Citation: J. Nwando Olayiwola, Melanie Raffoul. Saving Women, Saving Families: An Ecological Approach to Optimizing the Health of Women Refugees with S.M.A.R.T Primary Care[J]. AIMS Public Health, 2016, 3(2): 357-374. doi: 10.3934/publichealth.2016.2.357

| [1] | United Nations. Refugees, the numbers: Resources for Speakers on Global Issues. 2015. Available from: http://www.un.org/en/globalissues/briefingpapers/refugees/. |
| [2] | European Commission, Directorate-General for Health and Food Safety. Health assessment of refugees and migrants in the EU/EEA. 2015. Available from: http://ec.europa.eu/dgs/health_food-safety/docs/personal_health_handbook_en.pdf. |
| [3] | Frances Nicholson, United Nations High Commission for Refugees. Refugee women, survivors, protectors, providers. 2011. Available online from: http://www.unhcr.org.uk/resources/monthly-updates/november-2011-update/refugee-women-survivors-protectors-providers.html. |
| [4] | Fazel M, Reed R, Panter-Brick C, et al. (2012) Mental health of displaced and refugee children resettled in high-income countries: risk and protective factors. Lancet 379, no. 9812: 266-82. |
| [5] | Lucas, R. (2005) International migration to the high-income countries: Some consequences for economic development in the sending countries. Are we on track to achieve the Millennium Development Goals: 127-81. |
| [6] | United Nations High Commission for Refugees. A new beginning: Refugee integration in Europe. 2013. Available from: www.unhcr.org/52403d389.pdf. |
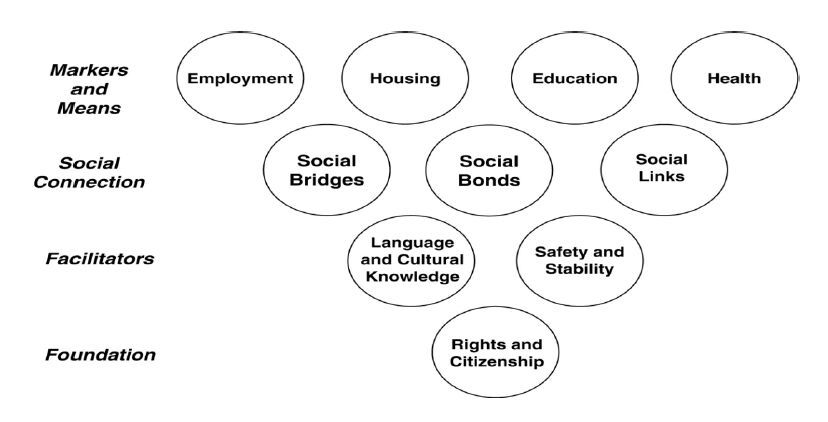
| [7] | Ager A, Strang A. (2008) Understanding integration: A conceptual framework. J Refug Stud 21(2): 166-91. |
| [8] | Robinson, V. (1998) Defining and measuring successful refugee integration. In Proceedings of ECRE International conference on Integration of Refugees in Europe, Antwerp November 1998. |
| [9] | Ager, Alastair, and Alison Strang. Indicators of integration: Final report. Home Office, Research, Development and Statistics Directorate, 2004. |
| [10] |
Fazel M, Wheeler J, Danesh J. (2005) Prevalence of serious mental disorder in 7000 refugees resettled in Western countries: A systematic review. Lancet 365:1309-14. doi: 10.1016/S0140-6736(05)61027-6

|
| [11] |
Asgary R, Segar M. (2011) Barriers to healthcare access among refugee asylum seekers. J Health Care for the Poor and Underserved 22:506-522. doi: 10.1353/hpu.2011.0047
|
| [12] | Pollard R, Betts, W, Carroll J, et al. (2014) Integrating primary care with behavioral health with four special populations: children with special needs, people with serious mental illness, refugees, and deaf people. Am Psychol 69(4): 377-87. |
| [13] | Executive board of the United Nations Entity for Gender Equality and the Empowerment of Women. 2011. Available online from: http://www.unwomen.org/~/media/Headquarters/Attachments/Sections/Executive%20Board/EB-2011-AS-UNW-2011-09-StrategicPlan-en.pdf. |
| [14] | Women, U. N., and UN Global Compact. "Women’s Empowerment Principles: Equality Means Business." New York City: UN Women, 2010. |
| [15] | The Partnership for Maternal, Newborn, and Child health; Partners in Population and development. Women’s empowerment and gender equality: Promoting women’s empowerment for better health outcomes for women and children. 2013. Available online from: http://www.opml.co.uk/sites/default/files/sb_gender_0.pdf. |
| [16] | Kishor, S. (2000) Empowerment of women in Egypt and links to the survival and health of their infants. In B.Presser & G. Sen (Eds.), Women’s empowerment and demographic processes. 119-156. New York: Oxford University Press. |
| [17] | Kar S, Pascual C, Chickering K. (1999) Empowerment of women for health promotion: a meta-analysis. Soc Sci Med 49(11): 1431-60. |
| [18] | Costa, D. (2007). Health care of refugee women. Australian Family Physician 36(3): 151. |
| [19] | Starfield B, Shi L, Macinko J. (2005) Contribution of primary care to health systems and health. Milbank Q 83(3): 457-502. |
| [20] | World Health Organization. "The World Health Report 2008: Primary health care (now more than ever)." Available online from: http://www.who.int/whr/2008/whr08_en.pdf. |
| [21] | Declaration of Alma-Ata, 1978. World Health Organization, 2005. |
| [22] | Redwood-Campbell L, Thind H, Howard M, et al. (2008) Understanding the health of refugee women in host countries: lessons from the Kosovar re-settlement in Canada. Prehospital and Disaster Med 23(04): 322-7. |
| [23] | Hadle C, Zodhiates A, Sellen D. (2007) Acculturation, economics and food insecurity among refugees resettled in the USA: a case study of West African refugees. Public Health Nutr 10(4): 405-12. |
| [24] | Pumariega A, Rothe E, Pumariega J. (2005) Mental health of immigrants and refugees. Community Ment Health J 41(5): 581-97. |
| [25] | O'Hare T, Van Tran T. (1998) Substance abuse among Southeast Asians in the US: Implications for practice and research. Soc Work in Health Care 26 (3): 69-80. |
| [26] | Wieland M, Weis J, Palmer T, et al. (2012) Physical activity and nutrition among immigrant and refugee women: a community-based participatory research approach. Women's Health 22(2): e225-e232. |
| [27] | Hynie M, Crooks V, Barragan J. (2011) Immigrant and refugee social networks: determinants and consequences of social support among women newcomers to Canada. Can J Nurs Res 43(4): 26-46. |
| [28] | Lim S. (2009) Loss of Connections Is Death: Transnational Family Ties Among Sudanese Refugee Families Resettling in the United States. J Cross-Cult Psychol 40, no. 6: 1028-40. |
| [29] | Muggeridge H, Dona G. (2006) Back Home? Refugees' experiences of their first visit back to their country of origin. J Refug Stud 19(4): 415-32. |
| [30] | McPherson, M. (2010) ‘I Integrate, Therefore I Am’: Contesting the Normalizing Discourse of Integrationism through Conversations with Refugee Women. J Refug Stud feq040. |
| [31] | Kennedy J, Seymour D, Hummel B. (1999) A comprehensive refugee health screening program. Public Health Rep 114(5): 469. |
| [32] | Colic-Peisker V, Walker I. (2003) Human capital, acculturation and social identity: Bosnian refugees in Australia. J Community & Appl Soc Psychol 13, no. 5: 337-60. |
| [33] | Oxman-Martinez J, Abdool S. (2000) Immigration, women and health in Canada. Can J Public Health 91(5): 394. |
| [34] | Wrigley, H. (2007). Beyond the life boat: Improving language, citizenship and training services for immigrants and refugees. In A. Belzer (Ed.) Toward defining and improving quality in adult basic education: Issues and challenges. Mahwah, New Jersey, Erlbaum Publishing, 221-239. |
| [35] | Wolf M, Ly U, Hobart M, Kernic M. (2003) Barriers to seeking police help for intimate partner violence. J Fam Violence 18(2):121-9. |
| [36] | United Nations High Commission for Refugees. News stories: New Delhi police teach refugee women how to take care of themselves. 2012. Available from: http://www.unhcr.org/507410439.html. |
| [37] | Fong, R. (Ed.). (2004). Culturally competent practice with immigrant and refugee children and families. Guilford Press. |
| [38] | Lurie N, Jung M, Lavizzo-Mourey R. (2005) Disparities and quality improvement: federal policy levers. Health Aff 24(2): 354-64. |
| [39] | Higgins, Andrew for the New York Times: Norway offers migrants a lesson in how to treat women. 2015. Available from: http://www.nytimes.com/2015/12/20/world/europe/norway-offers-migrants-a-lesson-in-how-to-treat-women.html?_r=1. |
| [40] | Olayiwola, Willard-Grace, Dube, Hessler, Shunk, Gottlieb (unpublished data, manuscript under review). |
| [41] | Bachrach D, Pfister H, Wallis K, et al. Addressing patients’ social needs: An emerging business case for provider investment. The Commonwealth Fund. 2014. Available from: http://www.commonwealthfund.org/~/media/files/publications/fund-report/2014/may/1749_bachrach_addressing_patients_social_needs_v2.pdf. |
| [42] | Tipirneni R, Vickery K, Ehlinger, E. (2015) Accountable Communities for Health: Moving From Providing Accountable Care to Creating Health. Ann Fam Med 13(4): 367-9. |
| [43] | Van Dooren G, Coomans S, Struyven L. (2014) Identifying Policy Innovations increasing Labour Market Resilience and Inclusion of Vulnerable Groups National Report Belgium. INSPIRES Working Paper Series 14: 1-48. |
| [44] | European Resettlement Network. Belgium Stakeholder Conference on Refugee Resettlement. 2015. Available from: http://www.resettlement.eu/page/belgium-stakeholder-conference-refugee-resettlement-brussels-june-23-2015. |
| [45] | San Francisco Department of Public Health. Community health equity and promotion: Newcomers Health Program. Available from: https://www.sfdph.org/dph/comupg/oprograms/CHPP/Newcomers/NewcomersStaffSites.asp. |
| [46] | Heather Knight for SF Gate. Medicine S.F. General provides lifeline to traumatized asylum-seekers. 2011. Available from: http://www.sfgate.com/bayarea/article/S-F-General-s-refugee-clinic-a-lifeline-to-care-2366663.php. |
| [47] | Theo Chang for the White House blog. Making good use of AARA funding: Frank Kiang Medical Center. 2010. Available from: https://www.whitehouse.gov/blog/2010/08/02/making-good-use-aara-funding-frank-kiang-medical-center. |
| [48] | Chang K, Jeung J, Pei P, et al. (2014) "Opening Access for Burmese and Karen Immigrant and Refugee Populations in California: A Blueprint for Integrated Health Service Expansion to Emerging Asian Communities." AAPI Nexus: Policy, Pract Community 12(1-2): 225-44. |
| [49] | Chang K, Pei P, Charlemagne L, et al. The Intersection of Culture and Behavioral Health —— Moving Beyond Language. Community Health Forum Magazine. National Association of Community Health Centers. 2012. Available from: http://www.nachc.com/magazine-article.cfm?MagazineArticleID=228. |
| [50] |
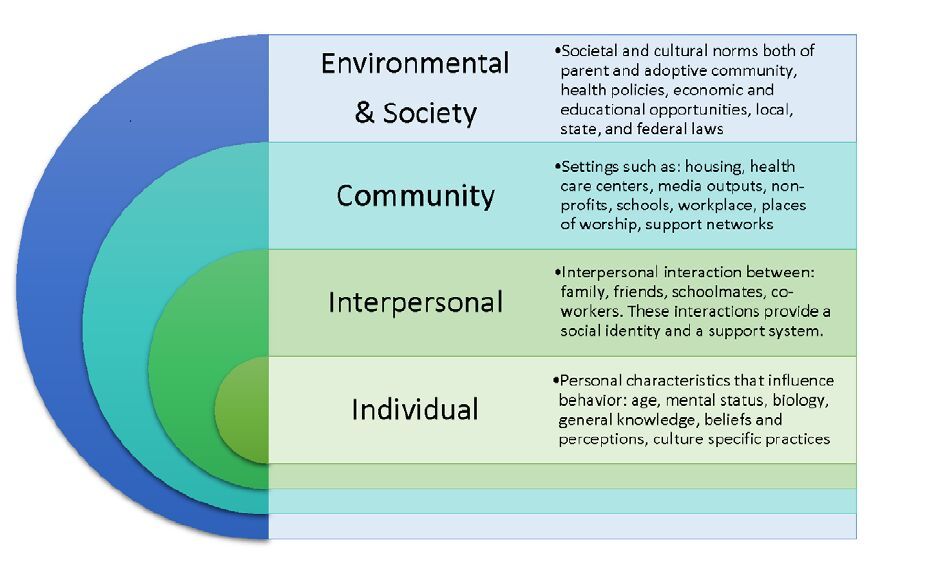
Edberg M, Cleary S, Vyas A. (2011) A trajectory model for understanding and assessing health disparities in Immigrant/Refugee communities. J Immigr Minority Health 13: 576-84.
n Canada. Can J Public Health 91(5): 394. doi: 10.1007/s10903-010-9337-5
|
Figures(4)

J. Nwando Olayiwola, Melanie Raffoul. Saving Women, Saving Families: An Ecological Approach to Optimizing the Health of Women Refugees with S.M.A.R.T Primary Care[J]. AIMS Public Health, 2016, 3(2): 357-374. doi: 10.3934/publichealth.2016.2.357







 DownLoad:
DownLoad: