Objective: To examine the associations between social and behavioral determinants of health (SBDH) and frailty among older adults using an existing Omaha System dataset collected in the community.
Design: Secondary exploratory data analysis.
Setting: An existing dataset of home health records from a Midwestern region, including Omaha System problems, interventions, and Knowledge (K), Behavior (B), and Status (S) outcomes.
Participants: Older adults (n = 1,618) that were 63.7% female with an average age of 80.1 years (SD = 7.6).
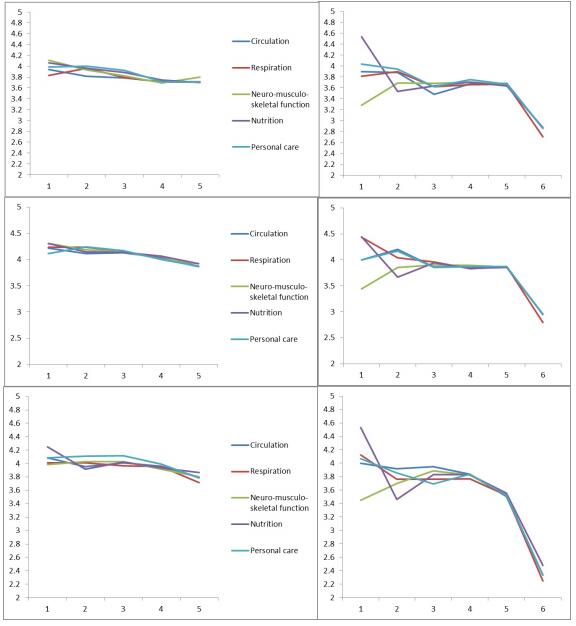
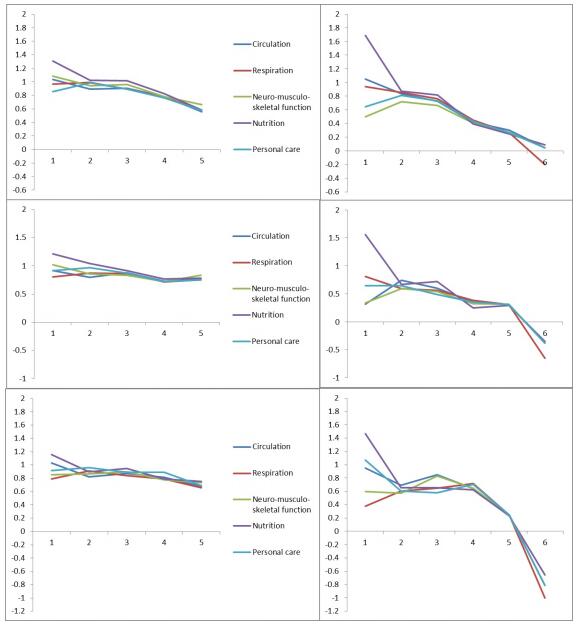
Methods: This exploratory data analysis study reused an existing Omaha System dataset to reveal hidden patterns in health outcomes of frail vs. non-frail older adults relative to SBDH. Two separate metrics were used to classify SBDH and frailty. An existing summative SBDH index was derived from measures recommended by the Institute of Medicine (IOM). A new frailty index was created based on Omaha System terms mapped to frailty criteria established by Fried and colleagues. Heat maps and line graphs were developed using Microsoft Excel and R. Patterns were discovered and related hypotheses were evaluated using paired samples t-tests and two-way ANOVA tests in R.
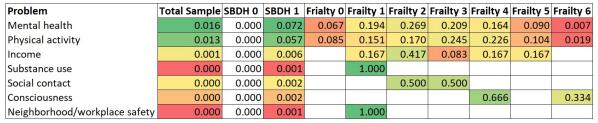
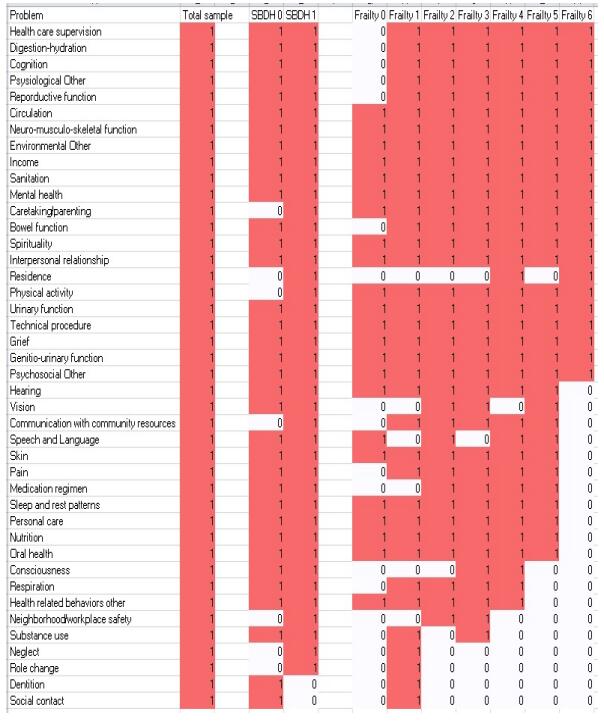
Results: Records (n = 1,618) were divided into SBDH Group 0 with no SBDH Problems (n = 1,397) and SBDH Group 1 with one or more SBDH Problems (n = 221). Overall, there was significant improvement in KBS after home care interventions. SBDH, Frailty, and interactions between SBDH and Frailty were significantly associated with differences in KBS outcomes. Visualizations showed numerous potential patterns for further research.
Discussion: SBDH Group 1 was largely defined by having the Mental health problem. Being in SBDH Group 1 was negatively associated with KBS outcomes. This aligns with the literature on the impact of mental health on overall health and wellbeing. As frailty scores increased, KBS outcomes decreased, demonstrating a possible continuum of increasing frailty as related co-morbidities accrued. This is a new perspective on frailty that should be further investigated. SBDH group, Frailty, and SBDH-Frailty interaction were all important for understanding outcomes for final K, final S, and difference in K, B, and S. For final B, SBDH group and Frailty were important. Because interaction between SBDH and Frailty was observed for most problems and outcomes, researchers who study Frailty should account for SBDH, especially mental health. SBDH problems were infrequent in the data. This has implications for our ability to understand SBDH in home care. Future research should incorporate data that include SBDH problem assessments.
Conclusion: This exploratory data analysis study identified relationships between SBDH and frailty for older adults along a continuum of frailty using the Omaha System. Further research is needed to validate the findings and to evaluate the metrics with other datasets and populations.
Citation: Grace Gao, Sasank Maganti, Karen A. Monsen. Older Adults, Frailty, and the Social and Behavioral Determinants of Health[J]. Big Data and Information Analytics, 2017, 2(3): 191-202. doi: 10.3934/bdia.2017012
Objective: To examine the associations between social and behavioral determinants of health (SBDH) and frailty among older adults using an existing Omaha System dataset collected in the community.
Design: Secondary exploratory data analysis.
Setting: An existing dataset of home health records from a Midwestern region, including Omaha System problems, interventions, and Knowledge (K), Behavior (B), and Status (S) outcomes.
Participants: Older adults (n = 1,618) that were 63.7% female with an average age of 80.1 years (SD = 7.6).
Methods: This exploratory data analysis study reused an existing Omaha System dataset to reveal hidden patterns in health outcomes of frail vs. non-frail older adults relative to SBDH. Two separate metrics were used to classify SBDH and frailty. An existing summative SBDH index was derived from measures recommended by the Institute of Medicine (IOM). A new frailty index was created based on Omaha System terms mapped to frailty criteria established by Fried and colleagues. Heat maps and line graphs were developed using Microsoft Excel and R. Patterns were discovered and related hypotheses were evaluated using paired samples t-tests and two-way ANOVA tests in R.
Results: Records (n = 1,618) were divided into SBDH Group 0 with no SBDH Problems (n = 1,397) and SBDH Group 1 with one or more SBDH Problems (n = 221). Overall, there was significant improvement in KBS after home care interventions. SBDH, Frailty, and interactions between SBDH and Frailty were significantly associated with differences in KBS outcomes. Visualizations showed numerous potential patterns for further research.
Discussion: SBDH Group 1 was largely defined by having the Mental health problem. Being in SBDH Group 1 was negatively associated with KBS outcomes. This aligns with the literature on the impact of mental health on overall health and wellbeing. As frailty scores increased, KBS outcomes decreased, demonstrating a possible continuum of increasing frailty as related co-morbidities accrued. This is a new perspective on frailty that should be further investigated. SBDH group, Frailty, and SBDH-Frailty interaction were all important for understanding outcomes for final K, final S, and difference in K, B, and S. For final B, SBDH group and Frailty were important. Because interaction between SBDH and Frailty was observed for most problems and outcomes, researchers who study Frailty should account for SBDH, especially mental health. SBDH problems were infrequent in the data. This has implications for our ability to understand SBDH in home care. Future research should incorporate data that include SBDH problem assessments.
Conclusion: This exploratory data analysis study identified relationships between SBDH and frailty for older adults along a continuum of frailty using the Omaha System. Further research is needed to validate the findings and to evaluate the metrics with other datasets and populations.

| [1] |
B. E. Alvarado, M.-V. Zunzunegui, F. Béland and J.-M. Bamvita, Life course social and health conditions linked to frailty in latin american older men and women, The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 63 (2008), 1399-1406. doi: 10.1093/gerona/63.12.1399

|
| [2] | J. A. Ávila-Funes, C. Helmer, H. Amieva, P. Barberger-Gateau, M. L. Goff, K. Ritchie, F. Portet, I. Carrière, B. Tavernier and L. M. Gutiérrez-Robledo et al., Frailty among community-dwelling elderly people in france: The three-city study, The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 63 (2008), 1089-1096. |
| [3] |
J. E. Carlson, K. A. Zocchi, D. M. Bettencourt, M. L. Gambrel, J. L. Freeman, D. Zhang and J. S. Goodwin, Measuring frailty in the hospitalized elderly: concept of functional homeostasis1, American Journal of Physical Medicine & Rehabilitation, 77 (1998), 252-257. doi: 10.1097/00002060-199805000-00012
|
| [4] |
A. M. Chamberlain, J. L. S. Sauver, D. J. Jacobson, S. M. Manemann, C. Fan, V. L. Roger, B. P. Yawn and L. J. F. Rutten, Social and behavioural factors associated with frailty trajectories in a population-based cohort of older adults, BMJ open, 6 (2016), e011410. doi: 10.1136/bmjopen-2016-011410
|
| [5] | S. L. Colby and J. M. Ortman et al., Projections of the Size and Composition of the US Population: 2014 to 2060, US Census Bureau, 9. |
| [6] |
L. P. Fried, C. M. Tangen, J. Walston, A. B. Newman, C. Hirsch, J. Gottdiener, T. Seeman, R. Tracy, W. J. Kop and G. Burke et al., Frailty in older adults: Evidence for a phenotype, The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 56 (2001), M146-M157. doi: 10.1093/gerona/56.3.M146
|
| [7] | C. T. M. R. T. S. M. R. Gruszin S Jorm L, Public Health Classifications Project - Determinants of Health Phase Two: Final Report, http://www.health.nsw.gov.au/hsnsw/Publications/classifications-project.pdf, 2010. |
| [8] |
I. A. Lang, R. E. Hubbard, M. K. Andrew, D. J. Llewellyn, D. Melzer and K. Rockwood, Neighborhood deprivation, individual socioeconomic status, and frailty in older adults, Journal of the American Geriatrics Society, 57 (2009), 1776-1780. doi: 10.1111/j.1532-5415.2009.02480.x
|
| [9] | K. S. Martin, The Omaha System: A Key to Practice, Documentation, and Information Management. (reprinted 2nd ed. ), Omaha, NE: Health Connections Press, 2005. |
| [10] |
A. d. C. Mello, E. M. Engstrom and L. C. Alves, Health-related and socio-demographic factors associated with frailty in the elderly: A systematic literature review, Cadernos de Saúde Pública, 30 (2014), 1143-1168. doi: 10.1590/0102-311X00148213
|
| [11] |
K. A. Monsen, J. K. Brandt, B. L. Brueshoff, C.-L. Chi, M. A. Mathiason, S. M. Swenson and D. R. Thorson, Social determinants and health disparities associated with outcomes of women of childbearing age who receive public health nurse home visiting services, Journal of Obstetric, Gynecologic & Neonatal Nursing, 46 (2017), 292-303. doi: 10.1016/j.jogn.2016.10.004
|
| [12] |
J. E. Morley, B. Vellas, G. A. Van Kan, S. D. Anker, J. M. Bauer, R. Bernabei, M. Cesari, W. Chumlea, W. Doehner and J. Evans et al., Frailty consensus: A call to action, Journal of the American Medical Directors Association, 14 (2013), 392-397. doi: 10.1016/j.jamda.2013.03.022
|
| [13] |
S. Moussavi, S. Chatterji, E. Verdes, A. Tandon, V. Patel and B. Ustun, Depression, Chronic diseases, and decrements in health: Results from the world health surveys, The Lancet, 370 (2007), 851-858. doi: 10.1016/S0140-6736(07)61415-9
|
| [14] | T. U. D. of Health and H. S. (HHS), Healtypeople2020, https://www.healthypeople.gov/2020/topics-objectives/topic/older-adults#1, 2016. |
| [15] | I. of Medicine (IOM), Living Well with Chronic Illness: A Call for Public Health Action, 2012. |
| [16] | I. of Medicine (US), Capturing Social and Behavioral Domains and Measures in Electronic Health Records: Phase 1, Washington, DC: National Academies Press, 2014. |
| [17] | I. of Medicine (US), Capturing Social and Behavioral Domains and Measures in Electronic Health Records: Phase 2, Washington, DC: National Academies Press, 2014. |
| [18] | N. I. of Nursing Research (NINR), The NINR Strategic Plan: Advancing Science, Improving Lives, https://www.ninr.nih.gov/sites/www.ninr.nih.gov/files/NINR_StratPlan2016_reduced.pdf, 2016. |
| [19] | W. H. Organization, What Are Social Determinants of Health?, http://www.who.int/social_determinants/sdh_definition/en/, 2012. |
| [20] | W. H. Organization, Health Impact Assessment (HIA), http://www.who.int/hia/evidence/doh/en/, 2017. |
| [21] |
M. J. C. A. Paw, J. M. Dekker, E. J. Feskens, E. G. Schouten and D. Kromhout, How to select a frail elderly population? A comparison of three working definitions, Journal of Clinical Epidemiology, 52 (1999), 1015-1021. doi: 10.1016/S0895-4356(99)00077-3
|
| [22] |
K. Rockwood, X. Song, C. MacKnight, H. Bergman, D. B. Hogan, I. McDowell and A. Mitnitski, A global clinical measure of fitness and frailty in elderly people, Canadian Medical Association Journal, 173 (2005), 489-495. doi: 10.1503/cmaj.050051
|
| [23] |
H. Syddall, C. Cooper, F. Martin, R. Briggs and A. Aihie Sayer, Is grip strength a useful single marker of frailty?, Age and Ageing, 32 (2003), 650-656. doi: 10.1093/ageing/afg111
|
| [24] | K. Van der Kooy, H. van Hout, H. Marwijk, H. Marten, C. Stehouwer and A. Beekman, Depression and the risk for cardiovascular diseases: systematic review and meta analysis, International Journal of Geriatric Psychiatry, 22 (2007), 613-626. |
| [25] | R. G. Wilkinson and M. Marmot, The Social Determinants of Health: The Solid Facts (2nd ed. ), World Health Organization, 2003. |
| [26] |
J. Woo, W. Goggins, A. Sham and S. Ho, Social determinants of frailty, Gerontology, 51 (2005), 402-408. doi: 10.1159/000088705
|
Figures(4) / Tables(4)

Grace Gao, Sasank Maganti, Karen A. Monsen. Older Adults, Frailty, and the Social and Behavioral Determinants of Health[J]. Big Data and Information Analytics, 2017, 2(3): 191-202. doi: 10.3934/bdia.2017012









 DownLoad:
DownLoad: