a single layer. The attention module computes the attentive map $ {A}_{x} $ by normalizing $ {W}_{x} $ with a Sigmoid function. Next, multiply the attention map by MLF to weigh the features in the MLF of each SLF. Finally, the weighted MLFs are merged with the corresponding features of each SLF by applying Conv + GroupNormal + PReLU again, which can automatically refine the SLF layer by layer and generate a given layer's final attention features. In this way, we can simultaneously utilize the advantages of SLFs and MLFs. Specifically, it suppresses the detailed information not in the semantically salient region, captures more details in the semantically salient region, and enhances the boundary details.
The cross-entropy loss function is commonly used for segmentation tasks since it can well retain boundary information; however, it is prone to produce significant errors when dealing with cost imbalance problems. In contrast, Dice loss has good performance for scenes with severely imbalanced positive and negative samples. Still, training loss would show instability in processing small targets. Therefore, we utilize a combination of Dice loss and binary cross-entropy loss to take into account the similarity of local details and global shapes, which are defined in Eqs (1) and (2), respectively.
| $ {L}_{BCE} = \sum _{i = 1}^{N}{g}_{i}\mathrm{log}{p}_{i}+\sum _{i = 1}^{N}(1-{g}_{i})\mathrm{log}(1-{p}_{i}) $ | (1) |
| $ {L}_{Dice} = 1-\frac{2{\sum }_{i = 1}^{N}\;{p}_{i}{g}_{i}}{{\sum }_{i = 1}^{N}\;{p}_{i}^{2}+{\sum }_{i = 1}^{N}\;{g}_{i}^{2}} $ | (2) |
where $ N $ is the voxel number of the input volume; $ {p}_{i} $∈[0.0, 1.0] represents the voxel value of the predicted probabilities; $ {g}_{i} $∈{0, 1} is the voxel value of the binary ground truth volume.
In the process of training, the supervision signal of each stage adopts the combination of $ {L}_{BCE} $ and $ {L}_{Dice} $, which are defined in Eq (3). We utilize a total of nine deep supervision signals and the $ {L}_{total} $ is defined as the sum of all signals, defined in Eq (4), in which, $ {w}^{i} $ and $ {L}_{signal}^{i} $ represent the weight and loss of the i-th layer, respectively, while $ {w}^{j} $ and $ {L}_{signal}^{j} $ represent the weight and loss of the j-th layer after the features refinement by the attention module, n represents the number of layers of the network, and $ {w}^{f} $ and $ {L}_{signal}^{f} $ denote the weight and loss of the output layer, respectively. In this paper, we empirically set the weights $ {w}^{i = \mathrm{1, 2}, \mathrm{3, 4}}, {w}^{j = \mathrm{1, 2}, \mathrm{3, 4}} $ and $ {w}^{f} $ as (0.2, 0.4, 0.6, 0.8), (0.3, 0.5, 0.7, 0.9) and 1, respectively.
| $ {L}_{signal} = {L}_{BCE}+{L}_{Dice} $ | (3) |
| $ {L}_{total} = \sum _{i = 1}^{n}{w}^{i}{L}_{signal}^{i}+\sum _{j = 1}^{n}{w}^{j}{L}_{signal}^{j}+{w}^{f}{L}_{signal}^{f} $ | (4) |
In this experiment, we choose five metrics to evaluate the performance of the proposed method, including Dice, volumetric overlap error (VOE), relative volume difference (RVD), average symmetric surface distance (ASD), and root mean square symmetric surface distance (RMSD) [35].
In addition, to validate whether the difference in segmentation accuracy between our proposed method and the comparison methods was statistically significant, we performed paired t-tests on two key metrics (Dice and ASD) with a significance level of p < 0.05. The null hypothesis is that the mean values of the same evaluation metric are the same for the compared methods.
We tested the proposed method on three public datasets: LiTS172, SLiver073, and 3DIRCADb4. For the LiTS17 dataset, we randomly select 116 sets of data for training (3:1) and 15 sets for testing. For both SLiver07 and 3DIRCADb datasets, we randomly choose 12 sets of data for training and eight groups for testing. The details of the three datasets are listed in Table 1.
| Datasets | Total train set | In-plane resolution | Inter-slice spacing | Slice num | Size |
| LiTS17 | 131 | 0.55–1.0 mm | 0.45–6.0 mm | 75–987 | 512 × 512 |
| SLiver07 | 20 | 0.5–0.8 mm | 1.0–3.0 mm | 64–394 | 512 × 512 |
| 3DIRCADb | 20 | 0.56–0.81 mm | 1.0–4.0 mm | 74–260 | 512 × 512 |
 DownLoad:
CSV
DownLoad:
CSV
2 The dataset is publicly available at https://competitions.codalab.org/competitions/17094#results
3 The dataset is publicly available at https://sliver07.grand-challenge.org
4 The dataset is publicly available at https://www.ircad.fr/research/3d-ircadb-01/
To reduce the training time and improve the computational efficiency, we set the volume of the input image to 16 × 256 × 256. Besides, to exclude irrelevant organs, we adjusted the greyscale to [-200,200] HU by windowing process, set the z-axis spacing of all data was to 1 mm and removed the slices without liver were. Finally, we expanded 20 slices to the front and back of the area containing the liver.
In addition, we chose Adam as the optimizer in the training process and combined BCE loss with Dice loss as the loss function. We set the initial learning rate to 0.001, which would update according to lr = initial_lr × γ. When the epoch reaches 400/650, the learning rate starts to decay, and the initial value of γ is set to 0.1. A total of 800 epochs were trained with a batch size of 1. We run the experiments on a workstation with Ubuntu 18.04, graphics card RTX2080Ti, RAM 32G, single CPU Intel Xeon Silver 4110, and Pytorch1.8.
To verify the effectiveness of the proposed model, we performed ablation experiments on the LiTS17 dataset. Taking 3D UNet as the baseline, we conducted qualitative comparative experiments with Baseline + LSSC, Baseline + LSSC + Multi-scale Attention (MA), Baseline + LSSC + MA + Deep Supervision (DS).
From Table 2, we can see that Baseline + LSSC achieves 0.9575 on Dice, which is 3.26% higher than the Baseline 3D UNet. By introducing a multi-scale attention module, the Dice score of Baseline + LSSC + MA achieved a 0.67% improvement (0.9642). Furthermore, our proposed MAD-UNet superimposed with deep supervision improves the Dice score by 0.85% (0.9727). Besides, the MAD-UNet also resulted in the best score on the other four evaluation metrics and thus proved the effectiveness of the proposed network.
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet (Baseline) | 92.49 ± 5.34* | 13.43 ± 9.77 | 1.05 ± 0.68 | 2.87 ± 1.43* | 8.53 ± 10.78 |
| +LSSC | 95.75 ± 1.59* | 8.26 ± 2.91 | 0.73 ± 0.58 | 1.21 ± 0.88* | 5.43 ± 4.76 |
| +LSSC+MA | 96.42 ± 1.53* | 7.56 ± 2.78 | 0.54 ± 0.31 | 1.17 ± 0.59* | 4.95 ± 5.23 |
| +LSSC+MA+DS | 97.27 ± 1.22 | 6.83 ± 2.31 | 0.34 ± 0.19 | 1.03 ± 0.37 | 3.74 ± 3.58 |
| *Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
DownLoad:
CSV
To verify the high accuracy of the proposed method, we compared the proposed method with four SOTA methods, including 3D UNet [17], VNet [18], 3D ResUNet [36], and 3D DenseUNet [24].
Figure 4 shows the Dice and Loss values of the five models during training on the LiTS17 dataset. For example, from Figure 4(a), we can see that the Dice of 3D UNet converge the slowest and has the lowest Dice value. In addition, the value of Dice of 3D ResUNet has been the highest in the first 400 epochs. However, after 400 and 650 epochs, as the learning rate decreases, its score is gradually exceeded by the proposed MAD-UNet. Finally, the proposed model outperforms the other four on Dice. In addition, during the training process, the loss of the proposed MAD-UNet (Figure 4(b)) converges in the lowest position.

Table 3 shows the comparison with the segmentation results of the SOTA methods. On the LiTS17 dataset, the Dice of the proposed method reached 0.9727, which is 4.78, 3.81, 1.84, and 2.42% higher than that of 3D UNet, VNet, 3D ResUNet, and 3D DenseUNet, respectively. The 3D UNet showed unsatisfactory results, mainly because the pooling causes the loss of image details during the downsampling. In addition, the VNet that uses convolution instead of pooling improves the accuracy by 0.97% compared to 3D UNet. Both 3D ResUNet and 3D DenseUNet using residual blocks and densely connected blocks achieve good segmentation results. Moreover, our proposed method achieves superior performance on other metrics except for RVD.
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet [17] | 92.49 ± 5.34* | 13.43 ± 9.77 | 1.05 ± 0.68 | 2.87 ± 1.43* | 8.53 ± 10.78 |
| VNet [18] | 93.46 ± 3.03* | 12.13 ± 5.23 | -0.18 ± 0.55 | 2.45 ± 1.96* | 6.45 ± 5.93 |
| 3D ResUNet [36] | 95.43 ± 2.04* | 8.57 ± 3.29 | 0.29 ± 0.37 | 1.39 ± 0.92* | 4.66 ± 4.78 |
| 3D DenseUNet [24] | 94.85 ± 2.67* | 9.42 ± 4.68 | -1.23 ± 0.75 | 1.46 ± 1.33* | 5.32 ± 4.39 |
| Our MAD-UNet | 97.27 ± 1.22 | 6.83 ± 2.31 | 0.34 ± 0.19 | 1.03 ± 0.37 | 3.74 ± 3.58 |
| *Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
DownLoad:
CSV
Figure 5 shows the segmentation results of the proposed method and other SOTA methods. (ⅰ) When segmenting liver regions with adjacent tissues (Figure 5(a)), 3D UNet, VNet, and 3D ResUNet mistakenly segmented the spleen as the liver. (ⅱ) When dealing with discontinuous liver regions (Figure 5(b)), 3D UNet and VNet showed results in under-segmentation errors, while MAD-UNet, 3D ResUNet, and 3D DenseUNet accurately segmented the liver. (ⅲ) For the liver region containing the tumor around (Figure 5(c)), the other four networks all produced significant segmentation errors. However, our proposed MAD-UNet showed a slight under-segmentation error.

Figure 6 shows the Dice and Loss curves during training on the SLiver07 dataset. Empirically we performed the learning rate decay at epoch 400, and the Dice curve of our proposed MAD-UNet showed a significant drop. However, the Dice value gradually recovered stable and was higher than other models with the epoch increase. The Loss of MAD-UNet also fluctuated in the first 400 epochs of training and then gradually stabilized and was lower than other models.

As shown in Table 4, on the SLiver07 dataset, our method achieves the best scores on all five-evaluation metrics. For example, the Dice of MAD-UNet is 4.72, 2.44, 1.5, and 1.19% higher than that of the other four methods, respectively. Besides, our proposed MAD-UNet also showed superior performance on the other four evaluation metrics and thus proved high accuracy and good robustness.
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet [17] | 92.80 ± 4.13* | 13.20 ± 2.85 | 1.26 ± 0.45 | 9.93 ± 5.86* | 18.51 ± 14.83 |
| VNet [18] | 95.08 ± 4.33* | 9.12 ± 7.41 | -0.93 ± 0.32 | 3.28 ± 5.12* | 7.67 ± 11.06 |
| 3D ResUNet [36] | 96.02 ± 2.54* | 7.55 ± 4.53 | -0.66 ± 0.19 | 2.84 ± 2.56* | 9.33 ± 9.43 |
| 3D DenseUNet [24] | 96.33 ± 1.52* | 7.03 ± 2.81 | 0.58 ± 0.16 | 3.50 ± 2.67* | 12.55 ± 10.79 |
| MAD-UNet | 97.52 ± 0.81 | 4.97 ± 1.73 | 0.23 ± 0.17 | 1.13 ± 0.82 | 4.73 ± 5.21 |
| Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
DownLoad:
CSV
Figure 7 provides the visual segmentation results of different methods on the SLiver07 dataset. (ⅰ) When the liver region containing adjacent tissues (Figure 7(a)), 3D UNet, VNet, and 3D ResUNet showed obvious over-segmentation errors; on the contrary, our proposed method and 3D DenseUNet obtained comparable results to the ground truth. (ⅱ) When dealing with the liver CT intensity similar to that of other organs (e.g., spleen, Figure 7(b)), both 3D UNet and VNet showed significant over-segmentation errors. However, our method achieves the highest segmentation accuracy. (ⅲ) For liver with discontinuous regions (Figure 7(c)), MAD-UNet results in the slightest segmentation error compared with other methods.

Figure 8 provides the Dice and Loss curves for different models during training on the 3DIRCADb dataset. It can be seen that the Dice of MAD-UNet converges to the highest. Besides, its Loss is always located at the lowest position among all the models.

As shown in Table 5, on the 3DIRCADb dataset, the effect of 3D UNet results in the worst Dice score (0.8988), while our proposed method obtains Dice of 0.9691. Moreover, our proposed MAD-UNet achieves the best segmentation results on other metrics except for slight inferiority to 3D ResUNet on RVD.
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet [17] | 89.88 ± 11.42* | 16.95 ± 15.82 | 2.63 ± 0.98 | 7.21 ± 6.74* | 10.24 ± 9.27 |
| VNet [18] | 92.47 ± 5.34* | 13.62 ± 8.67 | 1.05 ± 0.68 | 4.06 ± 3.30* | 7.41 ± 6.43 |
| 3D ResUNet [36] | 94.61 ± 2.08* | 10.16 ± 3.73 | -0.18 ± 0.29 | 2.27 ± 1.08* | 4.93 ± 3.87 |
| 3D DenseUNet [24] | 94.56 ± 2.23* | 10.25 ± 3.99 | 1.23 ± 0.75 | 3.23 ± 1.96* | 5.81 ± 4.63 |
| MAD-UNet | 96.91 ± 0.68 | 5.64 ± 1.96 | 0.25 ± 0.43 | 1.08 ± 0.77 | 2.33 ± 1.15 |
| *Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
DownLoad:
CSV
Figure 9 demonstrates some typical results on the 3DIRCADb dataset. (i) Figure 9(a) presents a segmentation comparison when dealing with discontinuous liver regions that contain tumors at the edges. It can be seen that all five methods result in some over-segmentation in the fuzzy connecting area of the liver regions. Still, the MAD-UNet showed a relatively more minor error (ii) Figure 9(b) and Figure 9(c) give the segmentation comparison when the liver region contains adjacent organs or tissues. It can be seen that MAD-UNet and 3D DenseUNet achieved relatively stable and high-precision segmentation accuracy.

Table 6 lists the parameters, training, and test time of different methods on LiTS17, SLiver07, and 3DIRCADb datasets. As can be seen from the table, 3D UNet requires the smallest amount of parameters, VNet requires the largest, while deploying the proposed MAD-UNet needs slightly more parameters than 3D UNet and 3D ResUNet. Furthermore, on all three datasets, the training time of 3D UNet is the least, while that of 3D DenseUNet is the most. Specifically, our proposed method requires the least time to test the three datasets.
| Method | Parameters | LiTS17 | SLiver07 | 3DIRCADb | |||
| Train time | Test time | Train time | Test time | Train time | Test time | ||
| 3D UNet [17] | 6,405,827 | 79h58m4s | 51.54 s | 25h21m12s | 20.42 s | 17h56m51s | 16.71 s |
| VNet [18] | 53,782,217 | 119h50m21s | 52.46 s | 38h4m52s | 19.63 s | 26h48m38s | 15.74 s |
| 3D ResUNet [36] | 9,498,195 | 81h24m18m | 52.01 s | 25h46m45s | 18.75 s | 18h7m53s | 14.42 s |
| 3D DenseUNet [24] | 19,783,361 | 150h19m15s | 58.21 s | 47h22m43s | 19.39 s | 33h27m43m | 17.89 s |
| MAD-UNet | 9,990,960 | 85h54m59s | 49.68 s | 27h16m23s | 18.55 s | 19h31m51s | 13.72 s |
DownLoad:
CSV
To illustrate the proposed method's limitation, we present the visualizations of 2D and 3D segmentation errors in some typical cases of the proposed MAD-UNet in Figure 10. (ⅰ) From Figure 10(a), we can see that MAD-UNet showed obvious over-segmentation errors in liver regions containing blood vessels. The main reason is that the boundary between the liver and surrounding organs and tissues is blurred in this case. (ⅱ) As shown in Figure 10(b), MAD-UNet produces obvious over-segmentation errors when processing liver regions with large tumors at the edges. This is because the grayscale difference between the tumor and the liver may cause the tumor located at the edge of the liver to be considered as other organs or tissues, resulting in segmentation errors. To alleviate this limitation, we would focus more on strategies to address blurred boundaries, e.g., Zhang et al. [37] effectively suppressed the inconsistency of data distribution by removing mean energy in the preprocessing stage.

This paper proposes a new framework by aggregating multi-scale attention and combining it with deep supervision. We aim to improve the liver segmentation accuracy from CT by the proposal of (ⅰ) the residual and skip connections, which avoid the repetition of low-resolution feature information and can effectively preserve the edge information of the target. (ⅱ) the attention module, which fully aggregates feature information of different scales and dimensions. It guides the refined attention module to filter out noisy areas, helping the network to pay more attention to areas of interest. (ⅲ) the deep supervision signals, which are used to improve the network's learning ability at different levels.
We extensively validated the proposed method on three publicly available datasets. The experimental results demonstrated that: 1) Compared with the existing SOTA models, our method achieves the best results in four evaluation metrics (Dice, VOE, ASD, and RMSD), with the least test time. 2) The proposed MAD-UNet obtains more satisfactory segmentation performance in dealing with cases, including (i) discontinuous liver regions and (ii) livers containing adjacent tissues or organs.
Nevertheless, the proposed method still shows certain limitations when processing the liver with blood vessels around or containing large tumors at the liver edge. Moreover, the 3D mode requires large memory. Therefore, we will focus on optimizing the network composition to improve the accuracy and robustness of the proposed method via more effective learning of edge features information.
This work is supported by the National Nature Science Foundation (No. 61741106, 61701178). This article does not contain any studies with live human participants or animals performed by any of the authors.
The authors declare that they have no conflict of interest.
| [1] | Clean Energy Regulator, 2014. Available from: http://www.cleanenergycouncil. org.au/policy-advocacy/reports/clean-energy-australia-report.html. |
| [2] |
Liu X (2010) Economic load dispatch constrained by wind power availability: A wait-and- see approach. Smart Grid, IEEE Transactions on 1: 347-355. doi: 10.1109/TSG.2010.2057458

|
| [3] |
Parvania M, Fotuhi-Firuzabad M (2010) Demand response scheduling by stochastic SCUC. Smart Grid, IEEE Transactions on 1: 89-98. doi: 10.1109/TSG.2010.2046430
|
| [4] |
Gong C,Wang X, Xu W, et al. (2013) Distributed real-time energy scheduling in smart grid: Stochastic model and fast optimization. Smart Grid, IEEE Transactions on 4: 1476-1489. doi: 10.1109/TSG.2013.2248399
|
| [5] |
Su S, Lu C, Chang R, et al. (2011) Distributed generation interconnection planning: A wind power case study. Smart Grid, IEEE Transactions on 2: 181-189. doi: 10.1109/TSG.2011.2105895
|
| [6] |
He M, Murugesan S, Zhang J (2013) A multi-timescale scheduling approach for stochastic reliability in smart grids with wind generation and opportunistic demand. Smart Grid, IEEE Transactions on 4: 521-529. doi: 10.1109/TSG.2012.2237421
|
| [7] | Mohd A, Ortjohann E, Schmelter A, et al. (2008) Challenges in integrating distributed energy storage systems into future smart grid. Industrial Electronics. ISIE 2008. IEEE International Symposium on: 1627-1632. |
| [8] | Dantzig G (1998) Linear Programming and Extensions, Princeton university Press. |
| [9] |
Nfaoui H, Essiarab H, Sayigh A (2004) A stochastic Markov chain model for simulating wind speed time series at Tangiers, Morocco. Renewable Energy 29: 1407-1418. doi: 10.1016/S0960-1481(03)00143-5
|
| [10] |
Hocaoglu F (2011) Stochastic approach for daily solar radiation modeling. Solar Energy 85: 278-287. doi: 10.1016/j.solener.2010.12.003
|
| [11] | Chen P, Pedersen T, Bak-Jensen B, et al. (2010) ARIMA-based time series model of stochastic wind power generation. Power Systems, IEEE Transactions on 25: 667-676. |
| [12] | Box G, Jenkins M, Reinsel G (2008) Time Series Analysis, Forecasting and Control, John Wiley & Sons Inc. |
| [13] |
Bivona S, Bonanno G, Burlon r, et al. (2011) Stochastic models for wind speed forecasting. Energy Conversion and Management 52: 1157-1165. doi: 10.1016/j.enconman.2010.09.010
|
| [14] | A Case Study of Increasing Levels of PV Penetration in an Isolated Electricity Supply Sys- tem, 2014. Available from: http://apvi.org.au/wp-content/uploads/2014/05/Carnarvon- High-PV-Penetration-Case-Study.pdf. |
| [15] |
Nguyen C, Flueck A (2012) Agent based restoration with distributed energy storage support in smart grids. Smart Grid, IEEE Transactions on 3: 1029-1038. doi: 10.1109/TSG.2012.2186833
|
| [16] |
Kodama J, Hamagami T, Shinji H, et al. (2009) Multi-agent-based autonomous power distribution network restoration using contract net protocol. Electrical Engineering in Japan 166: 56-63. doi: 10.1002/eej.20661
|
| [17] |
Lu B, Shahidehpour M (2005) Short-term scheduling of battery in a grid-connected PV/battery system. Power Systems, IEEE Transactions on 20: 1053-1061. doi: 10.1109/TPWRS.2005.846060
|
| [18] | Sortomme E, El-Sharkawi M, (2009) Optimal Power Flow for a System of Microgrids with Controllable Loads and Battery Storage. Power Systems Conference and Exposition, 2009 : 1-5. |
| [19] |
Zong Y, Kullmann D, Thavlov A, et al. (2012) Application of model predictive control for active load management in a distributed power system with high wind penetration. Smart Grid, IEEE Transactions on 3: 1055-1062. doi: 10.1109/TSG.2011.2177282
|
| [20] | Zhao Z, Wu L (2013) Impacts of high penetration wind generation and demand response on LMPs in day-ahead market. Smart Grid, IEEE Transactions on 5: 220-229. |
| [21] |
Li Y, Huang G, Xu Y, et al. (2010) Regional-scale electric power system planning under uncertainty a multistage interval-stochastic integer linear programming approach. Energy Policy 38: 475-490. doi: 10.1016/j.enpol.2009.09.038
|
| [22] |
Molderink A, Bakker V, Bosman M, et al. (2010) Management and control of domestic smart grid technology. Smart Grid, IEEE Transactions on 1: 109-119. doi: 10.1109/TSG.2010.2055904
|
| [23] |
Yu W, Liu D, Huang Y (2013) Operation Optimization Based on the Power Supply and Storage Capacity of an Active Distribution Network. Energies 6: 6423-6438. doi: 10.3390/en6126423
|
| [24] | McArthur S, Davidson E, Catterson V, et al. Multi-agent systems for power engineering applications, part ii: Technologies, standards, and tools for building multi-agent systems. Power Systems, IEEE Transactions on 22: 1753-1759. |
| [25] |
Moslehi K, Kumar R (2010) A reliability perspective of the smart grid. Smart Grid, IEEE Transactions on 1: 57-64. doi: 10.1109/TSG.2010.2046346
|
| [26] |
Garciaa-Ascanio C, Mate C (2010) Electric power demand forecasting using interval time series: A comparison between VAR and iMLP. Energy Policy 38: 715-725. doi: 10.1016/j.enpol.2009.10.007
|
| [27] |
Shirzeh H, Naghdy F, Ciufo P, et al. (2015) Balancing energy in the smart grid using distributed value function (DVF). Smart Grid, IEEE Transactions on 6: 808-818. doi: 10.1109/TSG.2014.2363844
|
| [28] | Pawlowski A, Guzman J, Rodriguez F, et al. (2010) Application of time-series methods to disturbance estimation in predictive control problems. in Industrial Electronics (ISIE), 2010 IEEE International Symposium on: 409-414. |
| [29] |
Taylor J, Menezes L, McSharry P (2006) A comparison of univariate methods for forecasting electricity demand up to a day ahead. International Journal of Forecasting 22: 1-16. doi: 10.1016/j.ijforecast.2005.06.006
|
| [30] | Munoz A, Sanchez-Ubeda E, Cruz A, et al. (2010) Short-term forecasting in power systems: A guided tour, Handbook of Power Systems II, Energy Systems, Springer Berlin Heidelberg, 129-160. |
| [31] | Pring M (2002) Technical Analysis Explained, McGraw-Hill, 2002. |
| [32] | Murphy J (1999) Technical Analysis of the Financial Markets, New York Institute of Finance. |
| [33] | Mooney C (1997) Monte Carlo Simulation, SAGE PUBLICATION. |
| [34] |
Nguyen M, Nguyen D, Yoon Y (2012) A New Battery Energy Storage Charging/Discharging Scheme for Wind Power Producers in Real-Time Markets. Energies, 5: 5439-5452. doi: 10.3390/en5125439
|
| [35] | Endeavor Energy, 2013. Available from: www.endeavourenergy.com.au/. |
| [36] | Bellifemine F, Caire G, Greenwood D (2007) Developing Multi Agent Systems with JADE, England: Wiley. |
| [37] | Department of Agriculture and Food, WA, Australia, 2014. Available from: https://www.agric.wa.gov.au/. |
| [38] | University of York, 2009. Available from: http://www.agentcontrol.co.uk/. |
| [39] | Robinson C, MendhamP, Clarke T (2010) MACSIMJX: A Tool for Enabling Agent Mod- elling with Simulink Using JADE. JoPha Journal of Pysical Agents 4: 1-7. |
| [40] | Shull F, Singer J, Sjoberg D (2008) Guide to advanced empirical software engineering, Springer. |
| 1. | Jun Liu, Zhenhua Yan, Chaochao Zhou, Liren Shao, Yuanyuan Han, Yusheng Song, mfeeU-Net: A multi-scale feature extraction and enhancement U-Net for automatic liver segmentation from CT Images, 2023, 20, 1551-0018, 7784, 10.3934/mbe.2023336 | |
| 2. | Desire Burume Mulindwa, Shengzhi Du, An n-Sigmoid Activation Function to Improve the Squeeze-and-Excitation for 2D and 3D Deep Networks, 2023, 12, 2079-9292, 911, 10.3390/electronics12040911 | |
| 3. | Shengwei Li, Xiao‐Guang Li, Fanyu Zhou, Yumeng Zhang, Zhixin Bie, Lin Cheng, Jinzhao Peng, Bin Li, Automated segmentation of liver and hepatic vessels on portal venous phase computed tomography images using a deep learning algorithm, 2024, 25, 1526-9914, 10.1002/acm2.14397 | |
| 4. | Yuriy A. Vasilev, Anton V. Vladzymyrskyy, Kirill M. Arzamasov, David U. Shikhmuradov, Andrey V. Pankratov, Iliya V. Ulyanov, Nikolay B. Nechaev, Prospects of using computer vision technology to detect urinary stones and liver and kidney neoplasms on computed tomography images of the abdomen and retroperitoneal space, 2024, 5, 2712-8962, 101, 10.17816/DD515814 | |
| 5. | Yanzhen Liu, Sutuke Yibulayimu, Yudi Sang, Gang Zhu, Yu Wang, Chunpeng Zhao, Xinbao Wu, 2023, Chapter 30, 978-3-031-43995-7, 312, 10.1007/978-3-031-43996-4_30 | |
| 6. | Di Wei, Yundan Jiang, Xuhui Zhou, Di Wu, Xiaorong Feng, A Review of Advancements and Challenges in Liver Segmentation, 2024, 10, 2313-433X, 202, 10.3390/jimaging10080202 | |
| 7. | Lulu Wang, Mostafa Fatemi, Azra Alizad, Artificial intelligence techniques in liver cancer, 2024, 14, 2234-943X, 10.3389/fonc.2024.1415859 | |
| 8. | Li Liu, Kaijian Xia, BTIS-Net: Efficient 3D U-Net for Brain Tumor Image Segmentation, 2024, 12, 2169-3536, 133392, 10.1109/ACCESS.2024.3460797 | |
| 9. | Yanzhen Liu, Sutuke Yibulayimu, Yudi Sang, Gang Zhu, Chao Shi, Chendi Liang, Qiyong Cao, Chunpeng Zhao, Xinbao Wu, Yu Wang, Preoperative fracture reduction planning for image-guided pelvic trauma surgery: A comprehensive pipeline with learning, 2025, 13618415, 103506, 10.1016/j.media.2025.103506 | |
| 10. | Yanzhen Liu, Sutuke Yibulayimu, Gang Zhu, Chao Shi, Chendi Liang, Chunpeng Zhao, Xinbao Wu, Yudi Sang, Yu Wang, Automatic pelvic fracture segmentation: a deep learning approach and benchmark dataset, 2025, 12, 2296-858X, 10.3389/fmed.2025.1511487 | |
| 11. | Rahman Maqsood, Fazeel Abid, Jawad Rasheed, Onur Osman, Shtwai Alsubai, Optimal Res-UNET architecture with deep supervision for tumor segmentation, 2025, 12, 2296-858X, 10.3389/fmed.2025.1593016 |




Figures(16) / Tables(3)

Hassan Shirzeh, Fazel Naghdy, Philip Ciufo, Montserrat Ros. Stochastic energy balancing in substation energy management[J]. AIMS Energy, 2015, 3(4): 810-837. doi: 10.3934/energy.2015.4.810

| Datasets | Total train set | In-plane resolution | Inter-slice spacing | Slice num | Size |
| LiTS17 | 131 | 0.55–1.0 mm | 0.45–6.0 mm | 75–987 | 512 × 512 |
| SLiver07 | 20 | 0.5–0.8 mm | 1.0–3.0 mm | 64–394 | 512 × 512 |
| 3DIRCADb | 20 | 0.56–0.81 mm | 1.0–4.0 mm | 74–260 | 512 × 512 |
DownLoad:
CSV
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet (Baseline) | 92.49 ± 5.34* | 13.43 ± 9.77 | 1.05 ± 0.68 | 2.87 ± 1.43* | 8.53 ± 10.78 |
| +LSSC | 95.75 ± 1.59* | 8.26 ± 2.91 | 0.73 ± 0.58 | 1.21 ± 0.88* | 5.43 ± 4.76 |
| +LSSC+MA | 96.42 ± 1.53* | 7.56 ± 2.78 | 0.54 ± 0.31 | 1.17 ± 0.59* | 4.95 ± 5.23 |
| +LSSC+MA+DS | 97.27 ± 1.22 | 6.83 ± 2.31 | 0.34 ± 0.19 | 1.03 ± 0.37 | 3.74 ± 3.58 |
| *Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
DownLoad:
CSV
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet [17] | 92.49 ± 5.34* | 13.43 ± 9.77 | 1.05 ± 0.68 | 2.87 ± 1.43* | 8.53 ± 10.78 |
| VNet [18] | 93.46 ± 3.03* | 12.13 ± 5.23 | -0.18 ± 0.55 | 2.45 ± 1.96* | 6.45 ± 5.93 |
| 3D ResUNet [36] | 95.43 ± 2.04* | 8.57 ± 3.29 | 0.29 ± 0.37 | 1.39 ± 0.92* | 4.66 ± 4.78 |
| 3D DenseUNet [24] | 94.85 ± 2.67* | 9.42 ± 4.68 | -1.23 ± 0.75 | 1.46 ± 1.33* | 5.32 ± 4.39 |
| Our MAD-UNet | 97.27 ± 1.22 | 6.83 ± 2.31 | 0.34 ± 0.19 | 1.03 ± 0.37 | 3.74 ± 3.58 |
| *Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
DownLoad:
CSV
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet [17] | 92.80 ± 4.13* | 13.20 ± 2.85 | 1.26 ± 0.45 | 9.93 ± 5.86* | 18.51 ± 14.83 |
| VNet [18] | 95.08 ± 4.33* | 9.12 ± 7.41 | -0.93 ± 0.32 | 3.28 ± 5.12* | 7.67 ± 11.06 |
| 3D ResUNet [36] | 96.02 ± 2.54* | 7.55 ± 4.53 | -0.66 ± 0.19 | 2.84 ± 2.56* | 9.33 ± 9.43 |
| 3D DenseUNet [24] | 96.33 ± 1.52* | 7.03 ± 2.81 | 0.58 ± 0.16 | 3.50 ± 2.67* | 12.55 ± 10.79 |
| MAD-UNet | 97.52 ± 0.81 | 4.97 ± 1.73 | 0.23 ± 0.17 | 1.13 ± 0.82 | 4.73 ± 5.21 |
| Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
DownLoad:
CSV
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet [17] | 89.88 ± 11.42* | 16.95 ± 15.82 | 2.63 ± 0.98 | 7.21 ± 6.74* | 10.24 ± 9.27 |
| VNet [18] | 92.47 ± 5.34* | 13.62 ± 8.67 | 1.05 ± 0.68 | 4.06 ± 3.30* | 7.41 ± 6.43 |
| 3D ResUNet [36] | 94.61 ± 2.08* | 10.16 ± 3.73 | -0.18 ± 0.29 | 2.27 ± 1.08* | 4.93 ± 3.87 |
| 3D DenseUNet [24] | 94.56 ± 2.23* | 10.25 ± 3.99 | 1.23 ± 0.75 | 3.23 ± 1.96* | 5.81 ± 4.63 |
| MAD-UNet | 96.91 ± 0.68 | 5.64 ± 1.96 | 0.25 ± 0.43 | 1.08 ± 0.77 | 2.33 ± 1.15 |
| *Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
DownLoad:
CSV
| Method | Parameters | LiTS17 | SLiver07 | 3DIRCADb | |||
| Train time | Test time | Train time | Test time | Train time | Test time | ||
| 3D UNet [17] | 6,405,827 | 79h58m4s | 51.54 s | 25h21m12s | 20.42 s | 17h56m51s | 16.71 s |
| VNet [18] | 53,782,217 | 119h50m21s | 52.46 s | 38h4m52s | 19.63 s | 26h48m38s | 15.74 s |
| 3D ResUNet [36] | 9,498,195 | 81h24m18m | 52.01 s | 25h46m45s | 18.75 s | 18h7m53s | 14.42 s |
| 3D DenseUNet [24] | 19,783,361 | 150h19m15s | 58.21 s | 47h22m43s | 19.39 s | 33h27m43m | 17.89 s |
| MAD-UNet | 9,990,960 | 85h54m59s | 49.68 s | 27h16m23s | 18.55 s | 19h31m51s | 13.72 s |
DownLoad:
CSV
| Datasets | Total train set | In-plane resolution | Inter-slice spacing | Slice num | Size |
| LiTS17 | 131 | 0.55–1.0 mm | 0.45–6.0 mm | 75–987 | 512 × 512 |
| SLiver07 | 20 | 0.5–0.8 mm | 1.0–3.0 mm | 64–394 | 512 × 512 |
| 3DIRCADb | 20 | 0.56–0.81 mm | 1.0–4.0 mm | 74–260 | 512 × 512 |
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet (Baseline) | 92.49 ± 5.34* | 13.43 ± 9.77 | 1.05 ± 0.68 | 2.87 ± 1.43* | 8.53 ± 10.78 |
| +LSSC | 95.75 ± 1.59* | 8.26 ± 2.91 | 0.73 ± 0.58 | 1.21 ± 0.88* | 5.43 ± 4.76 |
| +LSSC+MA | 96.42 ± 1.53* | 7.56 ± 2.78 | 0.54 ± 0.31 | 1.17 ± 0.59* | 4.95 ± 5.23 |
| +LSSC+MA+DS | 97.27 ± 1.22 | 6.83 ± 2.31 | 0.34 ± 0.19 | 1.03 ± 0.37 | 3.74 ± 3.58 |
| *Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet [17] | 92.49 ± 5.34* | 13.43 ± 9.77 | 1.05 ± 0.68 | 2.87 ± 1.43* | 8.53 ± 10.78 |
| VNet [18] | 93.46 ± 3.03* | 12.13 ± 5.23 | -0.18 ± 0.55 | 2.45 ± 1.96* | 6.45 ± 5.93 |
| 3D ResUNet [36] | 95.43 ± 2.04* | 8.57 ± 3.29 | 0.29 ± 0.37 | 1.39 ± 0.92* | 4.66 ± 4.78 |
| 3D DenseUNet [24] | 94.85 ± 2.67* | 9.42 ± 4.68 | -1.23 ± 0.75 | 1.46 ± 1.33* | 5.32 ± 4.39 |
| Our MAD-UNet | 97.27 ± 1.22 | 6.83 ± 2.31 | 0.34 ± 0.19 | 1.03 ± 0.37 | 3.74 ± 3.58 |
| *Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet [17] | 92.80 ± 4.13* | 13.20 ± 2.85 | 1.26 ± 0.45 | 9.93 ± 5.86* | 18.51 ± 14.83 |
| VNet [18] | 95.08 ± 4.33* | 9.12 ± 7.41 | -0.93 ± 0.32 | 3.28 ± 5.12* | 7.67 ± 11.06 |
| 3D ResUNet [36] | 96.02 ± 2.54* | 7.55 ± 4.53 | -0.66 ± 0.19 | 2.84 ± 2.56* | 9.33 ± 9.43 |
| 3D DenseUNet [24] | 96.33 ± 1.52* | 7.03 ± 2.81 | 0.58 ± 0.16 | 3.50 ± 2.67* | 12.55 ± 10.79 |
| MAD-UNet | 97.52 ± 0.81 | 4.97 ± 1.73 | 0.23 ± 0.17 | 1.13 ± 0.82 | 4.73 ± 5.21 |
| Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
| Method | Dice (%) | VOE (%) | RVD (%) | ASD (mm) | RMSD (mm) |
| 3D UNet [17] | 89.88 ± 11.42* | 16.95 ± 15.82 | 2.63 ± 0.98 | 7.21 ± 6.74* | 10.24 ± 9.27 |
| VNet [18] | 92.47 ± 5.34* | 13.62 ± 8.67 | 1.05 ± 0.68 | 4.06 ± 3.30* | 7.41 ± 6.43 |
| 3D ResUNet [36] | 94.61 ± 2.08* | 10.16 ± 3.73 | -0.18 ± 0.29 | 2.27 ± 1.08* | 4.93 ± 3.87 |
| 3D DenseUNet [24] | 94.56 ± 2.23* | 10.25 ± 3.99 | 1.23 ± 0.75 | 3.23 ± 1.96* | 5.81 ± 4.63 |
| MAD-UNet | 96.91 ± 0.68 | 5.64 ± 1.96 | 0.25 ± 0.43 | 1.08 ± 0.77 | 2.33 ± 1.15 |
| *Note: Bold font represents the best results. * indicates a statistically significant difference between the labeled results and the corresponding results of our method at a significance level of 0.05. | |||||
| Method | Parameters | LiTS17 | SLiver07 | 3DIRCADb | |||
| Train time | Test time | Train time | Test time | Train time | Test time | ||
| 3D UNet [17] | 6,405,827 | 79h58m4s | 51.54 s | 25h21m12s | 20.42 s | 17h56m51s | 16.71 s |
| VNet [18] | 53,782,217 | 119h50m21s | 52.46 s | 38h4m52s | 19.63 s | 26h48m38s | 15.74 s |
| 3D ResUNet [36] | 9,498,195 | 81h24m18m | 52.01 s | 25h46m45s | 18.75 s | 18h7m53s | 14.42 s |
| 3D DenseUNet [24] | 19,783,361 | 150h19m15s | 58.21 s | 47h22m43s | 19.39 s | 33h27m43m | 17.89 s |
| MAD-UNet | 9,990,960 | 85h54m59s | 49.68 s | 27h16m23s | 18.55 s | 19h31m51s | 13.72 s |
