The coronavirus pandemic (COVID-19) is an unprecedented global health crisis with emotional and physical impact on health care workers.
The purpose of this study was to investigate the levels of fatigue and burnout in nursing staff during the pandemic.
The present study involved nursing staff from hospitals in Greece in February 2021, who completed the Fatigue (FAS) and Burnout (CBI) questionnaires. Gender, age, years of work experience, workplace (COVID-19 or non-COVID-19 wards) and SARS-CoV-2 infection status were recorded.
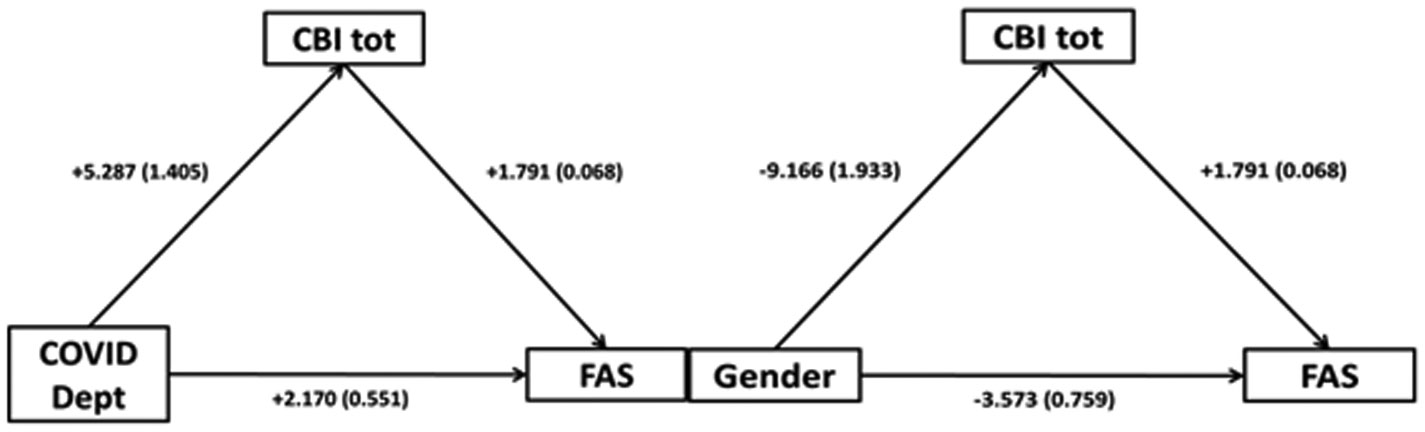
The sample included 593 women and 108 men, with a mean age ± SD: 42.9 ± 9.9 years and 18.14 ± 10.8 years work experience. Slightly more than half, (367, 52.4%) worked in COVID-19 departments. Fifty-six (8%) tested positive for SARS-CoV-2 and 14 of them needed to be treated. The mean ± SD FAS and CBI scores were 25.6 ± 7.4 and 46.9 ± 18.8, respectively (67.9% and 42.9% had scores suggestive of fatigue and burnout, respectively). Women showed higher values in both scales (p < 0.01). Subjects working in COVID-19 wards scored significantly higher on both the FAS and CBI scales; they were also younger and with less work experience (p < 0.01). Staff treated for COVID-19 scored higher on the burnout scale (p < 0.01) than the uninfected staff. Fatigue showed a strong positive correlation with burnout (p < 0.01, r = 0.70). Stepwise multiple regression showed that the variation of fatigue was explained by 47.0% and 6.1% by the scores on the subscales of personal and work-related burnout, respectively.
In conclusion, high rates of fatigue and burnout were found in the studied population. Nurses working with COVID-19 patients had higher rates of fatigue and burnout compared to those working elsewhere. There was a strong positive correlation (r = 0.70) between burnout and fatigue. Particular attention should be paid to staff who became ill and need to be treated.
Citation: Christos Sikaras, Ioannis Ilias, Athanasios Tselebis, Argyro Pachi, Sofia Zyga, Maria Tsironi, Andrea Paola Rojas Gil, Aspasia Panagiotou. Nursing staff fatigue and burnout during the COVID-19 pandemic in Greece[J]. AIMS Public Health, 2022, 9(1): 94-105. doi: 10.3934/publichealth.2022008
The coronavirus pandemic (COVID-19) is an unprecedented global health crisis with emotional and physical impact on health care workers.
The purpose of this study was to investigate the levels of fatigue and burnout in nursing staff during the pandemic.
The present study involved nursing staff from hospitals in Greece in February 2021, who completed the Fatigue (FAS) and Burnout (CBI) questionnaires. Gender, age, years of work experience, workplace (COVID-19 or non-COVID-19 wards) and SARS-CoV-2 infection status were recorded.
The sample included 593 women and 108 men, with a mean age ± SD: 42.9 ± 9.9 years and 18.14 ± 10.8 years work experience. Slightly more than half, (367, 52.4%) worked in COVID-19 departments. Fifty-six (8%) tested positive for SARS-CoV-2 and 14 of them needed to be treated. The mean ± SD FAS and CBI scores were 25.6 ± 7.4 and 46.9 ± 18.8, respectively (67.9% and 42.9% had scores suggestive of fatigue and burnout, respectively). Women showed higher values in both scales (p < 0.01). Subjects working in COVID-19 wards scored significantly higher on both the FAS and CBI scales; they were also younger and with less work experience (p < 0.01). Staff treated for COVID-19 scored higher on the burnout scale (p < 0.01) than the uninfected staff. Fatigue showed a strong positive correlation with burnout (p < 0.01, r = 0.70). Stepwise multiple regression showed that the variation of fatigue was explained by 47.0% and 6.1% by the scores on the subscales of personal and work-related burnout, respectively.
In conclusion, high rates of fatigue and burnout were found in the studied population. Nurses working with COVID-19 patients had higher rates of fatigue and burnout compared to those working elsewhere. There was a strong positive correlation (r = 0.70) between burnout and fatigue. Particular attention should be paid to staff who became ill and need to be treated.

| [1] |
Jarrahi A, Ahluwalia M, Khodadadi H, et al. (2020) Neurological consequences of COVID-19: what have we learned and where do we go from here? J Neuroinflammation 17: 286. doi: 10.1186/s12974-020-01957-4

|
| [2] |
Burkhart Sasangohar F, Jones SL, Masud FN, et al. (2020) Provider burnout and fatigue during the COVID-19 pandemic: lessons learned from a high-volume intensive care unit. Anesth Analg 131: 106-111. doi: 10.1213/ANE.0000000000004866
|
| [3] | Stedman T (2005) Stedman's medical dictionary Dalcassian publishing company. |
| [4] |
Zhan YX, Zhao SY, Yuan J, et al. (2020) Prevalence and influencing factors on fatigue of first-line nurses combating with COVID-19 in China: a descriptive cross-sectional study. Curr Med Sci 40: 625-635. doi: 10.1007/s11596-020-2226-9
|
| [5] |
Graham KC, Cvach M (2010) Monitor alarm fatigue: standardizing use of physiological monitors and decreasing nuisance alarms. Am J Crit Care 19: 28-34. doi: 10.4037/ajcc2010651
|
| [6] |
Batra K, Singh TP, Sharma M, et al. (2020) Investigating the psychological impact of COVID-19 among healthcare workers: a meta-analysis. Int J Environ Res Public Health 17: 9096. doi: 10.3390/ijerph17239096
|
| [7] |
Arnsten AFT, Shanafelt T (2021) Physician distress and burnout: the neurobiological perspective. Mayo Clin Proc Mar 96: 763-769. doi: 10.1016/j.mayocp.2020.12.027
|
| [8] |
Schaufeli WB, Greenglass ER (2021) Introduction to special issue on burnout and health. Psychol Health 16: 501-510. doi: 10.1080/08870440108405523
|
| [9] | ICD-10 Version: 2010 Available from: https://icd.who.int/browse10/2010/en. |
| [10] |
Rettig AE, Moore K, Savona E, et al. (2021) Take-a-break intervention: improving oncology nurse wellness. Clin J Oncol Nurs Apr 25: 210-214. doi: 10.1188/21.CJON.210-214
|
| [11] |
Singh A, Jha A, Purbey S (2020) Identification of measures affecting job satisfaction and levels of perceived stress and burnout among home health nurses of a developing Asian country. Hosp Top 99: 64-74. doi: 10.1080/00185868.2020.1830009
|
| [12] |
Drent M, Lower EE, De Vries J (2012) Sarcoidosis-associated fatigue. Eur Respir J 40: 255-263. doi: 10.1183/09031936.00002512
|
| [13] |
de Kleijn WP, De Vries J, Wijnen PAHM, et al. (2011) Minimal (clinically) important differences for the Fatigue Assessment Scale in sarcoidosis. Respir Med 105: 1388-1395. doi: 10.1016/j.rmed.2011.05.004
|
| [14] |
De Vries, Michielsen H, Van Heck GL, et al. (2004) Measuring fatigue in sarcoidosis: the Fatigue Assessment Scale (FAS). Br J Health Psychol 9: 279-291. doi: 10.1348/1359107041557048
|
| [15] | Alikari V, Fradelos E, Sachlas A, et al. (2016) Reliability and validity of the Greek version of «the Fatigue Assessment Scale». Arch Hell Med 33: 231-238. |
| [16] |
Kristensen TS, Borritz M, Villadsen E, et al. (2005) The Copenhagen Burnout Inventory: a new tool for the assessment of burnout. Work Stress 19: 192-207. doi: 10.1080/02678370500297720
|
| [17] |
Papaefstathiou E, Tsounis A, Malliarou M, et al. (2019) Translation and validation of the Copenhagen Burnout Inventory amongst Greek doctors. Health Psychol Res 7: 7678. doi: 10.4081/hpr.2019.7678
|
| [18] |
Henriksen L, Lukasse M (2016) Burnout among Norwegian midwives and the contribution of personal and work-related factors: a cross-sectional study. Sex Reprod Healthc 9: 42-47. doi: 10.1016/j.srhc.2016.08.001
|
| [19] |
Madsen IEH, Lange T, Borritz M, et al. (2015) Burnout as a risk factor for antidepressant treatment – a repeated measures time-to-event analysis of 2936 Danish human service workers. J Psychiatr Res 65: 47-52. doi: 10.1016/j.jpsychires.2015.04.004
|
| [20] | Tziallas D, Goutzias E, Konstantinidou E, et al. (2018) Quantitative and qualitative assessment of nurse staffing indicators across NHS public hospitals in Greece. Hell J Nurs 57: 420-449. |
| [21] |
Barker LM, Nussbaum MA (2011) Fatigue, performance and the work environment: a survey of registered nurses. J Adv Nurs 67: 1370-1382. doi: 10.1111/j.1365-2648.2010.05597.x
|
| [22] | Sagherian K, Steege LM, Cobb SJ, et al. (2020) Insomnia, fatigue and psychosocial well-being during COVID-19 pandemic: a cross-sectional survey of hospital nursing staff in the United States. J Clin Nurs . |
| [23] |
Geiger-Brown J, Trinkoff A, Rogers VE (2011) The impact of work schedules, home, and work demands on self-reported sleep in registered nurses. J Occup Environ Med 53: 303-307. doi: 10.1097/JOM.0b013e31820c3f87
|
| [24] |
Hirsch Allen AJ, Park JE, Adhami N, et al. (2014) Impact of work schedules on sleep duration of critical care nurses. Am J Crit Care 23: 290-295. doi: 10.4037/ajcc2014876
|
| [25] |
Johnson AL, Brown K, Weaver MT (2010) Sleep deprivation and psychomotor performance among night-shift nurses. AAOHN J 58: 147-154. doi: 10.1177/216507991005800404
|
| [26] |
Dorrian J, Tolley C, Lamond N, et al. (2008) Sleep and errors in a group of Australian hospital nurses at work and during the commute. Appl Ergon 39: 605-613. doi: 10.1016/j.apergo.2008.01.012
|
| [27] |
Tselebis A, Lekka D, Sikaras C, et al. (2020) Insomnia, perceived stress, and family support among nursing staff during the pandemic crisis. Healthcare 8: 434. doi: 10.3390/healthcare8040434
|
| [28] |
Liu Q, Luo D, Haase JE, et al. (2020) The experiences of healthcare providers during the COVID-19 crisis in China: a qualitative study. Lancet Glob Health 8: e790-e798. doi: 10.1016/S2214-109X(20)30204-7
|
| [29] |
Yifan T, Ying L, Chunhong G, et al. (2020) Symptom cluster of ICU nurses treating COVID-19 pneumonia patients in Wuhan, China. J Pain Symptom Manage 60: 48-53. doi: 10.1016/j.jpainsymman.2020.03.039
|
| [30] | Al-Masaeed M, Al-Soud M, Alkhlaifat E, et al. (2020) An investigation of the impacts of Covid-19 pandemic spread on nurses fatigue: an integrated literature review. World J Innov Res 9: 20-24. |
| [31] |
Luceño-Moreno L, Talavera-Velasco B, García-Albuerne Y, et al. (2020) Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in Spanish health personnel during the COVID-19 pandemic. Int J Environ Res Public Health 17: 5514. doi: 10.3390/ijerph17155514
|
| [32] |
Owuor RA, Mutungi K, Anyango R, et al. (2020) Prevalence of burnout among nurses in sub-Saharan Africa: a systematic review. JBI Evid Synth 18: 1189-1207. doi: 10.11124/JBISRIR-D-19-00170
|
| [33] |
Woo T, Ho R, Tang A, et al. (2020) Global prevalence of burnout symptoms among nurses: a systematic review and meta-analysis. J Psychiatr Res 123: 9-20. doi: 10.1016/j.jpsychires.2019.12.015
|
| [34] |
Galanis P, Vraka I, Fragkou D, et al. (2021) Nurses' burnout and associated risk factors during the COVID-19 pandemic: a systematic review and meta-analysis. J Adv Nurs 77: 3286-3302. doi: 10.1111/jan.14839
|
| [35] |
Sriharan A, West KJ, Almost J, et al. (2021) COVID-19-related occupational burnout and moral distress among nurses: a rapid scoping review. Nurs Leadersh 34: 7-19. doi: 10.12927/cjnl.2021.26459
|
| [36] |
Tselebis A, Moulou A, Ilias I (2001) Burnout versus depression and sense of coherence: study of Greek nursing staff. Nurs Health Sci 3: 69-71. doi: 10.1046/j.1442-2018.2001.00074.x
|
| [37] |
Bratis D, Tselebis A, Sikaras C, et al. (2009) Alexithymia and its association with burnout, depression and family support among Greek nursing staff. Hum Resour Health 7: 72. doi: 10.1186/1478-4491-7-72
|
| [38] |
Fernández-de-Las-Peñas C, Palacios-Ceña D, Gómez-Mayordomo V, et al. (2021) Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: a systematic review and meta-analysis. Eur J Intern Med 92: 55-70. doi: 10.1016/j.ejim.2021.06.009
|
| [39] |
Hou T, Zhang R, Song X, et al. (2020) Self-efficacy and fatigue among non-frontline health care workers during COVID-19 outbreak: a moderated mediation model of posttraumatic stress disorder symptoms and negative coping. PLoS One 15: e0243884. doi: 10.1371/journal.pone.0243884
|
| [40] |
Cui PP, Wang PP, Wang K, et al. (2021) Post-traumatic growth and influencing factors among frontline nurses fighting against COVID-19. Occup Environ Med 78: 129-135. doi: 10.1136/oemed-2020-106540
|
| [41] |
Heath C, Sommerfield A, Von Ungern-Sternberg BS (2020) Resilience strategies to manage psychological distress among healthcare workers during the COVID-19 pandemic: a narrative review. Anaesthesia 75: 1364-1371. doi: 10.1111/anae.15180
|
| [42] |
Kanekar A, Sharma M (2020) COVID-19 and mental well-being: guidance on the application of behavioral and positive well-being strategies. Healthcare 8: 336. doi: 10.3390/healthcare8030336
|
Figures(1) / Tables(6)

Christos Sikaras, Ioannis Ilias, Athanasios Tselebis, Argyro Pachi, Sofia Zyga, Maria Tsironi, Andrea Paola Rojas Gil, Aspasia Panagiotou. Nursing staff fatigue and burnout during the COVID-19 pandemic in Greece[J]. AIMS Public Health, 2022, 9(1): 94-105. doi: 10.3934/publichealth.2022008







 DownLoad:
DownLoad: