Citation: Pedro Neves, Morten Gleditsch, Cindy Bennet, Mathias Craig, Jon Sumanik-Leary. Assessment of locally manufactured small wind turbines as an appropriate technology for the electrification of the Caribbean Coast of Nicaragua[J]. AIMS Energy, 2015, 3(1): 41-74. doi: 10.3934/energy.2015.1.41

| [1] | Practical Action (2014) Poor People's Energy Outlook 2014: Key messages on energy for poverty alleviation, Practical Action Publishing. |
| [2] |
Yadoo A, Cruickshank H. (2012) The role for low carbon electrification technologies in poverty reduction and climate change strategies: A focus on renewable energy mini-grids with case studies in Nepal, Peru and Kenya. Energy Policy 42: 591-603. doi: 10.1016/j.enpol.2011.12.029

|
| [3] | SE4All (2014) High Impact Opportunity: Clean Energy Mini-Grids, 1-20, SE4All. |
| [4] | IEA (2014) World Energy Outlook 2014. Available from: www.iea.org. |
| [5] |
Domenech B, Ferrer-Martí L, Lillo P, et al. (2014) A community electrification project: Combination of microgrids and household systems fed by wind, PV or micro-hydro energies according to micro-scale resource evaluation and social constraints. Energy for Sustainable Development 23: 275-285. doi: 10.1016/j.esd.2014.09.007
|
| [6] | Xiliang Z, Gan L, Shuhua G, et al. (1999) Wind energy technology development and diffusion: A case study of Inner Mongolia, China, Center for International Climate and Environmental Research (Oslo, Norway) and Institute for Techno-economics and Energy Systems Analysis (Tsinghua University, Beijing, China). |
| [7] | Bachelor S, Scott N, Daoqi L, et al. (1999) Evaluating the impact of wind generators in Inner Mongolia: Project Technical Report, Gamos Ltd, DfID. |
| [8] |
Mishnaevsky Jr. L, Freere P, Sinha, et al. (2011) Small wind turbines with timber blades for developing countries: Materials choice, development, installation and experiences. Renewable Energy 36: 2128-2138. doi: 10.1016/j.renene.2011.01.034
|
| [9] |
Ferrer-Martí L, Garwood A, Chiroque J, et al. (2012) Evaluating and comparing three community small-scale wind electrification projects. Renew Sustain Energy Rev 16: 5379-5390. doi: 10.1016/j.rser.2012.04.015
|
| [10] | Leary J, While A, Howell R (2012) Locally manufactured wind power technology for sustainable rural electrification. Energy Policy 43-0: 173-183. |
| [11] | Sumanik-Leary J, While A, Howell R (2013) Small wind turbines for decentralised rural electrification: case studies in Peru, Nicaragua and Scotland, PhD Thesis, University of Sheffield. |
| [12] | Khennas S, Dunnett S, Piggott H (2008) Small Wind Systems for Rural Energy Services, Practical Action Publishing. |
| [13] | Piggot H (2013) A wind Turbine Recipe Book, Scoraig Wind Electric |
| [14] | Batrmann D, Fink D (2008) Homebrew Wind Power, Buckville Publications LLC. |
| [15] | Joulain C et al (2009) 12' Turbine final design pre-report, blueEnergy internal document. |
| [16] | HOMER (2009) National Renewable Energy Laboratory. Available from: www.nrel.gov. |
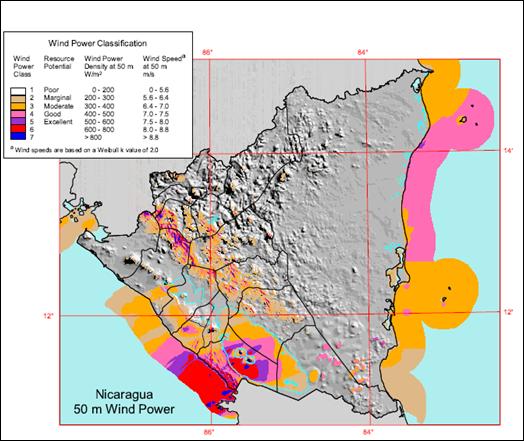
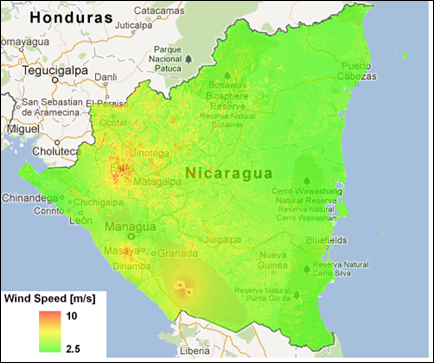
| [17] | National Renewable Energy Laboratory (2005) Wind Atlas of Nicaragua. Available from: http://www.nrel.gov/wind/pdfs/nicaragua.pdf. |
| [18] | Meteotest (www.meteotest.ch) (2005) Wind Map of Nicaragua. |
| [19] | Marandin L (2004) Etude du gisement éolien du site de Bluefields et réalisation d'un project pilote de production d'énergie électrique éolienne, SupAero, MsC Thesis. |
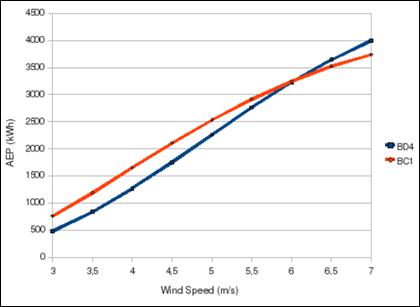
| [20] | C. Joulain et al (2009) bC1 pre-report, blueEnergy internal document. |
| [21] |
Ferrer-Martí L, Garwood A, Chiroque J, et al. (2010) A Community Small-Scale Wind Generation Project in Peru. Wind Engineering 34: 277-288. doi: 10.1260/0309-524X.34.3.277
|
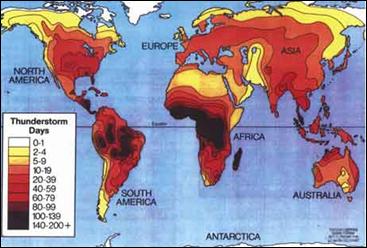
| [22] | National Lightning Safety Institute (2009) Lightening Protection for Engineers, 6 Eds., National Lightning Safety Institute. |
| [23] | NRG Systems (2011) NRG 60m and 50 m XHD Tall Tower Installation Manual & Specifications, NRG Systems. Available from: http://www.nrgsystems.com/FileLibrary/fdbaaba20b7f4542b8a9f95aea6aa617/NRG%2060m%20and%2050m%20XHD%20TallTower%20Installation%20Manual%20-%20Rev%203.0.pdf. |
| [24] | Sumanik-Leary J, Marandin L, Craig M, et al. (2013) Participatory Manufacture of Small Wind Turbines: A Case Study in Nicaragua, 2013. Available from: www.windempowerment.org. |
| [25] | Quéval L, Joulain C, Casillas CE (2014) Measuring the Power Curve of a Small-Scale Wind Turbine: A Practical Example in Proceedings of the 1st Int. e-Conf. on Energies 14-31 March 2014, Sciforum Electronic Conference Series Vol. 1. Available from: www.sciforum.net/conference/ece-1/paper/2338/download/pdf |
| [26] | ESMAP (2013) Technical and Economic Assessment of Off-Grid, Mini-Grid and Grid Electrification Technologies, ESMAP. Available from: http://www.esmap.org/sites/esmap.org/files/Technical%20and%20Economic%20Assessment%20of%20Off-grid,%20Minigrid%20and%20Grid%20Electrification%20Technologies_Report%2012107.pdf |
| [27] | IRENA (2012) SolarPower. Renewable Energy Technologies: Cost Analysis Series. Abu Dhabi, International Renewable Energy Agency. |
| [28] | SuperMagnete.ch (2012, 18th of December) What is the development of neodymium magnet prices. Available from: www.supermagnete.ch. |
| [29] | Sumankik-Leary J, Piggott H, Howell R, et al (2013) Locally manufactured small wind turbines—How do they compare to commercial machines? in Proceedings of the 9th PhD Seminar on Wind Energy in Europe 18-20 March 2013, Uppsala University. Available from: http://scoraigwind.co.uk/wp-content/uploads/2013/11/PhD_Seminar_2013_FullPaper_Sumanik-Leary-FINAL.pdf. |
| [30] | blueEnergy (2009 and 2010) Diagnóstico socio-económico de capacidades organizacionales y prioridades con enfoque de género, energía y agua (varias comunidades), blueEnergy internal document. |
| [31] | Hirmer S, Cruickshank H (2014) The user-value of rural electrification: An analysis and adoption of existing models and theories in Renewable and Sustainable Energy Reviews, 34, 145-154. |
| [32] | Vanheule L. (2012) Small Wind Turbines in Kenya—An Analysis with Strategic Niche Management, Department of Technology Dynamics & Sustainable Development, Delft University of Technology.Marandin L, Craig M, Casillas CE, et al. (2013) Small-scale Wind Power in Nicaragua—Market Analysis 2012-2013, Green Empowerment. |

Figures(14) / Tables(13)

Pedro Neves, Morten Gleditsch, Cindy Bennet, Mathias Craig, Jon Sumanik-Leary. Assessment of locally manufactured small wind turbines as an appropriate technology for the electrification of the Caribbean Coast of Nicaragua[J]. AIMS Energy, 2015, 3(1): 41-74. doi: 10.3934/energy.2015.1.41







 DownLoad:
DownLoad: