Citation: Zijian Li, Aaron A. Jennings. Implied Maximum Dose Analysis of Standard Values of 25 Pesticides Based on Major Human Exposure Pathways[J]. AIMS Public Health, 2017, 4(4): 383-398. doi: 10.3934/publichealth.2017.4.383

| [1] | European Commission. Plants – Pesticide. 2016. Available from: http://ec.europa.eu/food/plant/pesticides/index_en.htm (Accessed on 07.30.2016). |
| [2] | U.S. Environmental Protection Agency. U.S. EPA about pesticide. 2014. Available from: http://www.epa.gov/pesticides/about/index.htm (accessed on 03.17.15). |
| [3] | University of Minnesota. Pesticides in the Environment-Pesticide Transport and Fate. 2003. Available from: http://enhs.umn.edu/current/5103/pesticide/fate.html (accessed on 01.13.16). |
| [4] | Farmworker J (2008) Reproductive Health Effects of Pesticide Exposure. Available from: https://www.farmworkerjustice.org/sites/default/files/documents/Reproductibe%20Health%20Effects%20of%20Pesticide%20Exposure%20-%20Paper.pdf (accessed on 03.25.15). |
| [5] | Alewu B, Nosiri C (2011) Pesticides and human health. In: Stoytcheva M, editor. , editor. Pesticides in the Modern World – Effects of Pesticides Exposure. InTech. 231-250. Available from: http://www.intechopen.com/books/pesticides-in-the-modern-world-effects-of-pesticides-exposure/pesticide-and-human-health. |
| [6] |
Proctor DM, Shay EC, Scott PK (1997) Health-based soil action levels for trivalent and hexavalent chromium: a comparison with state and federal standards. J Soil Contam 6: 595-648. doi: 10.1080/15320389709383592

|
| [7] |
Davis A, Sherwin D, Ditmars R, et al. (2001) An analysis of soil arsenic records of decision. Environ Sci Technol 35: 2401-2406. doi: 10.1021/es001411i
|
| [8] |
Jennings A, Li Z (2014) Scope of the worldwide effort to regulate pesticide contamination in surface soils. J Environ Manag 146: 420-443. doi: 10.1016/j.jenvman.2014.07.020
|
| [9] |
Li Z, Jennings A (2017) Ranking system for national regulatory jurisdictions based on pesticide standard values in major exposures. AIMS Environ Sci 4: 540-561. doi: 10.3934/environsci.2017.4.540
|
| [10] | Jennings A, Li Z (2017) Worldwide regulatory guidance values applied to direct contact surface soil pesticide contamination: Part II-Noncarcinogenic pesticides. Air Soil Water Res 10: 1-14. |
| [11] | Jennings A, Li Z (2017) Worldwide regulatory guidance values applied to direct contact surface soil pesticide contamination: Part I-Carcinogenic pesticides. Air Soil Water Res 10: 1-12. |
| [12] |
Joon CC, Han RL, Alan DZ, et al. (2016) Fluoride: A naturally-occurring health hazard in drinking-water resources of Northern Thailand. Sci Total Environ 545-546: 266-279. doi: 10.1016/j.scitotenv.2015.12.069
|
| [13] |
Rachel Baum, Urooj Amjad, Jeanne Luh, et al. (2015) An examination of the potential added value of water safety plans to the United States national drinking water legislation. Int J Hyg Environ Health 218: 677-685. doi: 10.1016/j.ijheh.2014.12.004
|
| [14] | Stockholm Convention. The 12 initial POPs under the Stockholm Convention. 2008. Available from: http://chm.pops.int/TheConvention/ThePOPs/The12InitialPOPs/tabid/296/Default.aspx (accessed on 7/30/2016). |
| [15] |
Jennings A, Li Z (2015) Residential surface soil guidance applied worldwide to the pesticides added to the Stockholm Convention in 2009 and 2011. J Environ Manage 160: 226-240. doi: 10.1016/j.jenvman.2015.06.020
|
| [16] |
Jennings A, Li Z (2015) Residential surface soil guidance values applied worldwide to the original 2001 Stockholm Convention POP pesticides. J Environ Manage 160: 16-29. doi: 10.1016/j.jenvman.2015.06.001
|
| [17] | Li Z, Jennings A (2017) Worldwide Regulations of Standard Values of Pesticides for Human Health Risk Control: A Review. Int J Environ Res Public Health 14: 826. |
| [18] | Agency for Toxic Substances and Disease Registry. Public Health Assessment Guidance Manual, 2005. Available from: http://www.atsdr.cdc.gov/hac/PHAManual/appg.html (accessed on 07.08.15). |
| [19] | U.S. Environmental Protection Agency. Regional Screening Levels (RSLs) – Generic Tables, May 2016. Available from: https://www.epa.gov/risk/regional-screening-levels-rsls-generic-tables-may-2016 (accessed on 7/30/2016). |
| [20] | Li Z (2016) Analysis of worldwide pesticide regulatory models and standards for controlling human health risk. Case Western Reserve University. Available from: https://etd.ohiolink.edu/. |
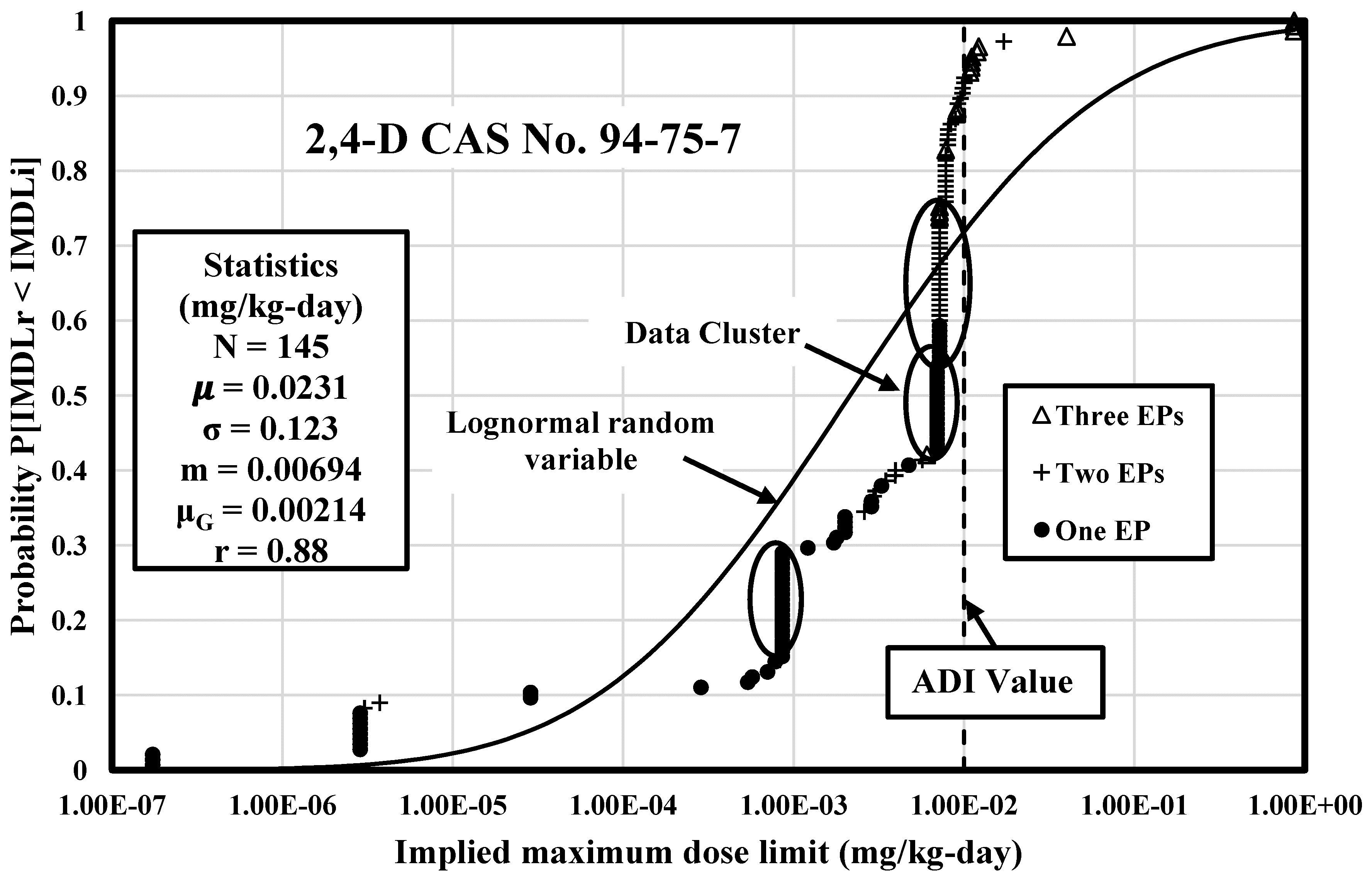
| [21] | World Health Organization (2003) 2,4-D in Drinking-water, background document for development of WHO Guidelines for Drinking-water Quality. Available from: http://www.who.int/water_sanitation_health/dwq/chemicals/24D.pdf (accessed on 07.30.16). |
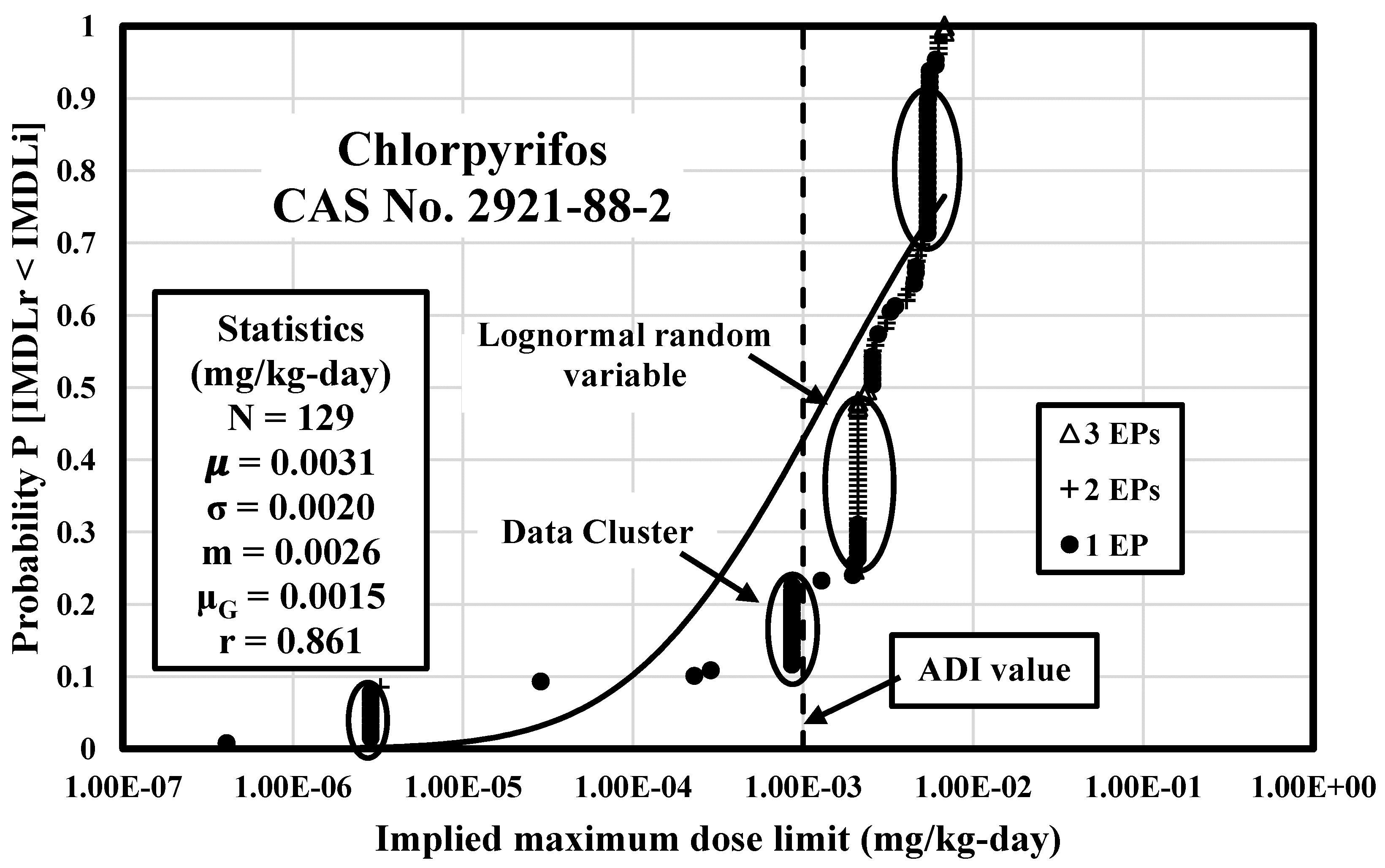
| [22] | Federal Institute for Risk Assessment (2012) Reconsideration of the human toxicological reference values (ARfD, ADI) for Chlorpyrifos. Available from: http://www.bfr.bund.de/cm/349/reconsideration-of-the-human-toxicological-reference-values-arfd-adi-for-chlorpyrifos.pdf (accessed on 07.30.16). |
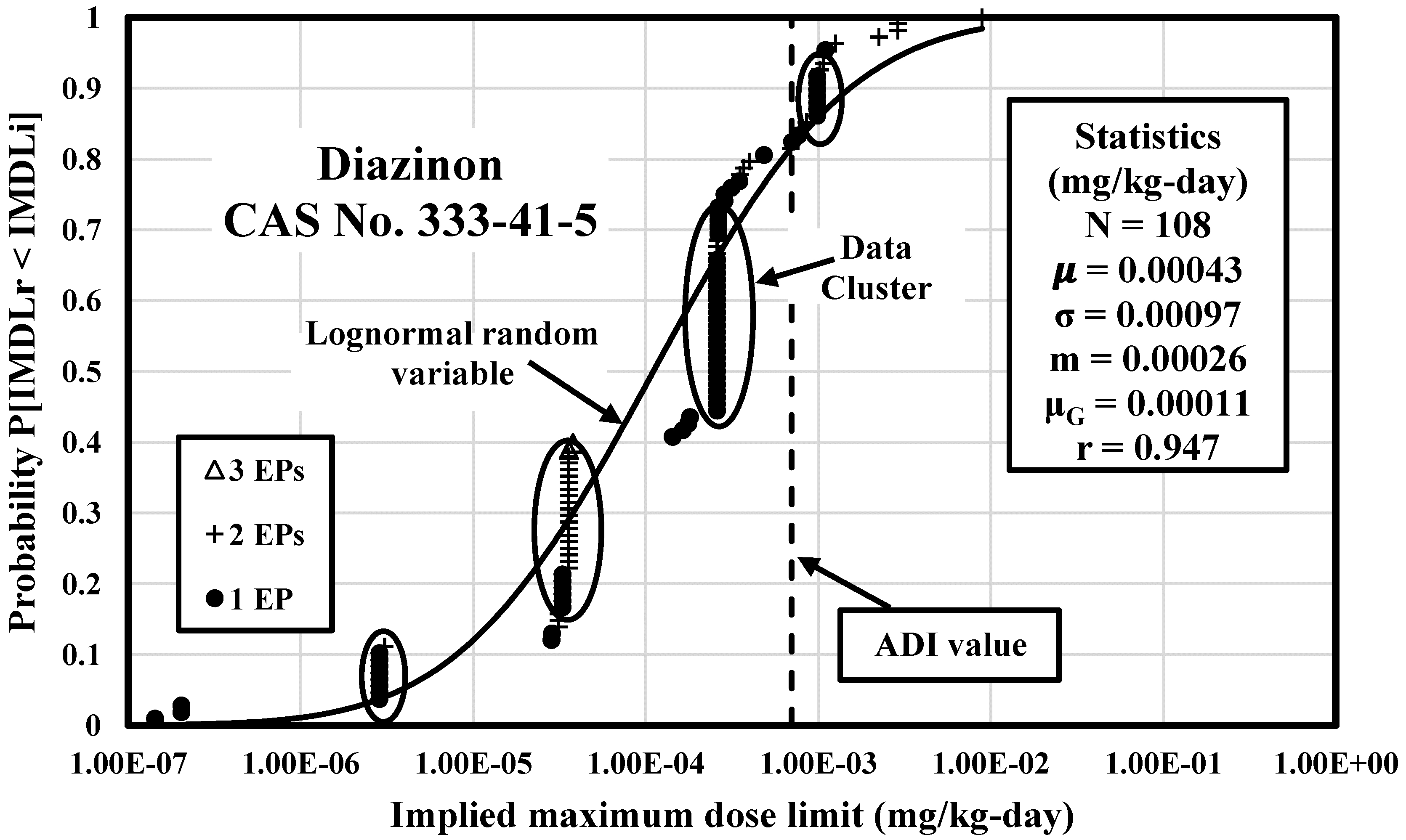
| [23] | Government of Canada (2009) Guidelines for Canadian Drinking Water Quality: Guideline Technical Document – Diazinon. Available from: http://healthycanadians.gc.ca/publications/healthy-living-vie-saine/water-diazinon-eau/index-eng.php (accessed on 07.30.16). |
Figures(3) / Tables(6)

Zijian Li, Aaron A. Jennings. Implied Maximum Dose Analysis of Standard Values of 25 Pesticides Based on Major Human Exposure Pathways[J]. AIMS Public Health, 2017, 4(4): 383-398. doi: 10.3934/publichealth.2017.4.383







 DownLoad:
DownLoad: