




Citation: Marie K. Fialkowski, Ashley Yamanaka, Lynne R. Wilkens, Kathryn L. Braun, Jean Butel, Reynolette Ettienne, Katalina McGlone, Shelley Remengesau, Julianne M. Power, Emihner Johnson, Daisy Gilmatam, Travis Fleming, Mark Acosta, Tayna Belyeu-Camacho, Moria Shomour, Cecilia Sigrah, Claudio Nigg, Rachel Novotny. Recruitment Strategies and Lessons Learned from the Children’s Healthy Living Program Prevalence Survey[J]. AIMS Public Health, 2016, 3(1): 140-157. doi: 10.3934/publichealth.2016.1.140
| [1] | Lars H. Wegner . Cotransport of water and solutes in plant membranes: The molecular basis, and physiological functions. AIMS Biophysics, 2017, 4(2): 192-209. doi: 10.3934/biophy.2017.2.192 |
| [2] | Nita R. Shah, Keni Vidilaseris, Henri Xhaard, Adrian Goldman . Integral membrane pyrophosphatases: a novel drug target for human pathogens?. AIMS Biophysics, 2016, 3(1): 171-194. doi: 10.3934/biophy.2016.1.171 |
| [3] | Mary Jane Beilby, Sabah Al Khazaaly . Re-modeling Chara action potential: II. The action potential form under salinity stress. AIMS Biophysics, 2017, 4(2): 298-315. doi: 10.3934/biophy.2017.2.298 |
| [4] | Alexander G. Volkov, Yuri B. Shtessel . Propagation of electrotonic potentials in plants: Experimental study and mathematical modeling. AIMS Biophysics, 2016, 3(3): 358-379. doi: 10.3934/biophy.2016.3.358 |
| [5] | Keleabetswe L. Mpye, Samantha Gildenhuys, Salerwe Mosebi . The effects of temperature on streptavidin-biotin binding using affinity isothermal titration calorimetry. AIMS Biophysics, 2020, 7(4): 236-247. doi: 10.3934/biophy.2020018 |
| [6] | Mary Jane Beilby, Sabah Al Khazaaly . Re-modeling Chara action potential: I. from Thiel model of Ca2+transient to action potential form. AIMS Biophysics, 2016, 3(3): 431-449. doi: 10.3934/biophy.2016.3.431 |
| [7] | Charles O. Nwamba, Ferdinand C. Chilaka, Ali Akbar Moosavi-Movahedi . Cation modulation of hemoglobin interaction with sodium n-dodecyl sulphate (SDS) iv: magnesium modulation at pH 7.20. AIMS Biophysics, 2016, 3(1): 146-170. doi: 10.3934/biophy.2016.1.146 |
| [8] | Ashwani Kumar Vashishtha, William H. Konigsberg . The effect of different divalent cations on the kinetics and fidelity of Bacillus stearothermophilus DNA polymerase. AIMS Biophysics, 2018, 5(2): 125-143. doi: 10.3934/biophy.2018.2.125 |
| [9] | Yoshiji Hantani, Hiroshi Imamura, Tsubasa Yamamoto, Akane Senga, Yuri Yamagami, Minoru Kato, Fusako Kawai, Masayuki Oda . Functional characterizations of polyethylene terephthalate-degrading cutinase-like enzyme Cut190 mutants using bis(2-hydroxyethyl) terephthalate as the model substrate. AIMS Biophysics, 2018, 5(4): 290-302. doi: 10.3934/biophy.2018.4.290 |
| [10] | Sudarat Tharad, Chontida Tangsongcharoen, Panadda Boonserm, José L. Toca-Herrera, Kanokporn Srisucharitpanit . Local conformations affect the histidine tag-Ni2+ binding affinity of BinA and BinB proteins. AIMS Biophysics, 2020, 7(3): 133-143. doi: 10.3934/biophy.2020011 |
| HKT | high-affinity potassium transporter; | NHX | sodium-proton exchanger; |
| NSCC | non-selective cation channels; | SOS1 | salt overly sensitive; |
| RBOH | respiratory burst oxidase homologue; | ROS | reactive oxygen species; |
| NO | nitric oxide; |
The macronutrient potassium (K+), which is the second most abundant mineral nutrient in plants after nitrogen, needs to be maintained within a range of 100-200 mM in the cytosol for efficient metabolic functioning [1,2]. Table 1summarizes the most important functions of K+ in higher plants. However, although sodium (Na+) is not an essential nutrient for plants, it can act as a substitute for K+ in relation to some functions, as has been demonstrated under certain K+-limiting conditions. For example, the decrease in nutrient uptake under salt stress conditions could be explained by the osmotic pressure exerted by the soil solution on the plant cell, leading to a reduction in water absorption and consequently nutrient acquisition [3,4]. The maintenance of ionic homeostasis is therefore necessary for plant salt resistance [5,6].To deal with such severe conditions, plants have developed different strategies, in particular, adequate uptake of K+ via discrimination between K+ and Na+ in order to maintain high cytosolic K+/Na+ ratios. The effect of salt stress on plant K+ nutrition has been the subject of numerous studies of both glycophytes and halophytes. These studies reveal that the presence of Na+ reduces K+ acquisition by inhibiting K+ transport in the aerial parts of the plant. Since Na+ ions are positively charged, they affect K+ absorption and related enzymatic activities in plant cells [7]. Therefore, the survival of plants depends on their ability to maintain homeostasis and transport of K+ across cell membranes [8]. Many studies indicate that relatively closed plant species have an evolutionary stage that enables them to develop adaptive mechanisms to cope with variations in environmental factors. The Brassicaceae family contains several species, the best known being the glycophyte Arabidopsis thaliana, the halophyte Thellungiellasalsuginea(formerly known as Thellungiella halophila) and, more recently, Cakile maritima. The distinct salt stress responses of these plant species reside in their ability to discriminate between K+ and Na+ and to maintain high K+/Na+ ratios despite intense competition from Na+. This review highlights the differential responses to salt stress in these three plant species, with particular emphasis on the potential involvement of reactive oxygen species (ROS) and nitric oxide (NO) in maintaining K+/Na+ homeostasis and their contribution to salt tolerance.
| Function |
| · Control of plant water status (stomatal activity) |
| · pH homeostasis, control of membrane electrical potential, and the regulation of cell osmotic pressure |
| · Increasing the rate of photosynthesis. |
| · Enhancing the loading and unloading of photosynthates into and out of the phloem. |
| · Activation of some enzymes |
| · Improve plant stress resistance |
 DownLoad: CSV
DownLoad: CSVThe ionic transport systems operating at the plasmalema and tonoplast play a crucial role in regulating the K+/Na+ ratio in the cell [9]. Under salt stress conditions, a series of transporters for Na+ and K+, called co-transporters, are activated to ensure high K+/Na+ ratios [5,10]. The common transporters for K+ and Na+ include the high affinity K+/Na+ transporter (HKT) [11], capable of co-transporting Na+ and K+ or only Na+ [12] and KT/HAK/KUP, K+(Na+)/H+ cation/proton antiporters (CPAs), and NHX proteins [13]. These transporters can transport 2 K+ ions over 1 Na+ ion. Potassium transporters are classified into two groups: cluster I transporters (AtHAK5, HvHAK1 and OsHAK1) and cluster II transporters (AtKUP4, HvHAK2, OsHAK2, OsHAK7 and OsHAK10). Several KT/HAK/KUP transporters may be involved in plant responses to salt stress [14]. A number of HvHAK1 cluster I transporters mitigate the influx of Na+ [15]. Others transporters, such as KUP-HAK, are known to be highly K+ selective, although the presence of Na+ at certain NaCl concentrations blocks these carriers [15]. For example, a 5 mM concentration of NaCl is sufficient to inhibit cluster II K+ transporters KUP1 responsible for mediating both high-and low-affinity K+ transport [16]. HAK5, a high-affinity K transporter and the largest contributor to K+ acquisition under salt stress and insufficient K+ availability conditions [17], can transport either K+ or Na+ and is often inhibited by Na+ [18], leading to sodium ion accumulation in plant cells [19]. These carriers are therefore important for the balance between K+ and Na+ and are efficiently regulated under salt stress conditions. In this context, many genes and transporters have been identified and shown to contribute significantly to the regulation of K+/Na+ ratios. As described above, the tolerance of plants to salt stress depends on their ability to regulate the expression of genes encoding several K+ transporters. This can be done by activating the high-affinity K+ transporter, particularly HAK5. According to the literature, many crops, as in the case of wheat, cultivated under saline conditions, are characterized by genetic regulation of K+/Na+ ratios, resulting in effective discrimination of K+ over Na+ at the xylem loading stage [20]. Recently, a study of tobacco has demonstrated that OsHAK5 expression in plant cells results in an increase in salt tolerance through the accumulation of K+, while Na+ content remains unaltered [21].Most K+ uptake systems, particularly non-selective cation channels (NSCCs) and high-affinity potassium transporters(HKTs), can be inhibited by Na+ [22].
Na+ enters the cell and plant via non-selective channels located at the plasma membrane. The activity of these channels induces a change in membrane potential and leads to its depolarization. Such modifications in membrane potential makes passive absorption of K+ through inward-rectifying K+ channels thermodynamically impossible, while an activation of outward-rectifying K+ channels occurs simultaneously, leading to a loss of K+. However, an increase in compatible solute synthesis ensures osmo-protection under these conditions, thus sharply reducing the pool of ATP and further decreasing K+ uptake [23]. Despite the fundamental role played by K+ in, for example, cell turgor pressure regulation [24,25,26], Na+ can substitute for K+ in functions such as osmotic adjustment, enzymatic activity and protein synthesis [27]. In terms of their chemical properties, Na+ and K+ actually share many physicochemical similarities which enable Na+ to compete with K+ at absorption sites and to impair K+ uptake. Thus, NaCl affects K+ status by reducing its uptake as a result of competition between Na+ and K+ for uptake sites as well as high-and low-affinity transporters [6,28,23] or by inducing K+ leakage due to membrane depolarization which activates outward-rectifying K+ channels [29]. According to Shabala and Cuin [23], NaCl can induce K+ deficiency via the two aforementioned mechanisms.
On the other hand, Na+ can have a beneficial impact on the halophytic plants and stimulate plant growth. Through the involvement of Na+ in osmoregulation, the energy used for osmoticum synthesis, such as proline in the form of adenosine triphosphate (ATP), contributes to the maintenance of plant growth. Moreover, large amounts of Na+, at levels similar or equal to those of K+, can be accumulated in the cell [30,31]. The antagonism between these two ions intensifies when the level of Na+ concentrations is excessive, as the accumulation of Na+ in plant tissue leads to a significant loss of K+ [32,33] through Na+, K+ and H+ antiporter activity. As described previously, under severe salinity conditions, the activation of outward-rectifying K+ channels, following the depolarization of the plasma membrane, leads to massive loss of K+ [23,34]. Given that salinity affects many regions around the world and can induce K+ deficiency [35], it is very important for plants to discriminate between Na+ and K+ and to maintain adequate K+/Na+ ratios.
Plant tolerance to salt stress is related to the maintenance of K+ homeostasis at both the cellular and whole plant levels mainly through high K+ selectivity over Na+ [36]. The maintenance of K+/Na+ ratios is therefore crucial for plant survival. Maintaining the lowest possible Na+/K+ ratios in the cytosol, which are regarded as a phytophysiological indicator of salt stress levels, is crucial to preserve vital cell functions [37,38]. Furthermore, the preservation of the intracellular K+/Na+ ratio, mainly in the cytoplasm, is a crucial factor in maintaining appropriate internal K+ concentrations and plant growth under salt stress conditions [9,39]. Thus, the cytoplasmic K+/Na+ ratio, considered to be an indicator of salt tolerance [23,40,41,42,43], enables plants to minimize Na+ accumulation in the cytosol and to avoid massive loss of K+ [32,44]. Plants tend to promote Na+ exclusion and K+ accumulation in tissues [25,45] in order to maintain a high cell K+/Na+ ratio [46] and to preserve vital metabolic pathways.
K+/Na+ homeostasis occurs through a series of Na+ and K + transporters located at the plasma membrane. To regulate cytosolic Na+ concentrations, plants tend to continuously exclude Na+. The principal mechanism of Na+ extrusion is mediated by power pumps located at the plasma membrane H+-ATPases [47].These pumps generate a H+ electrochemical gradient that transports ions and nutrients across the membrane [48]. H+-ATPases provide the plant cell with the energy to promote Na+/H+ antiporter activity involved in the extrusion of Na+ [48]. Once Na+ enters the plant cell, it needs to be accumulated in vacuoles to preserve the activity of several cytosolic enzymes. At the tonoplast, these Na+/H+ antiporters facilitate the sequestration of sodium ions in vacuoles and are encoded by AtNHX genes, as described in relation to Arabidopsis [49]. Vacuolar H+-pyrophosphatases, which are responsible for this process, have been identified in plants. Several channels and transporters mediating Na+ transport across the plasma membrane have also been identified [50]. The Ca2+-permeable nonselective cation channels (NSCCs) [6] and glutamate-like receptor (GLR) [51] families are among the most well known channels permeable to Na+ [50]. In Arabidopsis plants, 20 non-selective cation channels (NSCC) have been described [52]. Na+ flux is not only regulated at the root but also along its transport pathways to the aerial parts where a series of mainly KORC and NORC outward-rectifying K+ channels [53] and high-affinity K+ transporters (HKTs) play a crucial role in this process. The former are responsible for K+ xylem loading [54], while the latter facilitate the unloading of Na+ from the xylem sap [55,50,52]. In rice, Yang et al [56] found that OsHAK5 mediates high-affinity K+ acquisition and K+-regulated salt tolerance. In Arabidopsis, HAK5 expression was observed to increase under salt stress, reaching maximum transcript levels after 6 h of saline treatment [9]. Na+ and K+ transport is due to Na+/K+-symport activity which controls the transport of both ions. At the molecular level, the mechanisms involved in K+/Na+ uptake have been very well studied. The best known transporters, which contribute to K+ homeostasis, are the high-affinity HKT and HAK transporters [46,57]. SOS, a genetic locus essential for salt tolerance and potassium acquisition [58] in plants, regulates Na+ efflux across the plasma membrane to the soil solution. Other transporters play a crucial role in salt tolerance by mediating the K+/Na+ ratio. Some transporters such as OsHKT1;5, TaHKT1;5 and TmHKT; 4/5 are able to retrieve Na+ from the xylem in the xylem parenchyma, thus enabling the plant to avoid excessive Na+ accumulation, as in the case of SOS1 detected in T. salsuginea [59]. In wild-type Arabidopsis thaliana, the application of NaCl for a period of 6 days did not affect HAK5 transporter gene expression [60]. While Bassil et al. [39] observed an increase in HAK5 expression following the application of NaCl, which reached a peak after 6 h of treatment followed by a decrease after 24 h of treatment. In the same species, long term salt stress (16 days) reduced HAK5 expression [18]. Another high-affinity K+ transporter HKT, which is able to transport Na+, has been identified in plants. HKT1;1, which regulates Na+ penetration of plant cell roots and its distribution in the phloem, is crucial for salt stress tolerance in Arabidopsis [61]. Very recent new data indicate that the cation selectivity of HKT1 transporters is convertible by exchanging a single amino acid (Asp or Asn) in the 2nd pore-loop domain. In addition it was demonstrated that the amino acid serine in the 1st pore-loop domain is essential to facilitate Na+ uptake [62]. On the other hand, class II HKT transporters include the high-affinity Na+/K+ TaHKT2;1 transporter, which acts as a symporter under normal conditions and as a low‐affinity Na+ uniporter under salt stress conditions [63]. Recent studies of the model A. thaliana glycophyte plant have identifiedtwo high-affinity K+ transporters (AtHAK5 and AKT1), which are key elements in plant K+ uptake [64,65]. When K+ concentrations are highly limited [66,67,68] or under salt stress [69,19], AtHAK5 is the only system that ensures adequate K+ uptake, suggesting that Na+ can induce K+ deficiency [70]. In Arabidopsis, AtHAK5 is needed for K+ uptake when this nutrient is limited in the medium under saline conditions, although its expression is affected when Na+ concentrations are considerably higher in this glycophyte species [17]. Sun et al [71] attribute the variations in salinity tolerance between certain A. thaliana accessions to their ability to retain K+, with the tolerant accessions actually exhibiting low Na+/K+ ratios and high tissue K+ content [71]. These findings could be explained by significant up-regulation of genes coding for K+ transporters such as AtHAK5, AtCHX17 and AtKUP1 [71]. Recently, Alemán et al [22] have identified the conserved amino acid residue Phe130 in the HAK transporter family, which is required for AtHAK5 transporter selectivity. Moreover, the mutation Phe130Ser in the high-affinity Arabidopsis K+ transporter caused an increase in K+ uptake over Na+. The NHX protein, another K+/Na+ antiporter, is known to be expressed under salt stress conditions. In A. thaliana, overexpression of tomato antiporter LeNHX2 (NHX Class II) resulted in high sensitivity to K+ depletion [72].
Halophytes appear to be more effective in maintaining K+ transporter activity as compared to glycophytes. In T. salsuginea, salinity does not reduce K+ uptake via the high-affinity K+ transporter HAK5 to a lesser degree than in A. thaliana [69]. In this halophyte, two HKT genes, TsHKT1;1 and TsHKT1;2, encoding plasma membrane Na+/K+ co-transporters have been identified. One of these genes is induced and up-regulated at the transcriptional level under salt stress conditions [42]. This finding highlights the importance of TsHKT1 in the maintenance of K+ uptake and thus in the salt tolerance of this species. With regard to C. maritima, molecular studies are required to elucidate the transporters responsible for K+ homeostasis under high salinity stress conditions.
To overcome salt stress, plants need to maintain adequate nutrient uptake despite competition from Na+ and Cl− ions. It is critical for plants to maintain sufficient K+ uptake given the importance of this factor for plant survival. Thus, plants induce high K+-uptake systems such as HAK transporters.
A. thaliana is a model plant to investigate the physiology and biochemistry of plants under stressful and non-stressful conditions. A. thaliana, known to be sensitive to salt stress, prevents the accumulation of Na+ in its tissues through the extrusion of these ions in the external medium and in vacuoles. SOS1 is a transporter involved in Na+ extrusion at the roots. NHX proteins located at the tonoplast are responsible for Na+ accumulation in the vacuole, thus making Arabidopsis plants salinity-tolerant [73]. On the other hand, Thellungiella salsuginea (2n=14), which is relatively close to A. thaliana (2n=10), presents the characteristics of a halophytic model plant. This plant’s tolerance to salinity is due to its high capacity to prevent Na+ accumulation in shoots. This species has thus been found to be more efficient in accumulating less Na+ in its aerial parts as compared to A. thaliana[74]. Cakile maritima (2n=18), another plant which is relatively close to A. thaliana [75], is an excellent model for investigating salinity tolerance mechanisms in halophytic species. This plant tolerates high levels of salt even during germination and presents a germination rate of approximately 75% at 200 mM NaCl [76]. Unlike A. thaliana and T. salsuginea, C. maritima is able to accumulate Na+ in shoots, which it uses for osmotic adjustments and to maintain growth activity even at high salinity levels [36,77]. Competition from Na+ for K+ uptake is offset by high K+ selectivity and use efficiency levels [78].
In A. thaliana plants, Na+ can enter roots without difficulty due to the presence of various non-selective cation channels [6]. These channels are characterized by very low selectivity for K+ over Na+ [79], resulting in very high Na+/K+ ratios. Despite their intolerance to salt stress, glycophytes have developed saline resistance mechanisms, especially by maintaining high K+/Na+ ratios via the activation of ionic transport systems and the establishment of electrochemical gradients across the membrane [80]. Subjecting A. thaliana to 400 mM NaCl for 72 h has recently been found to maintain an ionic balance in roots, which results in high Na+/K+ ratios [81]. Unlike glycophytes, halophytes are able to support salinity levels of up to 1000 mM NaCl, with, for example, 800 mM NaCl in the case of the halophyte Sesuvium portulacastrum [82] and up to 500 mM NaCl in the case of Cakile maritima [83]. According to Newell [7], the ability of halophytes to tolerate high salinity levels is due to the compartmentalization of Na+ in vacuoles, the accumulation of osmolytes such as proline and the maintenance of constant K+ tissue concentrations via the induction of several transporters with high K+ selectivity resulting in adequate K+/Na+ ratios [75]. Given the interaction between K+ and Na+, the halophytes are characterized by high K+ discrimination rates and are able to maintain K+ homeostasis and transport across cellular membranes [8]. Thellungiella salsuginea is considered to be a halophytic model plant due to its high tolerance to several abiotic stresses [84,85,86], which explains its status as an extremophile plant, with its tolerance to salt stress being related to its K+ retention capacity [42,87]. Thellungiella salsuginea is able to regulate the uptake of K+ which is acquired very efficiently from the medium, thus enabling this species to maintain high K+/Na+ ratios, which is not the case for A. thaliana [88,89,90]. T. salsuginea and A. thaliana respond differently to salt stress in terms of K+ content, with the highest shoot K+ content being found in the halophytes rather than in the glycophyte. Moreover, although shoot K+ content is decreased by salt stress in A. thaliana (10-20%), it is increased by this type of stress in T. salsuginea (10-50%). This behavior is explained by the ability of T. salsuginea to accumulate less Na+ and more K+ than A. thaliana under salt stress conditions due to selective K+/Na+ channels located at the plasma membrane [91]. With regard to K+/Na+ selectivity, major differences between A. thaliana and T. salsuginea plants have been observed. In fact, despite the presence of large Na+ concentrations in the medium, the halophyte species exhibits the largest K+ concentrations and highest K+/Na+ ratios, as documented by Ghars et al [74] and Bailey et al [75]. This is due to the capacity of the halophyte to prevent Na+ accumulation in its tissues [91] and to maintain high K+-affinity transporter HAK5 activity as compared to the glycophyte species [69].
The voltage-independent channels at the root plasma membrane are extremely potassium-selective and contribute to more efficient K+ uptake in T. salsuginea than in A. thaliana [91]. In A. thaliana, a negative correlation between Na+ and K+ was found, while a positive correlation was detected in T. salsuginea [91]. The authors attribute their findings to the fact that both species differ in terms of their Na+ and K+ transport pathways. While intense competition between Na+ and K+ was observed in A. thaliana under salt stress conditions, this was not the case for T. salsuginea. Following the application of 100 mM NaCl, Volkov et al [91] detected significant differences between A. thaliana and T. salsuginea in terms of Na+ and K+ uptake and their distribution in shoots in these two species. T. salsuginea exhibits a specific behavior pattern following the saline application, and when the medium is deprived of salt, its epidermal cells acquire large amounts of K+. Salt stress treatment significantly modified the distribution of K+ in cells, with the sharp decrease in epidermal K+ concentrations leading to an increase in bulk K+ concentrations. This modification enabled T. salsuginea to maintain high K+/Na+ ratios in mesophyll cells, a pattern not observed in A. thaliana which is able to accumulate more K+ than Na+ during the first 25 h of salt treatment. These authors point to the existence of two different pathways for K+ and Na+ permeability to explain this behavior. T. salsuginea presents higher selectivity for K+ over Na+ at both the inward-and outward-rectifying K channel K+ uptake sites as compared to A. thaliana [91].They point out that the adaptation of T. salsuginea to salt stress is linked to high K+/Na+ selectivity in roots and to the exchange of K+ over Na+ between epidermal and mesophyll cells. More recently, Volkov and Amtmann [90] demonstrate that T. salsuginea maintains K+ uptake despite the presence of salt in the medium due to the slight depolarization generated, thus making the plasma membrane poorly permeable to Na+ under these conditions.
To gain a greater insight into high K+ selectivity in T. salsuginea, Bailey et al [75] studied the effect of low and high salinity levels on K+ content in both A. thaliana and T. salsuginea and found that treatment with 100 mM NaCl for 72 h during a period of 6 weeks caused a very rapid loss of K+ in the glycophyte due to an increase in Na+ uptake, resulting in high Na+/K+ ratios. By contrast, the halophyte can maintain the balance between K+ and Na+, which is essential to enable T. salsuginea to survive under salt stress conditions. The tolerance of this species to salinity appears to be related to the maintenance of K+ homeostasis via the discrimination between Na+ and K+ which results in low K+/Na+ ratios. Coskun et al [46] have also studied the responses of A. thaliana and T. salsuginea to salt stress, with particular emphasis on K+/Na+ homeostasis. Thus, while salinity significantly reduced K+/Na+ ratios in both Brassicaceae species, K+/Na+ values were significantly higher in T. salsugineathan in A. thaliana, with larger saline concentrations being observed in the medium. The K+/Na+ ratio was 2-fold higher in T. salsuginea following the application of 50 and 75 mM NaCl and 4-fold higher after treatment with 100, 150 and 200 mM NaCl. Coskun et al [46] have also demonstrated that K+/Na+ levels remain significantly higher in the halophyte species after treatment with 500 mM NaCl as compared to the glycophyte species treated with 200 mM NaCl. They also point out that the application of 50, 100, 150 and 200 mM NaCl did not affect K+ concentration levels in T. salsuginea, while a decrease of 40% was observed in A. thaliana after treatment with 100 mM NaCl. Under severe salinity conditions (300-500 mM NaCl), K+ content levels in the halophyte species were similar to those in the glycophyte species cultivated under control conditions. These differences between the two species could be explained by the highly K+/Na+-selective channels found in T. salsuginea as compared to A. thaliana [91].
Cakile maritima, an annual C3 species commonly found on sandy beaches around the world, is of great ecological interest mainly due to its soil fixation capacity. This species is capable of maintaining highly selective uptake of K+ as against Na+ [83] and of increasing K+ use efficiency [78]. These authors attribute this behavior to a Na+ flux regulation mechanism which occurs at the intracellular level and contributes to salt tolerance in this species. In fact, C. maritima preserves its K+ content by allocating Na+ to the vacuole and by preventing its accumulation in the cytoplasm [36]. As this behavior is typical of halophyte species, Na+ can be used as an osmoticum to carry out osmotic adjustments [92] and also as a signal to enable the plant to prevent ionic toxicity [93]. Na+ sequestration in C. maritima is caused by Na+/H+ tonoplastic antiport activity which exchanges the Na+ ion over a H+ proton [94].C. maritima is very K+-selective as compared to A. thaliana [94]. These authors suggest that efficient transport systems are present in the halophyte species which are responsible for the discrimination of K+ over Na+ to improve ionic status and to preserve crucial metabolic functions.
Indeed, a Na+/H+ exchange is necessary for the purposes of plant salinity tolerance. Many intracellular NHX transporters, which are responsible for Na+ accumulation in vacuoles, have been identified and are the first family of cation/H+ exchangers to be investigated in plant tissues [95,96]. Further molecular and genetic studies are required to investigate the capacity of these species to maintain K+/Na+ homeostasis when subjected to salinity. On the other hand, very recently, a new transporter called KUP7 has been described in Arabidopsis roots; this appears to be crucial for K+ uptake and might also be involved in K+ transport into xylem sap, affecting K+ translocation from root to shoot, especially under K+-limited conditions [97].
Figure 1 shows a simplified flowchart model to compare response mechanisms under salinity stress in glycophyte (Arabidopsis thaliana) and halophyte (Thellungiellasalsuginea and Cakile maritima) plants to regulate K+/Na+ ratios.
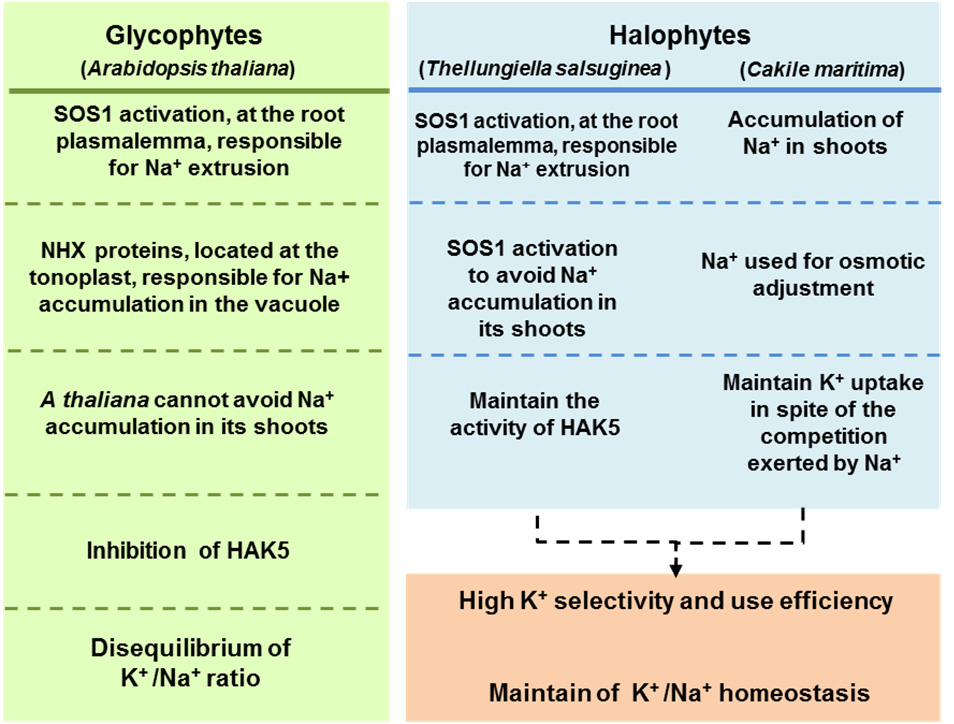 Figure 1. Comparative flowchart model of the mechanism of response under salinity stress in glycophyte (Arabidopsis thaliana) and halophyte (Thellungiella salsuginea and Cakile maritima) plants to regulate K+/Na+ ratio. HAK5, High Affinity K+ transporter 5. NHX, Sodium-Proton exchanger. SOS1, Salt Overly Sensitive.
Figure 1. Comparative flowchart model of the mechanism of response under salinity stress in glycophyte (Arabidopsis thaliana) and halophyte (Thellungiella salsuginea and Cakile maritima) plants to regulate K+/Na+ ratio. HAK5, High Affinity K+ transporter 5. NHX, Sodium-Proton exchanger. SOS1, Salt Overly Sensitive.A strong link between ROS production and the mediation of K+/Na+ homeostasis has been observed in many plant species [98]. In Populus euphratica, NaCl increases the production of hydrogen peroxide (H2O2), which contributes to the preservation of the K+/Na+ balance and high antioxidant capacity, enabling this species to regulate its ionic status and antioxidant defense system under long term salt stress conditions [99]. Under salt stress, ROS production increases and acts as a signal to maintain Na+/K+ homeostasis. ROS actually play an important role in regulating the Na+/K+ ratio, as ROS content increases significantly under salinity stress [9]. ROS are therefore also involved in regulating HAK5 expression [100,101]. Other studies have demonstrated that ROS also control ionic channel activity [102]. To cope with salinity, plants have developed specific strategies, which include both the regulation of ionic homeostasis and detoxification of ROS under these environmental conditions [10].
The role of ROS in maintaining K+/Na+ homeostasis is well documented. Ho and Tsay [103] have shown that, under K+ deficiency conditions, ethylene production increases and stimulates the generation of ROS in A. thaliana. The increased production of ROS contributes to the regulation of K+ transporters, particularly the high-affinity potassium transporter HAK5 which is induced under these conditions. Thus, ROS are crucial for generating K+ starvation responses at the root level via the regulation of AtHAK5 gene expression encoding a high-affinity K+ transporter induced under low K+ supply conditions [104].
In this context, a common response to ROS accumulation is the activation of the defense system which includes a diverse range of antioxidant enzymes, especially the superoxide dismutase (SOD), representing the first line of defense against oxidative stress [77]. In A. thaliana, a total of seven SOD isozymes has been identified which are differentially regulated in response to oxidative damage [105]. The manipulation of the Arabidopsis genome provides new mutants that are tolerant to salt stress. For example, the pst1 mutant presents higher levels of SOD activity under extremely stressful saline conditions as compared to the wild-type plant [106]. In T. salsuginea, four SOD isozymes have been described [107], and, surprisingly, a total of ten SOD isozymes have been found to be differentially expressed during development and under long term salt stress in the halophyte C. maritima [77] (Table 2). The antioxidant α-tocopherol can also contribute to the maintenance of cellular Na+/K+ homeostasis [108]. Thus, Arabidopsis mutants vte1 and vte4, characterized by tocopherol loss, have been shown to be sensitive to salt stress due to a sharp decrease in their growth and the generation of high oxidative stress levels under saline conditions.
| Plant species | MnSOD | FeSOD | CuZnSOD | Ref. |
| C. maritima | 2 | 1 | 7 | 77 |
| T. salsuginea | 1 | 1 | 2 | 107 |
| A. thaliana | 1 | 3 | 3 | 120 |
DownLoad: CSVOn the other hand, the Arabidopsis double mutants of plant membrane-bound NADPH oxidases (NOXs), also known as respiratory burst oxidase homologues (RBOHs), specifically atrbohD1/F1 and atrbohD2/F2, in which the generation of the superoxide radical (O2−) is considerably inhibited, have been found to be much more sensitive to NaCl treatments than wild-type plants. These two Arabidopsis double mutants also have much higher Na+ content, lower K+ content and consequently higher Na+/K+ ratios than WT mutants under salt stress conditions [109]. These results strongly suggest that ROS generated by both AtrbohD and AtrbohF act as signal molecules to regulate Na+/K+ homeostasis, thus improving the salt tolerance of Arabidopsis plants [109]. Studies of H2O2 signaling in halophytes and glycophytes demonstrate that the kinetics of this process are faster in halophytes than in glycophytes [110]. In the halophyte Cakile maritima, H2O2 reached a peak in leaves 4 hours after salt stress treatment and was maintained after 16 h and 24 h of treatment before decreasing after 72 h. On the other hand, in A. thaliana, the H2O2 levels detected in leaves continued to be higher even after 72 h of treatment [94].
Nitric oxide (NO) is a free radical molecule involved in a wide spectrum of plant processes [111]. It contributes to salt stress tolerance by acting as a signal molecule when produced in small quantities; even when accumulated in the plant cell, NO enhances anti-oxidative responses by stimulating its special scavengers [112,113]. Moreover, some studies show that NO helps to maintain the K+/Na+ equilibrium in Populus euphratica under long-term salt stress [99]. It has also been found to contribute to K+ homeostasis under salt stress by regulating both the Na+/K+ ratio and H+-ATPases located at the plasma membrane [114] through its involvement in establishing a proton gradient generated by H+-ATPase (H+-PPase) activity, thus contributing to K+/Na+ homeostasis [115].
Up to now, little information has been available on how NO regulates K+ homeostasis under salt stress in Brassicaceae species, especially in relation to the model plant A. thaliana. However, a recent study [116] has pointed out that NO is involved in regulating K+ absorption and Na+/K+ ratios under salt stress in A. thaliana. These authors have demonstrated that NO lowers A. thaliana K+ absorption by repressing the AKT1 channel function. Thus, in A. thaliana exposed to salt stress, NO up-regulates K+ absorption and the Na+ to K+ ratio through its impact on the gene encoded for vitamin B6; this leads to an excessive accumulation of vitamin B6 (PLP) which is responsible for the repression of K+ channel AKT1 activity, resulting in a reduction in K+ uptake by roots [116]. Arabidopsis mutant (Atnoa1) plants, with reduced endogenous levels of NO, display higher Na+ to K+ ratios in shoots than wild-type plants due to enhanced Na+ accumulation and reduced K+ accumulation when plants are exposed to NaCl, suggesting that NO is involved in maintaining K+/Na+ homeostasis [117].
The molecular connections, which explain how plants exposed to salinity rapidly accumulate NO and reorganize Na+ and K+ content, have begun to be elucidated. Thus, using an A. thalina mutant called sno1 (sensitive to nitric oxide 1), which is allelic to the well-known mutant sos4 (salt overly sensitive 4), NO has been shown to be capable of reducing K+ channel AKT1-mediated plant K+ uptake by modulating vitamin B6 biosynthesis [116]. However, in the halophyte Kandelia obovata, exposed to exogenous applications of NO, NO has been demonstrated to greatly contribute to the K+/Na+ balance under high salinity conditions by activating the AKT1-type K+ channel and Na+/H+ antiporter, which are critical components in the K+/Na+ transport system [118].
The tolerance of plants to salt stress resides in their ability to maintain ion homeostasis despite competition from sodium ions. Plants need to preserve K+ uptake under saline conditions in order to maintain their biological activity. Salt-tolerant plants are capable of maintaining high K+/Na+ ratios, which are later up-regulated at different levels through hormonal control, nitric oxide, ROS production, the antioxidant system and gene expression. A comparative study of the A. thaliana, T. salsuginea and C. maritima Brassicaceae species reveals that halophytes are more efficient in terms of salt resistance due to their ability to maintain K+ uptake and high K+/Na+ ratios.
We thank Dr María P. Rodríguez-Rosales for her constructive comments of this manuscript. Research in FJC laboratory is supported by an ERDF grant co-financed by the Ministry of Economy and Competitiveness (AGL2015-65104-P) and the Junta de Andalucía (group BIO192) in Spain.
The authors declare that there are no conflicts of interest related to this study.
| [1] | Ng M, Fleming T, Robinson M, et al. (2014) Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384(9945): 766-81. |
| [2] | Hawley NL and McGarvey ST. (2015) Obesity and diabetes in Pacific Islanders: the current burden and the need for urgent action. Curr Diab Rep 15(5): 29. |
| [3] | McLennan AK and Ulijaszek SJ. (2015) Obesity emergence in the Pacific islands: why understanding colonial history and social change is important. Public health nutrition 18(08): 1499-1505. |
| [4] | Pacific Islands Health Officers Association, Board Resolution #48-01: The burden of non-communicable diseases. 2010, Pacific Islands Health Officers Association: Honolulu, HI. |
| [5] | Must A. (2003) Does overweight in childhood have an impact on adult health? Nutr Rev 61(4): 139-42. |
| [6] | Berenson GS, Srinivasan SR, Bao W, et al. (1998) Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults. The Bogulasa Heart Study. N Engl J Med 338(23): 1650-1656. |
| [7] | Lauer RM and Clarke WR. (1989) Childhood risk factors for high adult blood pressure: the Muscatine Study. Pediatrics 84(4): 633-641. |
| [8] | Lauer RM, Lee J, and Clarke WR. (1988) Factors affecting the relationship between childhood and adult cholesterol levels: the Muscatine Study. Pediatrics 82(3): 309-318. |
| [9] | Association AD. (2000) Type 2 Diabetes in Children and Adolescents. Pediatrics 105(3): 671-680. |
| [10] | Novotny R. (2006) Nutrition and health status of children in the CNMI, in Preliminary Report: June 24, 2006. University of Hawaii, Northern Marianas College, Department of Public Health. |
| [11] | Novotny R, Coleman P, Tenorio L, et al. (2007) Breastfeeding is associated with lower body mass index among children of the Commonwealth of the Northern Mariana Islands. J Am Diet Assoc 107(10): 1743-6. |
| [12] | Guerrero RTL, Paulino YC, Novotny R, et al. (2008) Diet and obesity among Chamorro and Filipino adults on Guam. Asia Pac J Clin Nutr 17(2): 216-22. |
| [13] | Novotny R, Vijayadeva V, Grove J, et al. (2012) Dietary intake among Native Hawaiian, Filipino, and White children and caregivers in Hawai'i. Hawaii J Med Public Health 71(12): 353-8. |
| [14] | Derrickson J, Tanaka D, and Novotny R. (1997) Heights and weights of Head Start preschool children in Hawaii. J Am Diet Assoc 97(12): 1424-1426. |
| [15] | Paulino YC, Coleman P, Davison NH, et al. (2008) Nutritional characteristics and body mass index of children in the Commonwealth of the Northern Mariana Islands. J Am Diet Assoc 108(12): 2100-2104. |
| [16] | Novotny R, Williams AE, Vinoya AC, et al. (2009) US acculturation, food intake, and obesity among Asian-Pacific hotel workers. J Am Diet Assoc 109(10): 1712-1718. |
| [17] | Novotny R, Chen C, Williams AE, et al. (2012) US acculturation is associated with health behaviors and obesity, but not their change, with a hotel-based intervention among Asian-Pacific Islanders. J Acad Nutr Diet 112(5): 649-656. |
| [18] | Nigg C, Maddock J, Yamauchi J et al. (2005) The healthy Hawaii initiative: A social ecological approach promoting healthy communities. Am J Health Promot 19(4): 310-313. |
| [19] | Iversen CS, Nigg C, and Titchenal CA. (2011) The impact of an elementary after-school nutrition and physical activity program on children's fruit and vegetable intake, physical activity, and body mass index: Fun 5. Hawaii Med J 70(7 Suppl 1): 37-41. |
| [20] | Novotny R, Fialkowski MK, Li F, et al. (2015) Systematic review of prevalence of young child overweight and obesity in the United States-Affiliated Pacific region compared with the 48 contiguous states: The Children's Healthy Living Program. Am J Public Health 105(1): e22-e35. |
| [21] | Murphy SP. (2003) Collection and analysis of intake data from the integrated survey. J Nutr 133(2): p. 585S-589S. |
| [22] | Peterkin BB. (1981) Nationwide food consumption survey, 1977-1978. Prog Clin Biol Res 67: 59-69. |
| [23] | U.S. Central Intelligence Agency. The World Factbook. 2015. Available from: https://www.cia.gov/library/publications/the-world-factbook/. |
| [24] | U.S. Census Bureau, United States Census 2010. 2010: Jeffersonville, IN. |
| [25] | Central Intelligence Agency. Palau. World Fact Book, 2014. Available from: https://www.cia.gov/library/publications/the-world-factbook/geos/ps.html. |
| [26] | Novotny R, Areta A, Bersamin A, et al. (2013) The Pacific way to child wellness: the Children’s Healthy Living Program for remote underserved minority populations of the Pacific region (CHL). Hawaii J Med Public Health 72(11): 406-408. |
| [27] | Wilken LR, Novotny R, Fialkowski MK, et al. (2013) Children's healthy living (CHL) program for remote underserved minority populations in the pacific region: rationale and design of a community randomized trial to prevent early childhood obesity. BMC Public Health 13(1): 944. |
| [28] | Hooks PC, Tsong Y, Baranowski T, et al. (1988) Recruitment strategies for multiethnic family and community health research. Family and Community Health 11(1): 48-59. |
| [29] | Loxton D, Powers J, Anderson AE, et al. (2015) Online and Offline Recruitment of Young Women for a Longitudinal Health Survey: Findings From the Australian Longitudinal Study on Women's Health 1989-95 Cohort. J Med Internet Res 17(5): e109. |
| [30] | Markert J, Alff F, Zschaler S, et al. (2013) Prevention of childhood obesity: recruiting strategies via local paediatricians and study protocol for a telephone-based counselling programme. Obes Res Clin Pract 7(6): e476-e486. |
| [31] | Greany M, Lees FD, Nigg C, et al. (2006) Recruiting and Retaining Older Adults for Health Promotion Research: The Experience of the SENIOR Project. Journal of Nutrition for the Elderly 25(3-4): 3-22. |
| [32] | Dilworth-Anderson P, Thaker S, and Burke JM. (2005) Recruitment strategies for studying dementia in later life among diverse cultural groups. Alzheimer Dis Assoc Disord 19(4): 256-260. |
| [33] | Levkoff S and Sanchez H. (2003) Lessons learned about minority recruitment and retention from the Centers on Minority Aging and Health Promotion. Gerontologist 43(1): 18-26. |
| [34] | Saunders SD, Greaney ML, Lees FD, et al. Achieving recruitment goals through community partnerships: the SENIOR Project. Fam Community Health 26(3): 194-202. |
| [35] | Warren-Findlow J, Prohaska TR, and Freedman D. (2003) Challenges and opportunities in recruiting and retaining underrepresented populations into health promotion research. Gerontologist 43 Spec No 1: 37-46. |
| [36] | Luebbert R and Perez A. (2015) Barriers to Clinical Research Participation Among African Americans. J Transcult Nurs 1043659615575578. |
| [37] | Brown SD, Partee PN, Feng J, et al. (2015) Outreach to diversify clinical trial participation: A randomized recruitment study. Clin Trials 12(3): 205-211. |
| [38] | Recruitment for clinical trials: the Lipid Research Clinics Coronary Primary Prevention Trial experience. Its implications for future trials. Circulation, 1982. 66(6 Pt 2): IV1-78. |
| [39] | Corbie-Smith G, Thomas SB, and St George DM. (2002) Distrust, race, and research. Arch Intern Med 162(21): 2458-2463. |
| [40] | Roberson NL. (1994) Clinical trial participation. Viewpoints from racial/ethnic groups. Cancer 74(9 Suppl): 2687-2691. |
| [41] | Heller C, Balls-Berry JE, Nery JD, et al. (2014) Strategies addressing barriers to clinical trial enrollment of underrepresented populations: a systematic review. Contemp Clin Trials 39(2): 169-182. |
| [42] | Wasem C. (2004) U.S. affiliated Pacific basin jurisdictions: Legal, geographic, and demographic information. Office of Pacific Health & Human Services - Region IX Office of the Regional Health Administrator, HHS: Honolulu, HI. |
| [43] | Li F, Wilkens L, Novotny R, et al. (2014) Anthropometric standardization in the U.S. Affiliated Pacific: The Children’S Healthy Living Program (1024.6). The FASEB Journal 28(1 Supplement). |
| [44] | Novotny R, Li F, Fialkowski M, et al. (2015) Child Obesity and Acanthosis Nigricans in the Children's Healthy Living Program (CHL). The FASEB Journal 29(1 Supplement): 902-909. |
| [45] | Boushey C, Yonemori K, Novotny R, et al. (2015) Intakes of key dietary indicators among children 2-8 years participating in the Children's Healthy Living (CHL) Program. FASEB J 29(1 Supplement): 381-1. |
| [46] | Ettienne R, Boushey C, Yonemori K, et al. (2015) Young children's physical activities (PA) in the US Affiliated Pacific (USAP): The Children's Healthy Living (CHL) Program. The FASEB Journal 29(1 Supplement): 732-10. |
| [47] | Li F, Nigg C, McGlone K, et al. (2015) Young children's screen time and obesity in the US Affiliated Pacific: The Children's Healthy Living Program. The FASEB Journal 29(1 Supplement): 902-921. |
| [48] | Li F, Novotny R, Fialkowski M, et al. (2015) Determinants of young children's sleep duration in the US Affiliated Pacific: The Children's Healthy Living Program. The FASEB Journal 29(1 Supplement): 902-22. |
| [49] | Schulz AJ, Parker EA, Israel BA, et al. (1998) Conducting a participatory community-based survey for a community health intervention on Detroit's east side. J Public Health Manag Pract 4(2): 10-24. |
| [50] |
Israel BA, Schulz AJ, Parker EA, et al. (1998) Review of community-based research: assessing partnership approaches to improve public health. Annu Rev Public Health 19: 173-202. doi: 10.1146/annurev.publhealth.19.1.173

|
| [51] | Palafox NA, Buenconsejo-Lum L, Rikion S, et al. (2002) Improving health outcomes in diverse populations: competency in cross-cultural research with indigenous Pacific islander populations. Ethn Health 7(4): 279-285. |
| 1. | Nicolle Louise Ferreira Barros, Deyvid Novaes Marques, Lorene Bianca Araújo Tadaiesky, Cláudia Regina Batista de Souza, Halophytes and other molecular strategies for the generation of salt-tolerant crops, 2021, 162, 09819428, 581, 10.1016/j.plaphy.2021.03.028 | |
| 2. | Hayet Houmani, Marta Rodríguez-Ruiz, José M. Palma, Francisco J. Corpas, Mechanical wounding promotes local and long distance response in the halophyte Cakile maritima through the involvement of the ROS and RNS metabolism, 2018, 74, 10898603, 93, 10.1016/j.niox.2017.06.008 | |
| 3. | Antonio Sánchez-McSweeney, Salvador González-Gordo, María Nieves Aranda-Sicilia, María Pilar Rodríguez-Rosales, Kees Venema, José M. Palma, Francisco J. Corpas, Loss of function of the chloroplast membrane K+/H+ antiporters AtKEA1 and AtKEA2 alters the ROS and NO metabolism but promotes drought stress resilience, 2021, 160, 09819428, 106, 10.1016/j.plaphy.2021.01.010 | |
| 4. | Nazila Azhar, Nana Su, Lana Shabala, Sergey Shabala, Exogenously Applied 24-Epibrassinolide (EBL) Ameliorates Detrimental Effects of Salinity by Reducing K+ Efflux via Depolarization-Activated K+ Channels, 2017, 58, 0032-0781, 802, 10.1093/pcp/pcx026 | |
| 5. | Somayeh Faghih, Abdolkarim Zarei, Cyrus Ghobadi, Positive effects of plant growth regulators on physiology responses of Fragaria × ananassa cv. ‘Camarosa’ under salt stress, 2019, 19, 1553-8362, 104, 10.1080/15538362.2018.1462291 | |
| 6. | Silvia Del Vecchio, Marco Porceddu, Edy Fantinato, Alicia T. R. Acosta, Gabriella Buffa, Gianluigi Bacchetta, Germination responses of Mediterranean populations of Cakile maritima to light, salinity and temperature, 2018, 53, 1211-9520, 417, 10.1007/s12224-018-9332-5 | |
| 7. | A. Raza, J. Tabassum, M. S. Mubarik, S. Anwar, N. Zahra, Y. Sharif, M. B. Hafeez, C. Zhang, F. J. Corpas, H. Chen, M.H. Siddiqui, Hydrogen sulfide: an emerging component against abiotic stress in plants, 2022, 24, 1435-8603, 540, 10.1111/plb.13368 | |
| 8. | Ines Petrić, Dunja Šamec, Erna Karalija, Branka Salopek-Sondi, Beneficial Microbes and Molecules for Mitigation of Soil Salinity in Brassica Species: A Review, 2022, 6, 2571-8789, 18, 10.3390/soilsystems6010018 | |
| 9. | Havza Imtiaz, Anayat Rasool Mir, Francisco J. Corpas, Shamsul Hayat, Impact of potassium starvation on the uptake, transportation, photosynthesis, and abiotic stress tolerance, 2023, 99, 0167-6903, 429, 10.1007/s10725-022-00925-7 | |
| 10. | Barbara Hawrylak-Nowak, 2022, Chapter 6, 978-3-031-07062-4, 91, 10.1007/978-3-031-07063-1_6 | |
| 11. | Ricardo Gil-Ortiz, Miguel Ángel Naranjo, Sergio Atares, Oscar Vicente, Antioxidant Responses of Water-Stressed Cherry Tomato Plants to Natural Biostimulants, 2023, 13, 2073-4395, 2314, 10.3390/agronomy13092314 |

Marie K. Fialkowski, Ashley Yamanaka, Lynne R. Wilkens, Kathryn L. Braun, Jean Butel, Reynolette Ettienne, Katalina McGlone, Shelley Remengesau, Julianne M. Power, Emihner Johnson, Daisy Gilmatam, Travis Fleming, Mark Acosta, Tayna Belyeu-Camacho, Moria Shomour, Cecilia Sigrah, Claudio Nigg, Rachel Novotny. Recruitment Strategies and Lessons Learned from the Children’s Healthy Living Program Prevalence Survey[J]. AIMS Public Health, 2016, 3(1): 140-157. doi: 10.3934/publichealth.2016.1.140

| Function |
| · Control of plant water status (stomatal activity) |
| · pH homeostasis, control of membrane electrical potential, and the regulation of cell osmotic pressure |
| · Increasing the rate of photosynthesis. |
| · Enhancing the loading and unloading of photosynthates into and out of the phloem. |
| · Activation of some enzymes |
| · Improve plant stress resistance |
DownLoad: CSV| Plant species | MnSOD | FeSOD | CuZnSOD | Ref. |
| C. maritima | 2 | 1 | 7 | 77 |
| T. salsuginea | 1 | 1 | 2 | 107 |
| A. thaliana | 1 | 3 | 3 | 120 |
DownLoad: CSV| Function |
| · Control of plant water status (stomatal activity) |
| · pH homeostasis, control of membrane electrical potential, and the regulation of cell osmotic pressure |
| · Increasing the rate of photosynthesis. |
| · Enhancing the loading and unloading of photosynthates into and out of the phloem. |
| · Activation of some enzymes |
| · Improve plant stress resistance |
| Plant species | MnSOD | FeSOD | CuZnSOD | Ref. |
| C. maritima | 2 | 1 | 7 | 77 |
| T. salsuginea | 1 | 1 | 2 | 107 |
| A. thaliana | 1 | 3 | 3 | 120 |
