Citation: Shafiuzzaman Khan Khadem, Malabika Basu, Michael F. Conlon. Capacity enhancement and flexible operation of unified power quality conditioner in smart and microgrid network[J]. AIMS Energy, 2018, 6(1): 49-69. doi: 10.3934/energy.2018.1.49

| [1] |
Seme S, Lukač N, Štumberger B, et al. (2017) Power quality experimental analysis of grid-connected photovoltaic systems in urban distribution networks. Energy 139: 1261–1266. doi: 10.1016/j.energy.2017.05.088

|
| [2] |
Efkarpidis N, Rybel TD, Driesen J (2016) Technical assessment of centralized and localized voltage control strategies in low voltage networks. Sust Energ Grids Netw 8: 85–97. doi: 10.1016/j.segan.2016.09.003
|
| [3] | Khadem SK, Basu M, Conlon MF (2010) Power quality in grid connected renewable energy systems: Role of custom power devices. J Renew Energ Power Qual 8: 505. |
| [4] | Ghosh A, Ledwich G (2002) Power quality enhancement using custom power devices. AH Dordrecht: Kluwer Academic Publisher Group. |
| [5] |
Khadkikar V (2012) Enhancing electric power quality using UPQC: A comprehensive overview. IEEE T Power Electr 27: 2284–2297. doi: 10.1109/TPEL.2011.2172001
|
| [6] |
Han B, Bae B, Kim H, et al. (2006) Combined operation of unified power-quality conditioner with distributed generation. IEEE T Power Deliver 21: 330–338. doi: 10.1109/TPWRD.2005.852843
|
| [7] |
Khadem SK, Basu M, Conlon MF (2015) Intelligent islanding and seamless reconnection technique for microgrid with UPQC. IEEE J Em Sel Top P 3: 483–492. doi: 10.1109/JESTPE.2014.2326983
|
| [8] | Khadem SK, Basu M, Conlon MF (2013) A new placement and integration method of UPQC to improve the power quality in DG network. Power Engineering Conference. IEEE, 1–6. |
| [9] |
Khadem SK, Basu M, Conlon MF (2011) A review of parallel operation of active power filters in the distributed generation system. Renew Sust Energ Rev 15: 5155–5168. doi: 10.1016/j.rser.2011.06.011
|
| [10] |
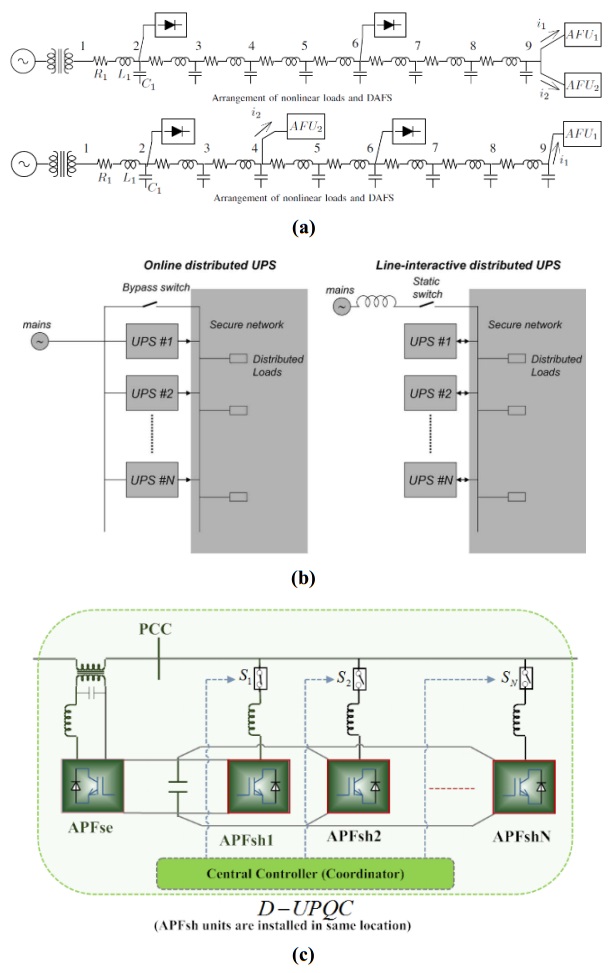
Cheng PT, Lee TL (2006) Distributed active filter systems (DAFSs): A new approach to power system harmonics. IEEE T Ind Appl 42: 1301–1309. doi: 10.1109/TIA.2006.880856
|
| [11] |
Guerrero JM, Hang L, Uceda J (2008) Control of distributed uninterruptible power supply systems. IEEE T Ind Electron 55: 2845–2859. doi: 10.1109/TIE.2008.924173
|
| [12] |
Lai J, Peng FZ (1996) Multilevel converters-a new breed of power converters. IEEE T Ind Appl 32: 509–517. doi: 10.1109/28.502161
|
| [13] |
Munoz JA, Espinoza JR, Moran LA, et al. (2009) Design of a modular UPQC configuration integrating a components economical analysis. IEEE T Power Deliver 24: 1763–1772. doi: 10.1109/TPWRD.2009.2028795
|
| [14] |
Peng FZ, Mckeever JW, Adams DJ (1998) A power line conditioner using cascade multilevel inverters for distribution systems. IEEE T Ind Appl 34: 1293–1298. doi: 10.1109/28.739012
|
| [15] |
Han B, Bae B, Baek S, et al. (2006) New configuration of UPQC for medium-voltage application. IEEE T Power Deliver 21: 1438–1444. doi: 10.1109/TPWRD.2005.860235
|
| [16] | Han B, Baek S, Kim H, et al. (2006) Dynamic characteristic analysis of SSSC based on multibridge inverter. IEEE Power Eng Rev 22: 62–63. |
| [17] |
Han BM, Mattavelli P (2003) Operation analysis of novel UPFC based on 3-level half-bridge modules. IEEE Power Tech Conference Proceedings, Bologna. IEEE 4: 307–312. doi: 10.1109/PTC.2003.1304740
|
| [18] | Munoz JA, Espinoza JR, Baier CR, et al. (2011) Design of a discrete-time linear control strategy for a multi-cell UPQC. IEEE T Ind Electron 59: 3797–3807. |
| [19] | Khadem MSK, Basu M, Conlon MF (2012) UPQC for power quality improvement in dg integrated smart grid network-a review. Int J Emerg Electr Power Syst 13: 3. |
| [20] |
Basu M, Das SP, Dubey GK (2008) Investigation on the performance of UPQC-Q for voltage sag mitigation and power quality improvement at a critical load point. IET Gener Transm Dis 2: 414–423. doi: 10.1049/iet-gtd:20060317
|
| [21] |
Khadem S, Basu M, Conlon M (2014) Harmonic power compensation capacity of shunt apf and its relationship to design parameters. IET Power Electron 7: 418–430. doi: 10.1049/iet-pel.2013.0098
|
| [22] |
Corradini L, Mattavelli P, Corradin M, et al. (2010) Analysis of parallel operation of uninterruptible power supplies loaded through long wiring cables. IEEE T Power Electr 25: 1046–1054. doi: 10.1109/TPEL.2009.2031178
|
| [23] |
Guerrero JM, Matas J, Castilla M, et al. (2006) Wireless-control strategy for parallel operation of distributed-generation inverters. IEEE T Ind Electron 53: 1461–1470. doi: 10.1109/TIE.2006.882015
|
| [24] | Khadem SK, Basu M, Conlon MF (2011) A review of parallel operation of active power filters in the distributed generation system. European Conference on Power Electronics and Applications. IEEE, 1–10. |
| [25] | Arrillaga J, Liu YH, Watson NR (2007) Self-commutating conversion, in flexible power transmission: The HVDC options. John Wiley & Sons, Ltd, Chichester, UK. |
| [26] | Khadem SK, Basu M, Conlon MF (2013) Selection of design parameters to reduce the zero-sequence circulating current flow in parallel operation of DC linked multiple shunt APF units. Adv Power Electron 2013: 13. |
| [27] |
Asiminoaei L, Aeloiza E, Enjeti PN, et al. (2008) Shunt active-power-filter topology based on parallel interleaved inverters. IEEE T Ind Electron 55: 1175–1189. doi: 10.1109/TIE.2007.907671
|
| [28] |
Chen TP (2012) Zero-sequence circulating current reduction method for parallel HEPWM inverters between AC bus and DC bus. IEEE T Ind Electron 59: 290–300. doi: 10.1109/TIE.2011.2106102
|
| [29] | Ye Z, Boroyevich D, Choi JY, et al. (2006) Control of circulating current in parallel three-phase boost rectifiers. Applied Power Electronics Conference and Exposition, 2000. IEEE 1: 506–512. |
| [30] |
Chen TP (2006) Circulating zero-sequence current control of parallel three-phase inverters. IEE P-Elect Pow Appl 153: 282–288. doi: 10.1049/ip-epa:20050231
|
| [31] | Abdelli Y, Machmoum M, Khoor MS (2004) Control of a multi module parallel able three phase active power filters. International Conference on Harmonics and Quality of Power. IEEE, 543–548. |
| [32] | Wei X, Dai K, Fang X, et al. (2006) Parallel control of three-phase three-wire shunt active power filters. Automat Electr Power Syst 31: 70–74. |

Figures(10) / Tables(3)

Shafiuzzaman Khan Khadem, Malabika Basu, Michael F. Conlon. Capacity enhancement and flexible operation of unified power quality conditioner in smart and microgrid network[J]. AIMS Energy, 2018, 6(1): 49-69. doi: 10.3934/energy.2018.1.49







 DownLoad:
DownLoad: