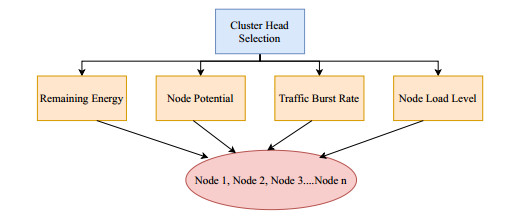
Network congestion may occur naturally or intentionally caused by selfish nodes. Existing congestion control techniques designed by researchers for sensor-based networks have primarily focused on natural modes of congestion occurrence and ignored malevolent nodes' potential for purposeful congestion-like scenario creation. In light of this fact, a security attack-resistant congestion control method that takes into account both possible sources of congestion in sensor nodes has been developed. So firstly, a trust-based technique has been developed to get rid of selfish nodes' intentional attempts to cause congestion. After the elimination of malicious nodes, a congestion avoidance method has been applied which tries to prevent the natural way of congestion occurrence. For this purpose, we have applied a multi-criteria decision-making method as there are many factors responsible for congestion occurrence. The remaining energy, node potential value, node load factor, and traffic burst rate have been considered as decision factors. Simulation results show that our Security Aware Congestion Control technique using the AHP method (SACC-AHP) outperforms the existing relevant techniques LEACH, TCEER, TASRP, CARA and SACC in terms of energy efficiency, security, packet delivery ratio and network lifetime.
Citation: Divya Pandey, Vandana Kushwaha. The use of Analytical Hierarchy Process in sensor-based networks for security-aware congestion control[J]. Networks and Heterogeneous Media, 2023, 18(1): 244-274. doi: 10.3934/nhm.2023009
Network congestion may occur naturally or intentionally caused by selfish nodes. Existing congestion control techniques designed by researchers for sensor-based networks have primarily focused on natural modes of congestion occurrence and ignored malevolent nodes' potential for purposeful congestion-like scenario creation. In light of this fact, a security attack-resistant congestion control method that takes into account both possible sources of congestion in sensor nodes has been developed. So firstly, a trust-based technique has been developed to get rid of selfish nodes' intentional attempts to cause congestion. After the elimination of malicious nodes, a congestion avoidance method has been applied which tries to prevent the natural way of congestion occurrence. For this purpose, we have applied a multi-criteria decision-making method as there are many factors responsible for congestion occurrence. The remaining energy, node potential value, node load factor, and traffic burst rate have been considered as decision factors. Simulation results show that our Security Aware Congestion Control technique using the AHP method (SACC-AHP) outperforms the existing relevant techniques LEACH, TCEER, TASRP, CARA and SACC in terms of energy efficiency, security, packet delivery ratio and network lifetime.

| [1] |
J. Yick, B. Mukherjee, D. Ghosal, Wireless sensor network survey, Comput. Netw., 52 (2008), 2292–2330. https://doi.org/10.1016/j.comnet.2008.04.002 doi: 10.1016/j.comnet.2008.04.002

|
| [2] |
C. F. Cheng, Y. C. Chen, J. C. W. Lin, A carrier-based sensor deployment algorithm for perception layer in the IoT architecture, IEEE. Sens. J., 20 (2020), 10295–10305. https://doi.org/10.1109/JSEN.2020.2989871 doi: 10.1109/JSEN.2020.2989871
|
| [3] |
M. Majid, S. Habib, A. R. Javed, M. Rizwan, G. Srivastava, T. R. Gadekallu, J. C. W. Lin, Applications of wireless sensor networks and internet of things frameworks in the industry revolution 4.0: a systematic literature review, Sensors-Basel., 22 (2022), 2087. https://doi.org/10.3390/s22062087 doi: 10.3390/s22062087
|
| [4] | N. Labraoui, M. Gueroui, L. Sekhri, On-off attacks mitigation against trust systems in wireless sensor networks, In: A. Amine, L. Bellatreche, Z. Elberrichi, E. J. Neuhold, and R. Wrembel, Computer Science and Its Applications, CIIA 2015, IFIP Advances in Information and Communication Technology, Springer, Cham, (2015), 406–415. |
| [5] |
J. C. W. Lin, P. Fournier-Viger, L. Wu, W. Gan, Y. Djenouri, J. Zhang, PPSF: an open-source privacy-preserving and security mining framework, 2018 IEEE International Conference on Data Mining Workshops (ICDMW) (2018), 1459–1463. https://doi.org/10.1109/ICDMW.2018.00208 doi: 10.1109/ICDMW.2018.00208
|
| [6] | J. Zheng, A. Jamalipour, Wireless Sensor Networks: A Networking Perspective, John Wiley and Sons, Ltd, (2009). https://doi.org/10.1002/9780470443521 |
| [7] |
D. Pandey, V. Kushwaha, An exploratory study of congestion control techniques in wireless sensor networks, Comput. Commun., 157 (2020), 257–283. https://doi.org/10.1016/j.comcom.2020.04.032 doi: 10.1016/j.comcom.2020.04.032
|
| [8] |
L. Q. Tao, F. Q. Yu, ECODA: enhanced congestion detection and avoidance for multiple class of traffic in sensor networks, IEEE. T. Consum. Electr., 56 (2010), 1387–1394. https://doi.org/10.1109/TCE.2010.5606274 doi: 10.1109/TCE.2010.5606274
|
| [9] |
F. Ren, T. He, S. K. Das, C. Lin, Traffic-aware dynamic routing to alleviate congestion in wireless sensor networks, IEEE. T. Parall. Distr., 22 (2011), 1585–1599. https://doi.org/10.1109/TPDS.2011.24 doi: 10.1109/TPDS.2011.24
|
| [10] |
C. Sergiou, V. Vassiliou, A. Paphitis, Hierarchical tree alternative path (HTAP) algorithm for congestion control in wireless sensor networks, Ad. Hoc. Netw., 11 (2013), 257–272. https://doi.org/10.1016/j.adhoc.2012.05.010 doi: 10.1016/j.adhoc.2012.05.010
|
| [11] |
A. A. Rezaee, M. H. Yaghmaee, A. M. Rahmani, A. H. Mohajerzadeh, HOCA: Healthcare aware optimized congestion avoidance and control protocol for wireless sensor networks, J. Netw. Comput. Appl., 37 (2014), 216–228. https://doi.org/10.1016/j.jnca.2013.02.014 doi: 10.1016/j.jnca.2013.02.014
|
| [12] | L. Tshiningayamwe, G. A. Lusilao-Zodi, M. E. Dlodlo, A priority rate-based routing protocol for wireless multimedia sensor networks, In: N. Pillay, A. P. Engelbrecht, A. Abraham, M. C. du Plessis, V. Snášel, and A. K. Muda, Advances in Nature and Biologically Inspired Computing, Advances in Intelligent Systems and Computing, Springer, Cham, (2016), 347–358. |
| [13] |
P. K. Donta, T. Amgoth, C. S. R. Annavarapu, Congestion-aware data acquisition with q-learning for wireless sensor networks, 2020 IEEE International IOT, Electronics and Mechatronics Conference (IEMTRONICS) (2020), 1–6, https://doi.org/10.1109/IEMTRONICS51293.2020.9216379 doi: 10.1109/IEMTRONICS51293.2020.9216379
|
| [14] | K. Sohraby, D. Minoli, T. Znati, Wireless Sensor Networks: Technology, Protocols, and Applications, John wiley and sons, (2007). |
| [15] |
A. Srivastava, P. K. Mishra, Multi-attributes based energy efficient clustering for enhancing network lifetime in WSN's, Peer. Peer. Netw. Appl., 15 (2022), 2670–2693. https://doi.org/10.1007/s12083-022-01357-w doi: 10.1007/s12083-022-01357-w
|
| [16] |
V. Kushwaha, Ratneshwer, A review of router based congestion control algorithms, Int. J. Comput. Netw. Inf. Secur., 1 (2014), 1–10. https://doi.org/10.5815/ijcnis.2014.01.01 doi: 10.5815/ijcnis.2014.01.01
|
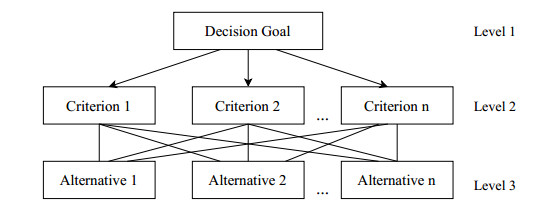
| [17] | T. L. Saaty, Decision making with the analytic hierarchy process, Int. J. Serv. Sci., 1 (2008), 83–98. |
| [18] | M. M. Momani, Bayesian Methods for Modelling and Management of Trust in Wireless Sensor Networks, University of Technology, Sydney, (2008). |
| [19] |
P. Rodrigues, J. John, Joint trust: an approach for trust-aware routing in WSN, Wirel. Netw., 26 (2020), 3553–3568. https://doi.org/10.1007/s11276-020-02271-w doi: 10.1007/s11276-020-02271-w
|
| [20] |
Y. Tao, X. Xu, P. Li, T. Li, L. Pan, A secure routing of wireless sensor networks based on trust evaluation model, Procedia. Comput. Sci., 131 (2018), 1156–1163. https://doi.org/10.1016/j.procs.2018.04.289 doi: 10.1016/j.procs.2018.04.289
|
| [21] |
X. Yin, S. Li, Trust evaluation model with entropy-based weight assignment for malicious node's detection in wireless sensor networks, EURASIP. J. Wirel. Comm., 198 (2019). https://doi.org/10.1186/s13638-019-1524-z doi: 10.1186/s13638-019-1524-z
|
| [22] |
T. Kalidoss, L. Rajasekaran, K. Kanagasabai, G. Sannasi, A. Kannan, QoS aware trust based routing algorithm for wireless sensor networks, Wireless. Pers. Commun., 110 (2020), 1637–1658. https://doi.org/10.1007/s11277-019-06788-y doi: 10.1007/s11277-019-06788-y
|
| [23] |
A. Tajeddine, A. Kayssi, A. Chehab, I. Elhajj, W. Itani, CENTERA: a centralized trust-based efficient routing protocol with authentication for wireless sensor networks, Sensors-Basel., 15 (2015), 3299–3333. https://doi.org/10.3390/s150203299 doi: 10.3390/s150203299
|
| [24] |
T. Khan, K. Singh, M. H. Hasan, K. Ahmad, G. T. Reddy, S. Mohan, A. Ahmadian, ETERS: A comprehensive energy aware trust-based efficient routing scheme for adversarial WSNs, Future. Gener. Comp. Sy., 125 (2021), 921–943. https://doi.org/10.1016/j.future.2021.06.049 doi: 10.1016/j.future.2021.06.049
|
| [25] |
M. Selvi, K. Thangaramya, S. Ganapathy, K. Kulothungan, H. K. Nehemiah, A. Kannan, An energy aware trust based secure routing algorithm for effective communication in wireless sensor networks, Wireless. Pers. Commun., 105 (2019), 1475–1490. https://doi.org/10.1007/s11277-019-06155-x doi: 10.1007/s11277-019-06155-x
|
| [26] |
E. Thenmozhi, S. Audithan, Trust based cluster and secure routing scheme for wireless sensor network, Second International Conference on Current Trends In Engineering and Technology–ICCTET 2014, (2014), 489–494. https://10.1109/ICCTET.2014.6966345 doi: 10.1109/ICCTET.2014.6966345
|
| [27] |
N. A. Khalid, Q. Bai, A. Al-Anbuky, Adaptive trust-based routing protocol for large scale WSNs, IEEE. Access. 7 (2019), 143539–143549. https://10.1109/ACCESS.2019.2944648 doi: 10.1109/ACCESS.2019.2944648
|
| [28] |
D. C. Mehetre, S. E. Roslin, S. J. Wagh, Detection and prevention of Black Hole and selective forwarding attack in clustered WSN with active trust, Cluster. Comput., 22 (2019), 1313–1328. https://doi.org/10.1007/s10586-017-1622-9 doi: 10.1007/s10586-017-1622-9
|
| [29] |
W. Fang, W. Zhang, W. Yang, Z. Li, W. Cao, Y. Yang, Trust management-based and energy efficient hierarchical routing protocol in wireless sensor networks, Digit. Commun. Netw., 7 (2021), 470–478. https://doi.org/10.1016/j.dcan.2021.03.005 doi: 10.1016/j.dcan.2021.03.005
|
| [30] |
N. Dharini, N. Duraipandian, J. Katiravan, ELPC-trust framework for wireless sensor networks, Wireless. Pers. Commun., 113 (2020), 1709–1742. https://doi.org/10.1007/s11277-020-07288-0 doi: 10.1007/s11277-020-07288-0
|
| [31] |
M. Rathee, S. Kumar, A. H. Gandomi, K. Dilip, B. Balusamy, R. Patan, Ant colony optimization based quality of service aware energy balancing secure routing algorithm for wireless sensor networks, IEEE. T. Eng. Manage., 68 (2019), 170–182. https://doi.org/10.1109/TEM.2019.2953889 doi: 10.1109/TEM.2019.2953889
|
| [32] |
M. U. Ghazi, S. S. H. Naqvi, K. Yamin, O. Humayun, Congestion-aware routing algorithm based on traffic priority in wireless sensor networks, 2018 15th International Conference on Smart Cities: Improving Quality of Life Using ICT and IoT (HONET-ICT), (2018), 112–116. https://doi.org/10.1109/HONET.2018.8551337 doi: 10.1109/HONET.2018.8551337
|
| [33] |
J. Yan, B. Qi, CARA: a congestion-aware routing algorithm for wireless sensor networks, Algorithms., 14 (2021), 199. https://doi.org/10.3390/a14070199 doi: 10.3390/a14070199
|
| [34] |
H. S. Das, S. Bhattacharjee, A congestion aware routing for lifetime improving in grid-based sensor networks, J. High. Speed. Netw., 23 (2017), 1–14. https://doi.org/10.3233/JHS-170553 doi: 10.3233/JHS-170553
|
| [35] |
G. Sangeetha, M. Vijayalakshmi, S. Ganapathy, A. Kannan, An improved congestion-aware routing mechanism in sensor networks using fuzzy rule sets, Peer. Peer. Netw. Appl., 13 (2020), 890–904. https://doi.org/10.1007/s12083-019-00821-4 doi: 10.1007/s12083-019-00821-4
|
| [36] | S. S. Babu, A. Raha, M. K. Naskar, Geometric mean based trust management system for WSNs (GMTMS), in 2011 World Congress on Information and Communication Technologies, (2011), 444–449. https://doi.org/10.1109/WICT.2011.6141286 |
| [37] | S. Ganguly, A. Chakraborty, M. K. Naskar, A trust-based framework for congestion-aware energy efficient routing in wireless multimedia sensor networks, (2013). https://doi.org/10.48550/arXiv.1312.4071 |
| [38] |
J. Duan, D. Yang, H. Zhu, S. Zhang, J. Zhao, TSRF: a trust-aware secure routing framework in wireless sensor networks, Int. J. Distrib. Sens. N., 10 (2014), 209436. https://doi.org/10.1155/2014/209436 doi: 10.1155/2014/209436
|
| [39] |
X. Wu, J. Huang, J. Ling, L. Shu, BLTM: beta and LQI based trust model for wireless sensor networks, IEEE. Access., 7 (2019), 43679–43690. https://doi.org/10.1109/ACCESS.2019.2905550 doi: 10.1109/ACCESS.2019.2905550
|
| [40] |
M. Gholipour, A. T. Haghighat, M. R. Meybodi, Congestion avoidance in cognitive wireless sensor networks using TOPSIS and response surface methodology, Telecommun. Syst., 67 (2018), 519–537. https://doi.org/10.1007/s11235-017-0356-6 doi: 10.1007/s11235-017-0356-6
|
| [41] |
K. Sumathi, P. Pandiaraja, Dynamic alternate buffer switching and congestion control in wireless multimedia sensor networks, Peer. Peer. Netw. Appl., 13 (2020), 2001–2010. https://doi.org/10.1007/s12083-019-00797-1 doi: 10.1007/s12083-019-00797-1
|
| [42] |
S. Li, Q. Xu, J. Gaber, Z. Dou, J. Chen, Congestion control mechanism based on dual threshold DI-RED for WSNs, Wireless. Pers. Commun., 115 (2020), 2171–2195. https://doi.org/10.1007/s11277-020-07676-6 doi: 10.1007/s11277-020-07676-6
|
| [43] |
A. Beheshtiasl, A. Ghaffari, Secure and trust-aware routing scheme in wireless sensor networks, Wireless. Pers. Commun., 107 (2019), 1799–1814. https://doi.org/10.1007/s11277-019-06357-3 doi: 10.1007/s11277-019-06357-3
|
| [44] |
S. Qu, L. Zhao, Y. Chen, W. Mao, A discrete-time sliding mode congestion controller for wireless sensor networks, Optik., 225 (2021), 165727. https://doi.org/10.1016/j.ijleo.2020.165727 doi: 10.1016/j.ijleo.2020.165727
|
| [45] |
S. Sefati, M. Abdi, A. Ghaffari, Cluster‐based data transmission scheme in wireless sensor networks using black hole and ant colony algorithms, Int. J. Commun. Syst., 34 (2012), e4768. https://doi.org/10.1002/dac.4768 doi: 10.1002/dac.4768
|
| [46] |
W. R. Heinzelman, A. Chandrakasan, H. Balakrishnan, Energy-efficient communication protocol for wireless microsensor networks, Proceedings of The 33rd Annual Hawaii International Conference on System Sciences (2000). https://doi.org/10.1109/HICSS.2000.926982 doi: 10.1109/HICSS.2000.926982
|
| [47] |
G. Srivastava, J. C. W. Lin, M. Pirouz, Y. Li, U. Yun, A pre-large weighted-fusion system of sensed high-utility patterns, IEEE. Sens. J., 21 (2020), 15626–15634. https://doi.org/10.1109/JSEN.2020.2991045 doi: 10.1109/JSEN.2020.2991045
|
| [48] |
T. Khan, K. Singh, TASRP: a trust aware secure routing protocol for wireless sensor networks, Int. J. Innov. Comput. Appl., 12 (2021), 108–122. https://doi.org/10.1504/ijica.2021.113750 doi: 10.1504/ijica.2021.113750
|
| [49] |
P. Chanak, I. Banerjee, Congestion free routing mechanism for IoT-enabled wireless sensor networks for smart healthcare applications. IEEE. T. Consum. Electr., 66 (2020), 223–232. https://doi.org/10.1109/TCE.2020.2987433 doi: 10.1109/TCE.2020.2987433
|
| [50] |
T. Gao, R. C. Jin, J. Y. Song, T. B. Xu, L. D. Wang, Energy-efficient cluster head selection scheme based on multiple criteria decision making for wireless sensor networks, Wireless. Pers. Commun., 63 (2012), 871–894. https://doi.org/10.1007/s11277-010-0172-8 doi: 10.1007/s11277-010-0172-8
|
| [51] |
P. Mukherjee, P. K. Pattnaik, A. A. Al-Absi, D. K. Kang, Recommended system for cluster head selection in a remote sensor cloud environment using the fuzzy-based multi-criteria decision-making technique, Sustainability-Basel., 13 (2021), 10579. https://doi.org/10.3390/su131910579 doi: 10.3390/su131910579
|
| [52] |
R. K. Dewi, B. T. Hanggara, A. Pinandito, A comparison between AHP and hybrid AHP for mobile based culinary recommendation system, Int. J. Interact. Mob. Technol., 12 (2018), 133–140. https://doi.org/10.3991/ijim.v12i1.7561 doi: 10.3991/ijim.v12i1.7561
|
Figures(10) / Tables(7)
Divya Pandey, Vandana Kushwaha. The use of Analytical Hierarchy Process in sensor-based networks for security-aware congestion control[J]. Networks and Heterogeneous Media, 2023, 18(1): 244-274. doi: 10.3934/nhm.2023009







 DownLoad:
DownLoad: