Figure 1.
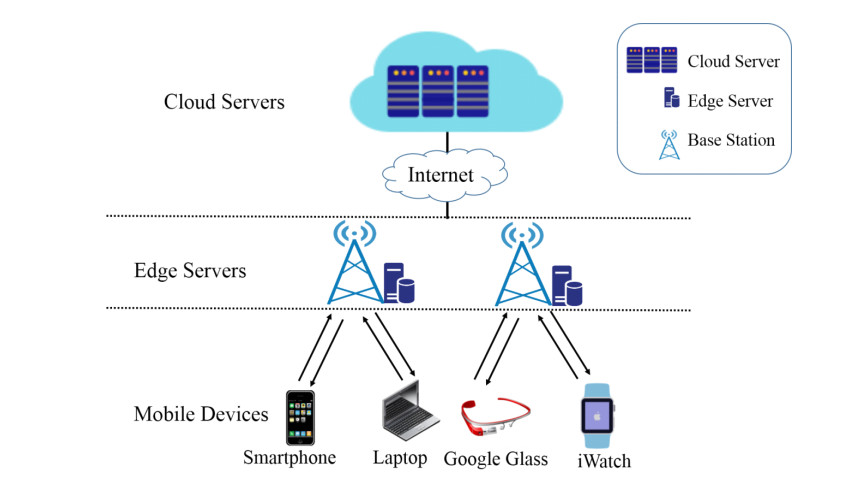
The architecture of MEC.





Citation: Saba Loloei, Hamed Pouraram, Reza Majdzadeh, Amirhossein Takian, Massomeh Goshtaei, Abolghasem Djazayery. Policy analysis of salt reduction in bread in Iran[J]. AIMS Public Health, 2019, 6(4): 534-545. doi: 10.3934/publichealth.2019.4.534
| [1] | Hongmei Jin, Ning He, Boyu Liu, Zhanli Li . Research on gesture recognition algorithm based on MME-P3D. Mathematical Biosciences and Engineering, 2024, 21(3): 3594-3617. doi: 10.3934/mbe.2024158 |
| [2] | Yong Tian, Tian Zhang, Qingchao Zhang, Yong Li, Zhaodong Wang . Feature fusion–based preprocessing for steel plate surface defect recognition. Mathematical Biosciences and Engineering, 2020, 17(5): 5672-5685. doi: 10.3934/mbe.2020305 |
| [3] | Yanpei Liu, Wei Huang, Liping Wang, Yunjing Zhu, Ningning Chen . Dynamic computation offloading algorithm based on particle swarm optimization with a mutation operator in multi-access edge computing. Mathematical Biosciences and Engineering, 2021, 18(6): 9163-9189. doi: 10.3934/mbe.2021452 |
| [4] | Mingchang Ni, Guo Zhang, Qi Yang, Liqiong Yin . Research on MEC computing offload strategy for joint optimization of delay and energy consumption. Mathematical Biosciences and Engineering, 2024, 21(6): 6336-6358. doi: 10.3934/mbe.2024276 |
| [5] | Xiangshuai Duan, Naiping Song, Fu Mo . An edge intelligence-enhanced quantitative assessment model for implicit working gain under mobile internet of things. Mathematical Biosciences and Engineering, 2023, 20(4): 7548-7564. doi: 10.3934/mbe.2023326 |
| [6] | Weibin Jiang, Xuelin Ye, Ruiqi Chen, Feng Su, Mengru Lin, Yuhanxiao Ma, Yanxiang Zhu, Shizhen Huang . Wearable on-device deep learning system for hand gesture recognition based on FPGA accelerator. Mathematical Biosciences and Engineering, 2021, 18(1): 132-153. doi: 10.3934/mbe.2021007 |
| [7] | Zhigao Zeng, Cheng Huang, Wenqiu Zhu, Zhiqiang Wen, Xinpan Yuan . Flower image classification based on an improved lightweight neural network with multi-scale feature fusion and attention mechanism. Mathematical Biosciences and Engineering, 2023, 20(8): 13900-13920. doi: 10.3934/mbe.2023619 |
| [8] | Shangbin Li, Yu Liu . Human motion recognition based on Nano-CMOS Image sensor. Mathematical Biosciences and Engineering, 2023, 20(6): 10135-10152. doi: 10.3934/mbe.2023444 |
| [9] | Yuan Tian, Biao Song, Mznah Al Rodhaan, Chen Rong Huang, Mohammed A. Al-Dhelaan, Abdullah Al-Dhelaan, Najla Al-Nabhan . A stochastic location privacy protection scheme for edge computing. Mathematical Biosciences and Engineering, 2020, 17(3): 2636-2649. doi: 10.3934/mbe.2020144 |
| [10] | Yuanyao Lu, Kexin Li . Research on lip recognition algorithm based on MobileNet + attention-GRU. Mathematical Biosciences and Engineering, 2022, 19(12): 13526-13540. doi: 10.3934/mbe.2022631 |
With the rapid growth of mobile devices, it is feasible and urgent-demand to deploy image recognition applications on mobile devices to provide image recognition services. However, since the constraint computing and storage resource, as well as energy resources, it is difficult to perform all image recognition applications on mobile devices. In recent years, a popular solution is to offload the image recognition tasks to the remote cloud servers [1,2]. That is, the image recognition applications deployed on mobile devices, they only responsible for collecting images. Then, the mobile devices upload the images to the cloud servers to perform recognition tasks. Although this solution can save the computing and storage resources, as well as the energy resources of mobile devices. In doing so, mobile devices can provide long-lasting image recognition services for mobile users. However, in 5G networks, if hundreds of thousands of mobile users upload images to the cloud servers at the same time, the core network can be overload and even incurs network congestion, it is very likely resulting in long transmission delays. Therefore, traditional cloud computing solution cannot meet the requirements of real time response.
Mobile Edge Computing (MEC), as an emerging architecture, it is possible to solve the traditional computing solution problems that cannot meet the users real time demands [3,4,5,6]. In MEC architecture, many small-scale edge servers are deploying at the edge of the network. These edge servers can provide computing and storage resources for image recognition applications. Thus, mobile users can offload the image recognition tasks to the edge servers rather than the cloud servers. Since users close to the edge servers, generally, one hope. Therefore, the transmission delays can be reduced. In traditional cloud computing scheme, running deep neural network models on the cloud servers can achieve good performance. The reason is that cloud servers are regarded as rich computing and storage resources, as well as stored a large number of trainable images. It is well known that using a large number of trainable images to train a very deep neural networks can achieve good performance. However, in MEC architecture, a single edge server has a small range so that it only can collect a small number of images. Therefore, it is inappropriate to use deep neural network models to run the image recognition tasks.
To address this problem, in this paper, we propose a location-ware feature extraction algorithm for image recognition, called DAGDNEP. In DAGDNEP, we employ DAGDNEP to construct two adjacency graphs to preserve the intra-class information and the inter-class information that make every samples linked to its homogeneous and heterogeneous neighbors respectively and also, we introduce a heat kernel function as weight when construct matrix of the intra-class and inter-class. Thus, DAGDNEP could keep the geometric structure of the given data that find an optimal projection matrix. Experimental results validate the effectiveness of our DAGDNEP in comparison with DAGDNE algorithm.
The reminder of this paper is organized as follows. Section 2 introduces the related work, which includes mobile edge computing and feature extraction algorithm. In Section 3, we introduce the proposed feature extraction algorithm. In section, we discuss the combination between MEC architecture and the proposed algorithms. The experimental results are presented in Section 4. Finally, we provide the concluding remarks in Section 5.
Mobile Edge Computing (MEC), which can provide computing and storage resources for image recognition applications by deploying some small-scale servers at the edge of the network [3,4,5,6]. MEC mainly solves the problems of traditional mobile cloud computing that directly upload the raw images to the cloud servers that incurs long response time [7]. With the explosive growth of mobile traffic, if hundreds of thousands of mobile users upload the image data to cloud servers at the same time, it may incur the core network congestion, resulting longer transmission delays and longer response time. The architecture of MEC is as shown in Figure 1, which consists of three layers of components, mobile devices, edge servers and cloud servers.
Mobile Devices: Mobile devices are the front-end devices, such as smartphone, laptop, iWatch, etc. Mobile devices are utilized to install image recognition applications. Since the constraint computing and storage resources of mobile devices, we only use them to capture images and receive results, as well as show results. Edge Servers: Edge servers are small scale servers deploying at the edge of the network. Edge servers are typically performing single function with limited resources, such as cache servers and specialized servers. Since edge servers close to users, using edge servers to provide computing and storage resources for image recognition applications can reduce the transmission delay. This is because mobile users only require upload the captured image to the edge servers instead of cloud servers. Cloud Servers: Cloud servers are regarded as having rich computing and storage resources. In general, the cloud servers are very far away from users.
Many feature extraction algorithms are proposed in recent years, such as discriminant neighborhood embedding [8], marginal Fisher analysis [9,10], local features discriminant projection [7], Appropriate points choosing based DAGDNE [11], double adjacency graphs-based discriminant neighborhood embedding [12].
For example, Zhang et al. [8] proposed discriminant neighborhood embedding, which supposes that multi-class data points in high-dimensional space tend to move due to local intra-class attraction or inter-class repulsion, and the optimal embedding from the point of view of classification is discovered consequently. Yan et al. [9,10] proposed marginal fisher analysis, which adopts two adjacency graphs to preserving the geometric structure. This approach first constructs two adjacency graphs, the intrinsic graph and the penalty graph, of which the intrinsic graph characterizes the intra-class compactness and connects each data point with its neighboring points of the same class, while the penalty graph connects the marginal points and characterizes the inter-class separability. Ding and Zhang [12] proposed double adjacency graphs-based discriminant neighborhood embedding, which let each sample be respectively linked to its homogeneous and heterogeneous neighbors by constructing two adjacency graphs. As a consequence, balance links are produced, neighbors belonging to the same class are compact while neighbors belonging to different classes become separable in the subspace. Thus, DAGDNE could keep the local structure of a given data and find a good projection matrix.
However, these algorithms ignore the location information. Thus, these algorithms just preserve the local structure but ignore the location information. Nevertheless, in the task of clustering or classification, the location information is very important.
In this section, we will introduce the location-aware feature extraction algorithm, called DAGDNEP. Let
Similar to DAGDNE algorithm, DAGDNEP requires to construct two adjacency graphs. Let
The intra-class adjacency matrix
|
$
F_{ij}^w = \left\{ {exp(−||xi−xj||2β), xi∈NHwk(xj) or xj∈NHwk(xi)0 , otherwise } \right.$
|
(1) |
|
$F_{ij}^b = \left\{ {exp(−||xi−xj||2β),, xi∈NHbk(xj) or xj∈NHbk(xi)0 , otherwise } \right.$
|
(2) |
where
The intra-class scatter
| $\Phi ({\bf{P}}) = {\rm{ }}\sum\limits_{i, j} {||{{\bf{P}}^T}{{\bf{x}}_i} - {{\bf{P}}^T}{{\bf{x}}_j}|{|^2}} F_{ij}^w = {\rm{ }}2tr\{ {{\bf{P}}^T}{\bf{X}}({{\bf{D}}^w} - {{\bf{F}}^w}){{\bf{X}}^T}{\bf{P}}\} $ | (3) |
| $\Psi ({\bf{P}}) = {\rm{ }}\sum\limits_{i, j} {||{{\bf{P}}^T}{{\bf{x}}_i} - {{\bf{P}}^T}{{\bf{x}}_j}|{|^2}} F_{ij}^b = {\rm{ }}2tr\{ {{\bf{P}}^T}{\bf{X}}({{\bf{D}}^b} - {{\bf{F}}^b}){{\bf{X}}^T}{\bf{P}}\} $ | (4) |
where
In order to achieve impressive accuracy, the extracted features need to satisfy that features from the same class labels are compact while features from different class labels become separable. To this end, we need to maximize the margin of total inter-class scatter and total intra-class scatter, i.e.,
| $\Theta ({\bf{P}}) = \Psi ({\bf{P}}) - \Phi ({\bf{P}})$ | (5) |
DAGDNEP aims to find a feature extractor
|
$\left\{ {maxP tr{PTXSXTP}s.t. PTP=I } \right.$
|
(6) |
Where
| ${\bf{XS}}{{\bf{X}}^T}{\bf{P}} = \lambda {\bf{P}}$ | (7) |
Thus,
The details of DAGDNEP is given in Algorithm 1.
| Algorithm 1. Location-aware Feature Extraction (DAGDNEP) |
| Input: A training image set Output: Feature Extractor: Step 1. Compute the intra-class scatter matrix Step 2. Eigenvalue decomposition of Step 3. Choose the first |
The DAGDNEP algorithm is an improved version of the DAGDNE algorithm. DAGDNE could keep the local intrinsic structure for the raw image data through the extracted features by constructing two adjacency graphs. However, DAGDNE just gives the weight value +1 when construct intra-class adjacency graph and inter-class adjacency graph. That just give +1 cannot preserve the geometric structure of the given data and the geometric structure plays a different role in the classification task. Therefore, when extracting the discriminative features from the raw image data, some more important discriminative features may miss. DAGDNEP regulates heat kernel function as the weight that can preserve the geometric structure among data. As a result, DAGDNEP can achieve a good performance.
Since a single edge server only collects a small amount of images, it is inappropriate to use deep neural network models to perform image recognition tasks. The reason is that using deep neural network models cannot achieve good performance due to the small number of images stored on a single edge server. In the contrast, the proposed feature extraction algorithm can well fit the small number of images and achieve good performance. In this sense, Combining the MEC architecture [13,14,15,16,17] and the proposed feature extraction algorithm to provide image recognition services is advisable.
We have conducted experiments on two datasets, which are publicly available, UMIST and ORL datasets. Wherein the UMIST dataset contains 564 face images of 20 individuals and the ORL dataset contains 400 face images of 40 individuals, with 10 images for each individual.
DAGDNE and the proposed algorithm are implemented in MATLAB 2015b, and are conducted on an i5 Intel ® Core CPU 2.50 GHz machine with 4G bytes of memory. In our experiment, which requires the nearest neighbor parameter
To evaluate the effectiveness and the correctness of DAGDNEP, experiments are carried out on UMIST and ORL databases, and the results are compared with DAGDNE.
In the experiment, the parameter
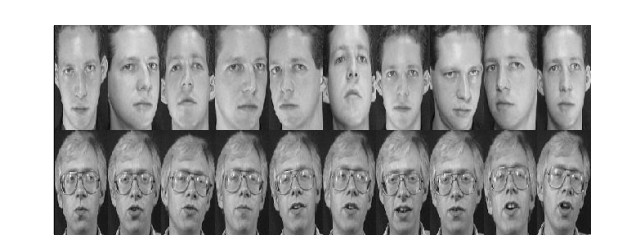
The UMIST dataset consists of 564 images of 20 individuals, taking into account race, sex and appearance. Each subject is taken in a range of poses from profile to frontal views. The pre-cropped dataset is used and the size of each image is

First, we consider parameter choose, the nearest neighbor parameter
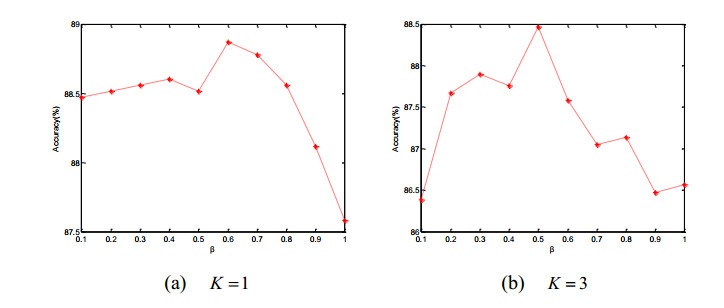
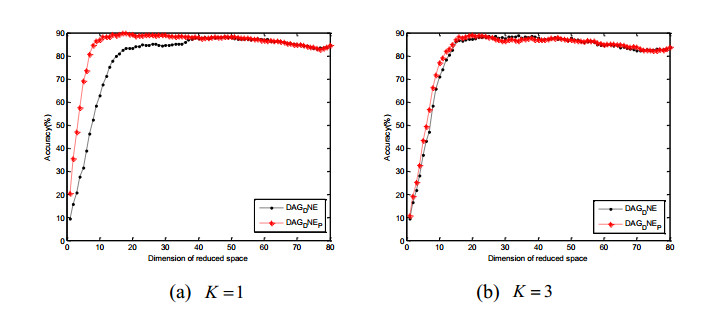
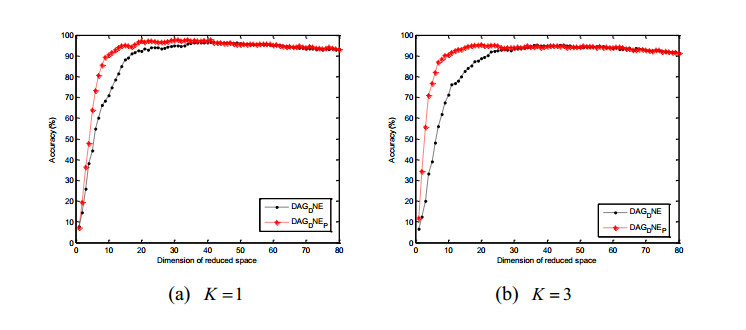
Figure 4 (a) and (b) show the accuracy of two algorithms vs. dimensionality of subspace with different
The ORL dataset is composed of 40 distinct subjects, each of which contains 10 different gray-scale images. In ORL dataset, images for each subject were taken by varying the lighting, facial expressions or facial details at different times, and all were taken against a dark homogenous background in an upright and frontal position. The size of each image is
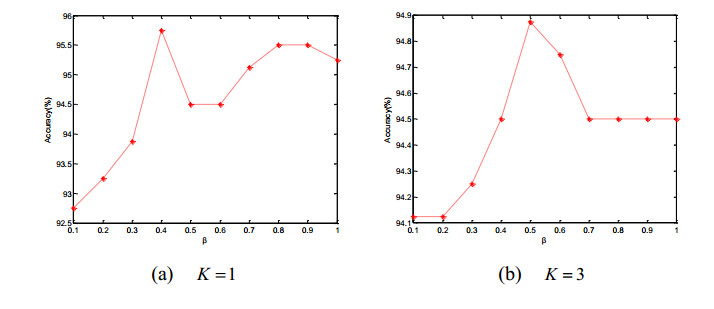
In this experiment, we reduce dimensionality with two times so as to get a high running speed. When choose parameter, similar to UMIST dataset, the neighborhood parameter
Figure 7 shows the accuracy of DAGDNE and DAGDNEP algorithms vs. dimensionality of subspace with different
In this paper, we proposed a location-aware feature extraction algorithm to fit the image recognition in the MEC environment. By considering that in MEC architecture, a single edge server only collects a small number of images, we propose a location-aware feature extraction algorithm, which can achieve good performance when the trainable images are very few. Moreover, the proposed feature extraction algorithm considers the location information of the images, compared with traditional feature extraction algorithms, it achieves higher accuracy. Thus, by combining the MEC architecture and the proposed feature extraction algorithm, it is possible to support the mobile devices to provide long-lasting real time response and high accuracy image recognition services. Finally, on two publicly datasets, we demonstrate the effectiveness of our proposed feature extraction algorithm.
The work is supported by National Natural Science Foundation of China (No.61003100), Hubei Provincial Natural Science Foundation of China (No. 2017CFA012), National Natural Science Foundation of China (No. 61572012), National Natural Science Foundation of Hubei Province (No.2015CFB525) and Wuhan science and technology plan innovation team project (No.201307020402005).
All authors declare no conflicts of interest in this paper.
| [1] |
Jafari M, Mohammadi M, Ghazizadeh H, et al. (2016) Feasibility and outcome of reducing salt in bread: a community trial in Southern Iran. Glob J Health Sci 8: 163. doi: 10.5539/gjhs.v8n12p163

|
| [2] |
Silow C, Axel C, Zannini E, et al. (2016) Current status of salt reduction in bread and bakery products-a review. J Cereal Sci 72: 135–145. doi: 10.1016/j.jcs.2016.10.010
|
| [3] |
Israr T, Rakha A, Sohail M, et al. (2016) Salt reduction in baked products: Strategies and constraints. Trends Food Sci Tech 51: 98–105. doi: 10.1016/j.tifs.2016.03.002
|
| [4] |
Lynch EJ, Dal Bello F, Sheehan EM, et al. (2009) Fundamental studies on the reduction of salt on dough and bread characteristics. Food Res Intl 42: 885–891. doi: 10.1016/j.foodres.2009.03.014
|
| [5] |
Antúnez L, Giménez A, Ares G (2016) A consumer-based approach to salt reduction: Case study with bread. Food Res Intl 90: 66–72. doi: 10.1016/j.foodres.2016.10.015
|
| [6] |
Karizaki VM (2017) Ethnic and traditional Iranian breads: different types, and historical and cultural aspects. J Ethn Food 4: 8–14. doi: 10.1016/j.jef.2017.01.002
|
| [7] | Belz MC, Ryan LA, Arendt EK (2012) The impact of salt reduction in bread: a review. Crit Rev Food Sci Nutr 5: 514–524. |
| [8] | Tomonari T, Fukuda M, Miura T, et al. (2011) Is salt intake an independent risk factor of stroke mortality? Demographic analysis by regions in Japan. J Am Soc Hypertens 25: 456–462. |
| [9] |
Pasqualone A, Caponio F, Pagani MA, et al. (2019) Effect of salt reduction on quality and acceptability of durum wheat bread. Food Chem 289: 575–581. doi: 10.1016/j.foodchem.2019.03.098
|
| [10] |
Avolio AP, Clyde KM, Beard TC, et al. (1986) Improved arterial distensibility in normotensive subjects on a low salt diet. Arteriosclerosis 6: 166–169. doi: 10.1161/01.ATV.6.2.166
|
| [11] |
D'Elia L, Rossi G, Ippolito R, et al. (2012) Habitual salt intake and risk of gastric cancer: a meta-analysis of prospective studies. Clin Nutr 31: 489–498. doi: 10.1016/j.clnu.2012.01.003
|
| [12] |
Quilez J, Salas-Salvado J (2012) Salt in bread in Europe: potential benefits of reduction. Nutr Rev 70: 666–678. doi: 10.1111/j.1753-4887.2012.00540.x
|
| [13] | Ghazizadeh-Hashemi SH, Larijani B (2015) National action plan for prevention and control of non communicable diseases and the related risk factors in the Islamic Republic of Iran, 2015–2025. Tehran, Iran: Aftab e Andisheh Publ, 47–65. |
| [14] | World Health Organization (2011) Global status report on noncommunicable diseases 2010: Geneva. Available from: https://www.who.int/nmh/publications/ncd_report2010/en/. |
| [15] | World Health Organization (2010) Creating an enabling environment for population-based salt reduction strategies: report of a joint technical meeting held by WHO and the Food Standards Agency, United Kingdom, July 2010. Available from: https://apps.who.int/iris/handle/10665/44474. |
| [16] | Shahram Rafieifar M, Hossein Kazemeini M (2016) Strategies and opportunities ahead to reduce salt intake. Arc Iran Med 19: 729–734. |
| [17] | Alireza Khosravi M, Reza Malekzadeh M, Sarrafzadegan N (2012) Advocacy strategies and action plans for reducing salt intake in Iran. Arc Iran Med 15: 320–324. |
| [18] |
Avramenko N, Tyler R, Scanlon M, et al. (2018) The chemistry of bread making: The role of salt to ensure optimal functionality of its constituents. Food Rev Intl 34: 204–225. doi: 10.1080/87559129.2016.1261296
|
| [19] | Buse K, Dickinson C, Gilson L, et al. (2009) How can the analysis of power and process in policy-making improve health outcomes? Off J Int Hosp Fed 45: 14. |
| [20] | Miles MB, Huberman AM, Huberman MA, et al. (1994) Qualitative data analysis: An expanded sourcebook. Sage. |
| [21] |
Walt G, Shiffman J, Schneider H, et al. (2008) 'Doing'health policy analysis: methodological and conceptual reflections and challenges. Health Policy Plan 23: 308–317. doi: 10.1093/heapol/czn024
|
| [22] | Walt G (1994) Health policy: an introduction to process and power. Available from: https://repository.library.georgetown.edu/handle/10822/870131. |
| [23] |
Fontanet I, Davidou S, Dacremont C, et al. (1997) Effect of water on the mechanical behaviour of extruded flat bread. J Cereal Sci 25: 303–311. doi: 10.1006/jcrs.1996.0087
|
| [24] |
Brinsden HC, He FJ, Jenner KH, et al. (2013) Surveys of the salt content in UK bread: progress made and further reductions possible. BMJ open 3: e002936. doi: 10.1136/bmjopen-2013-002936
|
| [25] |
Amid J (2007) The dilemma of cheap food and self-sufficiency: The case of wheat in Iran. Food Policy 32: 537–552. doi: 10.1016/j.foodpol.2006.11.001
|
| [26] |
Moynihan DP (2006) Ambiguity in policy lessons: The agencification experience. Public Adm 84: 1029–1050. doi: 10.1111/j.1467-9299.2006.00625.x
|
| [27] |
Walker L, Gilson L (2004) 'We are bitter but we are satisfied': nurses as street-level bureaucrats in South Africa. Soc Sci Med 59: 1251–1261. doi: 10.1016/j.socscimed.2003.12.020
|
| [28] | Kilcast D, Angus F (2007) Reducing salt in foods: Practical strategies. Elsevier. |
| [29] | Salovaara H (2009) Technologies of salt reduction in bread: issues, problems and solutions. Salt in bread: technical, taste and other parameters for healthy eating: CCAB Seminar Brussels, |
| [30] | Belgium: Centre de Conferences Albert Borschette (CAAB). |
| [31] |
30. Dunford EK, Eyles H, Ni Mhurchu C, et al. (2011) Changes in the sodium content of bread in Australia and New Zealand between 2007 and 2010: implications for policy. Med J Aust 195: 346–349. doi: 10.5694/mja11.10673
|
| [32] | 31. World Health Organization (2016) The SHAKE technical package for salt reduction. Available from: https://apps.who.int/iris/handle/10665/250135. |
 publichealth-06-04-534-s001.pdf publichealth-06-04-534-s001.pdf |
 |
| 1. | Marwa Zamzam, Tallal El-Shabrawy, Mohamed Ashour, 2020, Energy-Efficient Computation Offloading for Indoor Localization Based on Game Theory, 978-1-7281-8226-1, 270, 10.1109/NILES50944.2020.9257948 | |
| 2. | Xiwen Yu, Kai Wang, Shaoxuan Wang, Miaochao Chen, Research on Image Recognition of Building Wall Design Defects Based on Partial Differential Equation, 2021, 2021, 1687-9139, 1, 10.1155/2021/1229660 | |
| 3. | Hongyan Sang, 2022, Chapter 82, 978-3-030-96907-3, 660, 10.1007/978-3-030-96908-0_82 |
Saba Loloei, Hamed Pouraram, Reza Majdzadeh, Amirhossein Takian, Massomeh Goshtaei, Abolghasem Djazayery. Policy analysis of salt reduction in bread in Iran[J]. AIMS Public Health, 2019, 6(4): 534-545. doi: 10.3934/publichealth.2019.4.534

 DownLoad:
DownLoad:

