Citation: Lei Shi, Hongyong Zhao, Daiyong Wu. Modelling and analysis of HFMD with the effects of vaccination, contaminated environments and quarantine in mainland China[J]. Mathematical Biosciences and Engineering, 2019, 16(1): 474-500. doi: 10.3934/mbe.2019022

| [1] | F. C. Tseng, H. C. Huang, C. Y. Chi, T. L. Lin, C. C. Liu, J. W. Jian, L. C. Hsu, H. S. Wu, J. Y. Yang and Y. W. Chang, Epidemiological survey of enterovirus infections occurring in Taiwan between 2000 and 2005: analysis of sentinel physician surveillance data, J. Med. Virol., 79 (2007), 1850–1860. |
| [2] | Q. Zhu, Y. Hao, J. Ma, S. Yu and Y. Wang, Surveillance of hand, foot, and mouth disease in mainland China (2008-2009), Biomed. Environ. Sci., 24 (2011), 349–356. |
| [3] | Chinese Center for Disease Control and Prevention (CCDC), National Public Health Statistical Data. 2018 Available from: http://www.chinacdc.cn/tjsj/fdcrbbg/index.html. |
| [4] | N. J. Schmidt, E. H. Lennette and H. H. Ho, An apparently new enterovirus isolated from patients with disease of the central nervous system, J. Infect. Dis., 129 (1974), 304–309. |
| [5] | G. L. Repass, W. C. Palmer and F. F. Stancampiano, Hand, foot and mouth disease: identifying and managing an acute viral syndrome, Clev. Clin. J. Med., 81 (2014), 537–543. |
| [6] | M. Cabrerizo, D. Tarragó, C. Muñoz-Almagro, A. E. Del, M. Domínguez-Gil, J. M. Eiros, I. López-Miragaya, C. P´erez, J. Reina and A. Otero, Molecular epidemiology of enterovirus 71, coxsackievirus A16 and A6 associated with hand, foot and mouth disease in Spain, Clin. Microbiol. Infec., 20 (2014), O150–O156. |
| [7] | S. Ljubin-Sternak, V. Slavic-Vrzic, T. Vilibić-Č avlek and I. Gjenero-Margan, Outbreak of hand, foot and mouth disease caused by coxsackie A16 virus in a childcare center in croatia, European Communicable Disease Bulletin, 21 (2011), 9–11. |
| [8] | N. Sarma, A. Sarkar, A. Mukherjee, A. Ghosh, S. Dhar and R. Malakar, Epidemic of hand, foot and mouth disease in west bengal, india in august, 2007: a multicentric study, Indian J. Dermatol., 54 (2009), 26–30. |
| [9] | O. M. How,W. S. Chang, M. Anand, P. Yuwana, P. David, C. Daniella, D. S. Sylvia, C. C. Hee, T. P. Hooi and C. M. Jane, Identification and validation of clinical predictors for the risk of neurological involvement in children with hand, foot, and mouth disease in Sarawak, Bmc Infect. Dis., 9 (2009), 3–3. |
| [10] | T. Fujimoto, M. Chikahira, S. Yoshida, H. Ebira, A. Hasegawa, A. Totsuka and O. Nishio, Outbreak of central nervous system disease associated with hand, foot, and mouth disease in Japan during the summer of 2000: detection and molecular epidemiology of enterovirus 71, Microbiol. Immunol., 46 (2002), 621–627. |
| [11] | J.Wang, Z. Cao, D. D. Zeng, Q.Wang, X.Wang and H. Qian, Epidemiological analysis, detection, and comparison of space-time patterns of Beijing hand-foot-mouth disease (2008-2012), PLoS One, 9 (2014). Article ID: e92745. |
| [12] | W. S. Ryu, B. Kang, J. Hong, S. Hwang, J. Kim and D. S. Cheon, Clinical and etiological characteristics of enterovirus 71-related diseases during a recent 2-year period in Korea, J. Clin. Microbiol., 48 (2010), 2490–2494. |
| [13] | J. Cheng, J.Wu, Z. Xu, R. Zhu, X.Wang, K. Li, L.Wen, H. Yang and H. Su, Associations between extreme precipitation and childhood hand, foot and mouth disease in urban and rural areas in Hefei, China, Sci. Total Environ., 497 (2014), 484–490. |
| [14] | H. X. Nguyen, C. Chu, H. L. T. Nguyen, H. T. Nguyen, C. M. Do, S. Rutherford and D. Phung, Temporal and spatial analysis of hand, foot, and mouth disease in relation to climate factors: A study in the Mekong Delta region, Vietnam, Sci. Total Environ., 581 (2017), 766–772. |
| [15] | F. Gou, X. Liu, X. Ren, D. Liu, H. Liu, K. Wei, X. Yang, Y. Cheng, Y. Zheng and X. Jiang, Socioecological factors and hand, foot and mouth disease in dry climate regions: a Bayesian spatial approach in Gansu, China, Int. J. Biometeorol., 61 (2017), 137–147. |
| [16] | W. Jing, T. Hu, D. Sun, S. Ding, M. J. Carr, W. Xing, S. Li, X. Wang and W. Shi, Epidemiological characteristics of hand, foot, and mouth disease in Shandong, China, 2009-2016, Sci. Rep., 7 (2017). Article ID: 8900. |
| [17] | Y. Weng, W. Chen, W. He, M. Huang, Y. Zhu and Y. Yan, Serotyping and genetic characterization of hand, foot, and mouth disease (HFMD)-associated enteroviruses of no-ev71 and non-cva16 circulating in fujian, china, 2011-2015, Med. Sci. Monitor, 23 (2017), 2508–2518. |
| [18] | National Health and Family Planning Commission of the Peoples Republic of China (NHFPC), China Health Statistical Yearbook. 2018 Available from: http://www.moh.gov.cn/zwgk/yqbb3/ejlist.shtml. |
| [19] | Z. Chang, F. Liu, L. Bin, Z. Wang and L. Zeng, Analysis on surveillance data of hand, foot and mouth disease in China, January - May 2017, Disease Surveillance, 32 (2017), 447–452. |
| [20] | Y. Cao, Z. Hong, L. Jin, O. U. Jian-Ming and R. Hong, Surveillance of hand, foot and mouth disease in China, 2011-2012, Disease Surveillance, 28 (2013), 975–980. |
| [21] | J. Sun, Z. Chang, L. Wang and L. Wang, Analysis on the epidemic situation of hand, foot and mouth disease in China in January - March, 2013, Practical Prev. Med., 21 (2014), 183–186. |
| [22] | J. T. Wu, M. Jit, Y. Zheng, K. Leung and W. Xing, Routine pediatric enterovirus 71 vaccination in China: a cost-effectiveness analysis, Plos Med., 13 (2016). Article ID: e1002013. |
| [23] | S. Takahashi, Q. Liao, T. P. Van Boeckel, W. Xing, J. Sun, V. Y. Hsiao, C. J. Metcalf, Z. Chang, F. Liu and J. Zhang, Hand, foot, and mouth disease in China: modeling epidemic dynamics of enterovirus serotypes and implications for vaccination, Plos Med., 13 (2016). Article ID: e1001958. |
| [24] | N. Ziyadi, A male-female mathematical model of human papillomavirus (HPV) in African American population, Math. Biosci. Eng., 14 (2017), 339–358. |
| [25] | S. Liu, Y. Li, Y. Bi, and Q. Huang, Mixed vaccination strategy for the control of tuberculosis: A case study in China, Math. Biosci. Eng., 14 (2017), 695–708. |
| [26] | M. L. Manyombe, J. Mbang, J. Lubuma and B. Tsanou, Global dynamics of a vaccination model for infectious diseases with asymptomatic carriers, Math. Biosci., 13 (2016), 813–840. |
| [27] | Y. C. Wang and F. C. Sung, Modeling the infections for Enteroviruses in Taiwan, Taipei: Institute of Environmental Health (2006). Article ID: 228559790. |
| [28] | F. C. S. Tiing and J. Labadin, A simple deterministic model for the spread of hand, foot and mouth disease (HFMD) in Sarawak, 2008 Second Asia International Conference on Modelling & Simulation, (2008), 947–952. |
| [29] | N. Roy, Mathematical modeling of hand-foot-mouth disease: quarantine as a control measure, Int. J. Adv. Sci. Eng. Technol. Res., 1 (2012), 1–11. |
| [30] | Y. Ma, M. Liu, Q. Hou and J. Zhao, Modelling seasonal HFMD with the recessive infection in Shandong, China, Math. Biosci. Eng., 10 (2013), 1159–1171. |
| [31] | J.Wang, Y. Xiao and R. A. Cheke, Modelling the effects of contaminated environments on HFMD infections in mainland China, Marriage Fam Rev, 35 (2016), 77–97. |
| [32] | J. Wang, Y. Xiao and Z. Peng, Modelling seasonal HFMD infections with the effects of contaminated environments in mainland China, Appl. Math. Comput., 271 (2016), 615–627. |
| [33] | Y. Zhu, B. Xu, X. Lian, W. Lin, Z. Zhou and W. Wang, A hand-foot-and-mouth disease model with periodic transmission rate in Wenzhou, China, Abstr. Appl. Anal., 15 (2014), 1–11. |
| [34] | Y. Li, J. Zhang and X. Zhang, Modelling and preventive measures of hand, foot and mouth disease (HFMD) in China, Int. J. Environ. Res. Pub. Heal., 11 (2014), 3108–3117. |
| [35] | Y. Li, L. Wang, L. Pang and S. Liu, The data fitting and optimal control of a hand, foot and mouth disease (HFMD) model with stage structure, Appl. Math. Comput., 276 (2016), 61–74. |
| [36] | J. Liu, Threshold dynamics for a HFMD epidemic model with periodic transmission rate, Nonlinear Dynam., 64 (2011), 89–95. |
| [37] | J. Y. Yang, Y. Chen and F. Q. Zhang, Stability analysis and optimal control of a hand-foot-mouth disease (HFMD) model, J. Appl. Math. Comput., 41 (2013), 99–117. |
| [38] | G. P. Samanta, Analysis of a delayed hand-foot-mouth disease epidemic model with pulse vaccination, Syst. Sci. Control Eng., 2 (2014), 61–73. |
| [39] | R. Viriyapong and S. Wichaino, Mathematical modeling of hand, foot and mouth disease in the Northern Thailand, Far East J. Math. Sci., 100 (2016), 805–820. |
| [40] | S. Sharma and G. P. Samanta, Analysis of a hand-foot-mouth disease model, Int. J. Biomath., 10 (2017). Article ID: 1750016. |
| [41] | P. V. D. Driessche and J. Watmough, Reproduction numbers and sub-threshold endemic equilibria for compartmental models of disease, Math. Biosci., 180 (2002), 29–48. |
| [42] | W. M. Hirsch, H. Hanisch and J. P. Gabriel, Differential equation models of some parasitic infections: methods for the study of asymptotic behavior, Commun. Pure. Appl. Math., 38 (1985), 733-753. |
| [43] | X. Zhao, Uniform persistence and periodic coexistence states in infinite-dimensional periodic semiflows with applications, Can. Appl. Math. Q., 3 (1995), 473–495. |
| [44] | W. Wang and X. Zhao, An epidemic model in a patchy environment, Math. Biosci., 190 (2004), 97–112. |
| [45] | National Bureau of Statistics of China (NBSC), China Demographic Yearbook of 2013, 2014, 2015, 2016, 2017. 2018 Available from: http://www.stats.gov.cn/tjsj/ndsj/. |
| [46] | S. Marino, I. B. Hogue, C. J. Ray and D. E. Kirschner, A methodology for performing global uncertainty and sensitivity analysis in systems biology, J. Theor. Biol., 254 (2008), 178–196. |
| [47] | Y. Xiao, Y. Zhou and S. Tang, Principles of biological mathematics, Xi'an Jiaotong University Press, 2012. |
| [48] | H. O. Hartley, A. Booker, Nonlinear Least Squares Estimation, Ann. Math. Stat., 36 (1965), 638– 650. |
| [49] | G. Arminger and B. O. Muth´en, A Bayesian approach to nonlinear latent variable models using the Gibbs sampler and the Metropolis-Hastings algorithm, Psychometrika, 63 (1998), 271–300. |
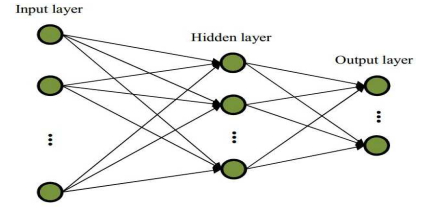
| [50] | S. S. Haykin, Neural networks and learning machines, China Machine Press, 2009. |
Figures(12) / Tables(5)

Lei Shi, Hongyong Zhao, Daiyong Wu. Modelling and analysis of HFMD with the effects of vaccination, contaminated environments and quarantine in mainland China[J]. Mathematical Biosciences and Engineering, 2019, 16(1): 474-500. doi: 10.3934/mbe.2019022







 DownLoad:
DownLoad: