Citation: LauraM.Daniels, KimE.Dixon, LisaC.Campbell. Building Capacity for Behavioral Health Services and Clinical Research in a Rural Primary Care Clinic: A Case Study[J]. AIMS Public Health, 2014, 1(2): 60-75. doi: 10.3934/publichealth.2014.2.60

| [1] | Ziegelstein RC. (2001) Depression in patients recovering from a myocardial infarction. J Am Med Assoc ,286: 1621-1627. |
| [2] | Lustman PJ, Clouse RE. (2005) Depression in diabetic patients: The relationship between mood and glycemic control. J Diabetes Complica ,19: 113-122. |
| [3] | Loeppke R, Taitel M, Richling D, et al. (2007) Health and productivity as a business strategy. J Occup Environ Med ,49: 712-721. |
| [4] | Chiles J A, Lambert M J, Hatch A L (1999) The Impact of Psychological Interventions on Medical Cost Offset: A Meta‐analytic Review. Clin Psychol: Sci Pr ,6: 204-220. |
| [5] | Blount A, Schoenbaum M, Kathol R, et al. (2007) The economics of behavioral health services in medical settings: A summary of the evidence. Prof Psychol Res Pract ,38: 290-297. |
| [6] | Hunter C L, Goodie J L (2010) Operational and clinical components for integrated-collaborative behavioral healthcare in the patient-centered medical home. Fam Syst Health ,28: 308. |
| [7] | Gilbody S, Bower P, Fletcher J, et al. (2006) Collaborative care for depression: A cumulative meta-analysis and review of longer-term outcomes. Arch Intern Med ,166: 2314-2321. |
| [8] | Katon W, Von Korff M, Lin E, et al. (1995) Collaborative management to achieve treatment guidelines: Impact on depression in primary care. J Am Med Assoc ,273: 1026-1026. |
| [9] | Katon W, Unutzer J (2006) Collaborative care models for depression: Time to move from evidence to practice. Arch Intern Med ,166: 2304-2306. |
| [10] | Strosahl K. (1998) Integrating behavioral health and primary care services: The primary mental health care model. In A. Blount (Ed. ), Integrated primary care; The future of medical and mental health collaboration New York: W. W. Norton & Co, ,139-166. |
| [11] | Ockene JK, Edgerton EA, Teutsch SM, et al. (2007) Integrating evidence-based clinical and community strategies to improve health. Am J Prev Med. ,32: 244-252. |
| [12] | Taylor J (2004) The fundamentals of community health centers. National Health Policy Forum . |
| [13] | Butler M, Kane RL, McAlpine D, et al. (2008) Integration of mental health/substance abuse and primary care no. Integration of mental health/substance abuse and primary care no. 173 (prepared by the Minnesota Evidence-based Practice Center under contract no. 290-02-0009. ) (No. 09-E003) . |
| [14] | Robert Wood Johnson Foundation and University of Wisconsin Population Health Institute (2013) County Health Rankings. Available from http://www. countyhealthrankings. org/app/home . |
| [15] | Log Into North Carolina (LINC) Database (2011) Office of State Planning, NC Office of the Governor. Available from http://linc.state.nc.us/ . |
| [16] | Yin R. (2011) Applications of case study research. Los Angeles: Sage . |
| [17] | Czarniawska B. (2004) Narratives in social science research. London: Sage . |
| [18] | Yin R. (2009) Case study research: Design and methods. Los Angeles: Sage . |
| [19] | North Carolina Center for Excellence in Integrated Care. (2012) WNC Depression Algorithm.43. |
| [20] | Kroenke K, Spitzer RL, Williams JBW. (2001) The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med ,16: 606-613. |
| [21] | Lustman PJ, Anderson RJ, Freedland KE, et al. (2000) Depression and poor glycemic control: a meta-analytic review of the literature. Diabetes care ,23: 934-942. |
| [22] | Lustman P J, Clouse R E (2004) Section III: Practical Considerations in the management of depression in diabetes. Diabetes Spectrum ,17: 160-166. |
| [23] | Blount A. (Ed. ) (1998) Integrated primary care: The future of medical and mental health collaboration. New York: W. W. Norton & Co . |
| [24] | McDaniel SH, Campbell TL, Hepworth J. (2005) Family-oriented primary care. Family-oriented primary care . |
| [25] | Wagner E, Austin B, Davis C, et al. (2001) Improving chronic illness care: Translating evidence into action. Health Affair ,20: 64-78. |
| [26] | Hunter CL, Goodie JL, Oordt MS, et al. (2009) Integrated behavioral health in primary care: Step-by-step guidance for assessment and intervention. Washington, DC: American Psychological Association . |
| [27] | Funderburk JS, Sugarman DE, Labbe AK, et al. (2011) Behavioral health interventions being implemented in a VA primary care system. J Clin Psychol Med S ,18: 22-29. |
| [28] | Korsen N, Pietruszewski P (2009) Translating evidence to practice: Two stories from the field. J Clin Psychol Med S ,16: 47-57. |
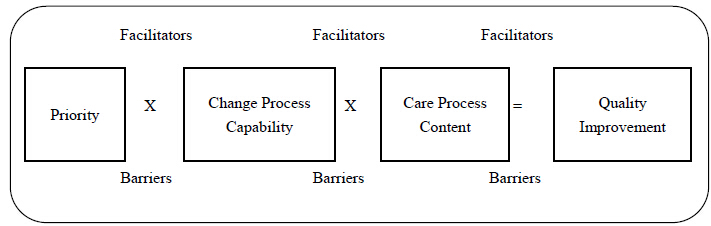
| [29] | Solberg LI. (2007) Improving medical practice: A conceptual framework. Ann Fam Med ,5: 251-256. |
| [30] | Peek CJ. (2008) Planning care in the clinical, operational, and financial worlds. In R. Kessler, & D. Stafford (Eds. ), Collaborative medicine case studies: Evidence in practice. New York: Springer . |
| [31] | Solberg LI, Asche SE, Margolis KL, et al. (2008) Measuring an organization's ability to manage change: the change process capability questionnaire and its use for improving depression care. Am J Med Qual ,23: 193-200. |
| [32] | Brownson RC, Colditz GA, Proctor EK. (2012) Dissemination and implementation research in health: Translating science to practice. New York: Oxford University Press, Inc . |
| [33] | Meissner HI, Glasgow RI, Vinson CA, et al. (2013) The U. S. training institute for dissemination and implementation research in health. Implement Sci ,8: 1-9. |
Figures(2)

LauraM.Daniels, KimE.Dixon, LisaC.Campbell. Building Capacity for Behavioral Health Services and Clinical Research in a Rural Primary Care Clinic: A Case Study[J]. AIMS Public Health, 2014, 1(2): 60-75. doi: 10.3934/publichealth.2014.2.60







 DownLoad:
DownLoad: