Last cholera epidemic has been recorded in Bangladesh between 1992–1993, while few sporadic localized outbreaks have been reported as recent as 2005. Serotype O1 of Vibrio cholera is considered as the principal causative agent which transmits through contaminated drinking water resulting that epidemic. Therefore, the objective of this research was to isolate V. cholera in 3 different water sources; River, pond and tube-well, in 5 different locations of Gazipur, Bangladesh, and to analyze their antibiogram study. A total of 45 water samples were randomly collected for the isolation and identification of Vibrio spp. Samples are then serially diluted in alkaline peptone water and streak on Thiosulfate Citrate Bile Salt Sucrose-TCBS agar for quantification of V. spp. For V. cholera isolation water samples were first enriched in nutrient broth at 37 °C for 16 hours followed by cultivation in selective media; TCBS agar at 37 °C for 24 hours. Yellow colonies on TCBS agar were screed as V. cholera and was confirmed by analyzing their biochemical characteristics like Catalase, Oxidase, MR, VP, Indole, Sugar fermentation. Following isolation antibiotic sensitivity test was performed on each V. cholera isolates to determine their antibiotic sensitivity profile. The results showed, out of 45 samples 12 contained V. cholera. Tube-well water has significantly lower concentration (log CFU/mL) of V. spp. than river and pond water (P < 0.05). Bacterial concentration doesn't deviate (P > 0.05) significantly in 5 different location the sample was collected from. All the 12 isolates were sensitive to Gentamicin and ciprofloxacin (100%), while Chloramphenicol (91.67%), Sulfamethoxazole (91.67%), Azithromycin (66.67%) showed high sensitivity. Isolates showed marginal sensitivity towards Tetracycline (33.33%), and Cephalexin (16.67%) and 100% resistance against antibiotics like Vancomycin, Penicillin, Erythromycin, and Nalidixic Acid. Based on these data we recommend using tube-well water instead of river and pond water for drinking purposes. Furthermore, we suggest selective use of sensitive antimicrobials listed here for therapeutics of cholera outbreak.
Citation: Md. Aoulad Hosen, Fozol Korim Ovi, Harunur Rashid, MD. Hasibul Hasan, Md. Abdul Khalek, Mahmudul Hasan, Farhana Easmin, Nazmi Ara Rumi, Mohammad Shariful Islam. Characterization of Vibrio spp. in environmental water samples collected from flood prone areas of Bangladesh and their antibiotic resistance profile[J]. AIMS Microbiology, 2021, 7(4): 471-480. doi: 10.3934/microbiol.2021028
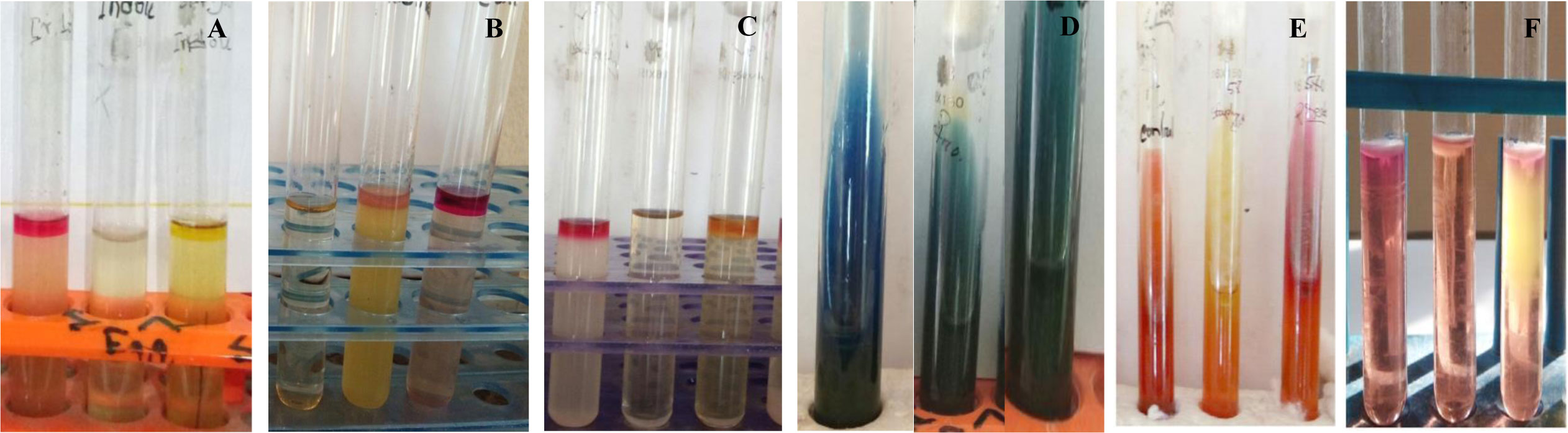
Last cholera epidemic has been recorded in Bangladesh between 1992–1993, while few sporadic localized outbreaks have been reported as recent as 2005. Serotype O1 of Vibrio cholera is considered as the principal causative agent which transmits through contaminated drinking water resulting that epidemic. Therefore, the objective of this research was to isolate V. cholera in 3 different water sources; River, pond and tube-well, in 5 different locations of Gazipur, Bangladesh, and to analyze their antibiogram study. A total of 45 water samples were randomly collected for the isolation and identification of Vibrio spp. Samples are then serially diluted in alkaline peptone water and streak on Thiosulfate Citrate Bile Salt Sucrose-TCBS agar for quantification of V. spp. For V. cholera isolation water samples were first enriched in nutrient broth at 37 °C for 16 hours followed by cultivation in selective media; TCBS agar at 37 °C for 24 hours. Yellow colonies on TCBS agar were screed as V. cholera and was confirmed by analyzing their biochemical characteristics like Catalase, Oxidase, MR, VP, Indole, Sugar fermentation. Following isolation antibiotic sensitivity test was performed on each V. cholera isolates to determine their antibiotic sensitivity profile. The results showed, out of 45 samples 12 contained V. cholera. Tube-well water has significantly lower concentration (log CFU/mL) of V. spp. than river and pond water (P < 0.05). Bacterial concentration doesn't deviate (P > 0.05) significantly in 5 different location the sample was collected from. All the 12 isolates were sensitive to Gentamicin and ciprofloxacin (100%), while Chloramphenicol (91.67%), Sulfamethoxazole (91.67%), Azithromycin (66.67%) showed high sensitivity. Isolates showed marginal sensitivity towards Tetracycline (33.33%), and Cephalexin (16.67%) and 100% resistance against antibiotics like Vancomycin, Penicillin, Erythromycin, and Nalidixic Acid. Based on these data we recommend using tube-well water instead of river and pond water for drinking purposes. Furthermore, we suggest selective use of sensitive antimicrobials listed here for therapeutics of cholera outbreak.

| [1] |
Harris JB, LaRocque RC, Qadri F, et al. (2012) Cholera. Lancet 379: 2466-2476. doi: 10.1016/S0140-6736(12)60436-X

|
| [2] |
Gaffga NH, Tauxe RV, Mintz ED (2007) Cholera: a new homeland in Africa? Am J Trop Med Hyg 77: 705-713. doi: 10.4269/ajtmh.2007.77.705
|
| [3] |
Biswas DK, Bhunia R, Maji D, et al. (2014) Contaminated pond water favors cholera outbreak at haibatpur village, purba medinipur district, west bengal, India. J Trop Med 2014: 764530. doi: 10.1155/2014/764530
|
| [4] |
Schärer K, Savioz S, Cernela N, et al. (2011) Occurrence of Vibrio spp. in fish and shellfish collected from the Swiss market. J Food Prot 74: 1345-1347. doi: 10.4315/0362-028X.JFP-11-001
|
| [5] | Mrityunjoy A, Kaniz F, Fahmida J, et al. (2013) Prevalence of Vibrio cholera in different food samples in the city of Dhaka, Bangladesh. Int Food Res J 20: 1017-1022. |
| [6] | Sarkar MKD, Ahmmed T, Shahabuddin Md, et al. (2019) Antibiotic resistance analysis of Vibrio spp. isolated from different types of water sources of Bangladesh and their characterization. Eur J Med Health Sci 1: 19-29. |
| [7] | Huq A, Haley BJ, Taviani E (2012) Detection, isolation, and identification of V. cholera from the environment. Curr Protoc Microbio Chapter 6: Unit6A.5. |
| [8] | Clinical Laboratory Standards Institute (2006) Performance standards for antimicrobial disk susceptibility tests. Clinical Laboratory Standards Institute CLSI document M2-A9, 1. |
| [9] |
Bauer AW, Kirby WMN, Sherris JC, et al. (1966) Antibiotic susceptibility testing by a standardized single disk method. Am J Clin Pathol 36: 493-496. doi: 10.1093/ajcp/45.4_ts.493
|
| [10] | Shrestha SD, Malla S, Adhikari B, et al. (2010) Antibiotic susceptibility patterns of V. cholera isolates. JNMA J Nepal Med Assoc 49: 232-236. |
| [11] | Colwell RR (1996) Global climate and infectious disease: the cholera paradigm. Am Assoc Adv Sci 274: 2025-2031. |

Figures(2) / Tables(7)

Md. Aoulad Hosen, Fozol Korim Ovi, Harunur Rashid, MD. Hasibul Hasan, Md. Abdul Khalek, Mahmudul Hasan, Farhana Easmin, Nazmi Ara Rumi, Mohammad Shariful Islam. Characterization of Vibrio spp. in environmental water samples collected from flood prone areas of Bangladesh and their antibiotic resistance profile[J]. AIMS Microbiology, 2021, 7(4): 471-480. doi: 10.3934/microbiol.2021028







 DownLoad:
DownLoad: