Citation: Misato Kuroyanagi, Yoshimitsu Kuroyanagi. Tissue-engineered products capable of enhancing wound healing[J]. AIMS Materials Science, 2017, 4(3): 561-581. doi: 10.3934/matersci.2017.3.561

| [1] |
Clark RAF (1985) Cutaneous tissue repair: basic biological considerations. I. J Am Acad Dermatol 13: 701–725. doi: 10.1016/S0190-9622(85)70213-7

|
| [2] |
Falanga V, Grinnel F, Gilchrest B, et al. (1995) Experimental approaches to chronic wounds. Wound Repair Regen 3: 132–140. doi: 10.1046/j.1524-475X.1995.30205.x
|
| [3] |
Yager DR, Zhang LY, Liang HX, et al. (1996) Wound fluids from human pressure ulcers contain elevated matrix metalloproteinase levels and activity compared to surgical wound fluids. J Invest Dermatol 107: 743–748. doi: 10.1111/1523-1747.ep12365637
|
| [4] |
Yager DR, Chen SM, Ward SI, et al. (1997) Ability of chronic wound fluids to degrade peptide growth factors is associated with increased levels of elastase activity and diminished levels of proteinase inhibitors. Wound Repair Regen 5: 23–32. doi: 10.1046/j.1524-475X.1997.50108.x
|
| [5] | Weckroch M, Vaheri A, Lauharanta J, et al. (1996) Matrix metalloproteinases, gelatinase, and collagenase in chronic leg ulcers. J Invest Dermatol 109: 1119–1124. |
| [6] |
Wysocki AB, Staiano-Coico L, Grinnel F (1993) Wound fluid from chronic leg ulcers contains elevated levels of metalloproteinase MMP-2 and MMP-9. J Invest Dermatol 101: 64–68. doi: 10.1111/1523-1747.ep12359590
|
| [7] |
Rheinwald JG, Green H (1977) Epidermal growth factor and the multiplication of cultured human epidermal keratinocytes. Nature 265: 421–424. doi: 10.1038/265421a0
|
| [8] |
Green H, Kehinde O, Thomas J (1979) Growth of cultured human epidermal cells into multiple epithelia suitable for grafting. P Natl Acad Sci USA 76: 5665–5668. doi: 10.1073/pnas.76.11.5665
|
| [9] | O'Connor NE, Muliken JG, Banks-Schlegel S, et al. (1982) Grafting of burns with cultured epithelium prepared from autologous epidermal cells. Lancet 1: 75–78. |
| [10] |
Gallico GG, O'Connor NE, Compton CC, et al. (1984) Permanent coverage of large burn wounds with autologous cultured human epithelium. New Engl J Med 311: 448–451. doi: 10.1056/NEJM198408163110706
|
| [11] | Cuono CB, Langdon R, McGuire J (1986) Use of cultured epidermal autografts and dermal allografts as skin replacement ater burn injury. Lancet 1: 1123–1124. |
| [12] | Compton CC, Gill JM, Bradford DA, et al. (1989) Skin regenerated from cultured epithelial autografts on full-thickness burn wounds frm 6 days to 5 years after grafting. Lab Invest 60: 600–612. |
| [13] |
Gallico GG, O'Connor NE, Compton CC (1989) Cultured epithelial autografts for giant congenital nevi. Plast Reconstr Surg 84: 1–9. doi: 10.1097/00006534-198907000-00001
|
| [14] |
De Luca M, Albanese E, Bondanza S, et al. (1989) Multicenter experience in the treatment of burns with autologous and allogenic cultured epithelium, fresh or preserved in a frozen state. Burns 15: 303–309. doi: 10.1016/0305-4179(89)90007-7
|
| [15] |
Odessey R (1992) Addendum: Multicenter experience with cultured epidermal autograft for treatment of burns. J Burn Care Res 13: 174–180. doi: 10.1097/00004630-199201000-00038
|
| [16] |
Bell E, Ehrlich HP, Buttle DJ, et al. (1981) Living tissue formed in vitro and accepted as skin-equivalent tissue of full thickness. Science 211: 1052–1054. doi: 10.1126/science.7008197
|
| [17] |
Bell E, Ehrlich HP, Sher S, et al. (1981) Development and use of a living skin equivalent. Plast Reconstr Surg 67: 386–392. doi: 10.1097/00006534-198103000-00024
|
| [18] |
Bell E, Sher S, Hull B, et al. (1983) The reconstitution of living skin. J Invest Dermatol 81: 2–10. doi: 10.1111/1523-1747.ep12537381
|
| [19] | Parenteau N, Naughton G (1999) Skin: the first tissue-engineered products. Sci Am 83-85. |
| [20] |
Kuroyanagi Y, Kubo K, Matsui H, et al. (2004) Establishment of banking system for allogeneic cultured dermal substitute. Artif Organs 28: 13–21. doi: 10.1111/j.1525-1594.2004.07318.x
|
| [21] |
Kubo K, Kuroyanagi Y (2005) A study of cytokines released from fibroblasts in cultured dermal subsitute. Artif Organs 29: 845–849. doi: 10.1111/j.1525-1594.2005.00138.x
|
| [22] |
Hashimoto A, Kuroyanagi Y (2008) Standardization for mass production of allogeneic cultured dermal substitute by measuring the amount of VEGF, bFGF, HGF, TGF-β, and IL-8. J Artif Organs 11: 225–231. doi: 10.1007/s10047-008-0436-1
|
| [23] |
Kashiwa N, Ito O, Ueda T, et al. (2004) Treatment of full-thickness skin defect with concomitant grafting of 6-fold extended mesh auto-skin and allogeneic cultured dermal substitute. Artif Organs 28: 444–450. doi: 10.1111/j.1525-1594.2004.00009.x
|
| [24] | Ohtani T, Okamoto K, Kaminaka C, et al. (2004) Digital gangrene associated with idiopathic hypereosinophilia: treatment with allogeneic cultured dermal substitute (CDS). Eur J Dermatol 14: 168–171. |
| [25] | Moroi Y, Fujita S, Fukagawa S, et al. (2004) Clinical evaluation of allogeneic cultured dermal substitutes for intractable skin ulcers after tumor resection. Eur J Dermatol 14: 172–176. |
| [26] |
Yamada N, Uchinuma E, Kuroyanagi Y (2008) Clinical trial of allogeneic cultured dermal substitute for intractable skin ulcers of the lower leg. J Artif Organs 11: 100–103. doi: 10.1007/s10047-008-0406-7
|
| [27] |
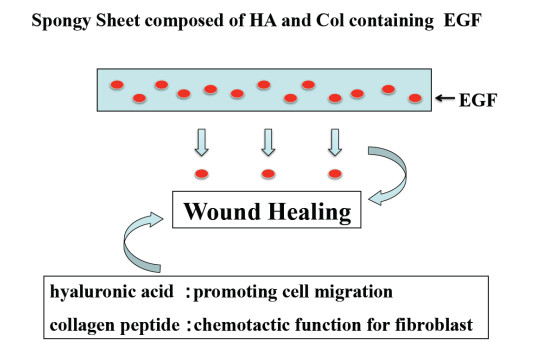
Chen WYJ, Abatangelo G (1999) Functions of hyaluronan in wound repair. Wound Repair Regen 7: 79–89. doi: 10.1046/j.1524-475X.1999.00079.x
|
| [28] |
West DC, Hampson IN, Arnold F, et al. (1985) Angiogenesis induced by degradation products of hyaluronic acid. Science 228: 1324–1326. doi: 10.1126/science.2408340
|
| [29] |
Sattar A, Rooney P, Kumar S, et al. (1994) Application of angiogenic oligosaccharides of hyaluronan increases blood vessel numbers in rat skin. J Invest Dermatol 103: 576–579. doi: 10.1111/1523-1747.ep12396880
|
| [30] | Lees VC, Fan TP, West DC (1995) Angiogenesis in a delayed revascularization model is accelerated by angiogenic oligosaccharides of hyaluronan. Lab Invest 73: 259–266. |
| [31] |
Pardue EL, Ibrahim S, Ramamurthi A (2008) Role of hyaluronan in angiogenesis and its utility to angiogenic tissue engineering. Organogenesis 4: 203–214. doi: 10.4161/org.4.4.6926
|
| [32] | Postlethwaite AE, Seyer JM, Kang AH (1978) Chemotactic attraction of human fibroblasts to type I, II, and III collagens and collagen-derived peptides. P Natl Acad Sci USA 78: 871–875. |
| [33] |
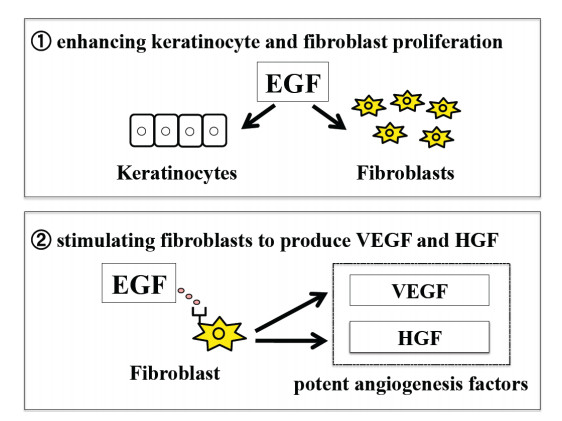
Carpenter G, Cohen S (1976) Human epidermal growth factor and the proliferation of human fibroblasts. J Cell Physiol 88: 227–237. doi: 10.1002/jcp.1040880212
|
| [34] |
Carpenter G, Cohen S (1979) Epidermal growth factor. Annu Rev Biochem 48: 193–216. doi: 10.1146/annurev.bi.48.070179.001205
|
| [35] |
Park JS, Kim JY, Cho JY, et al. (2000) Epidermal growth factor (EGF) antagonizes transforming growth factor (TGF)-beta 1-induced collagen lattice contraction by human skin fibroblasts. Biol Pharm Bull 23: 1521–1523. doi: 10.1248/bpb.23.1521
|
| [36] |
Xin X, Yang S, Ingle G, et al. (2001) Hepatocyte growth factor enhances vascular endothelial growth factor-induce angiogenesis in vitro and in vivo. Am J Pathol 158: 1111–1120. doi: 10.1016/S0002-9440(10)64058-8
|
| [37] |
Conway K, Price P, Harding KG, et al. (2006) The molecular and clinical impact of hepatocyte growth factor, its receptor, activators, and inhibitors in wound healing. Wound Repair Regen 14: 2–10. doi: 10.1111/j.1524-475X.2005.00081.x
|
| [38] |
Kondo S, Kuroyanagi Y (2012) Development of wound dressing composed of hyaluronic acid and collagen sponge with epidermal growth factor. J Biomat Sci-Ploym E 23: 629–643. doi: 10.1163/092050611X555687
|
| [39] | Kondo S, Niiyama H, Yu A, et al. (2012) Evaluation of a wound dressing composed of hyaluronic acid and collagen sponge containing epidermal growth factor in diabetic mice. J Biomat Sci-Ploym E 23: 1729–1740. |
| [40] |
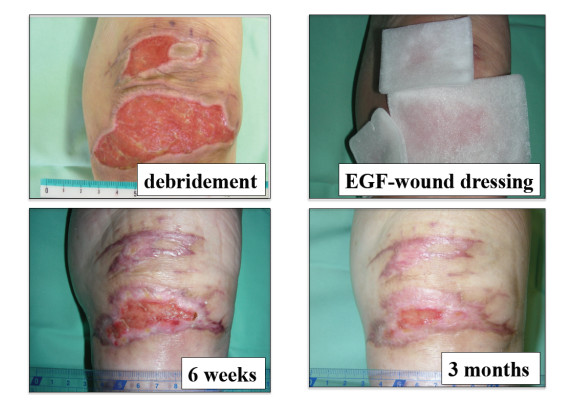
Yu A, Takeda A, Kumazawa K, et al. (2015) Preliminary clinical study using a novel wound dressing composed of hyaluronic acid and collagen containing EGF. Open J Regen Med 4: 6–13. doi: 10.4236/ojrm.2015.41002
|
| [41] | Wolfort FG, Dalton WE, Hoopes JE (1972) Chemical peel with trichloroacetic acid. Brit J Plast Surg 25: 333–334. |
| [42] |
Baker TJ, Gordon HL, Mosienko P, et al. (1974) Longterm histological study of skin after chemical peeling. Plast Reconstr Surg 53: 522–525. doi: 10.1097/00006534-197405000-00003
|
| [43] |
Coleman WP, Brody HJ (1997) Advances in chemical peeling. Dermatol Clin 15: 19–26. doi: 10.1016/S0733-8635(05)70411-3
|
| [44] |
Brody HJ, Monheit GD, Resnik SS, et al. (2000) A history of chemical peeling. Dermatol Surg 26: 405–409. doi: 10.1046/j.1524-4725.2000.00505.x
|
| [45] |
Anitha B (2010) Prevention of complications in chemical peeling. J Cutan AesthetSurg 3: 186–188. doi: 10.4103/0974-2077.74500
|
| [46] |
Cui XL, Iwasa M, Iwasa Y, et al. (2000) Arginine-supplemented diet decreases expression of inflammatory cytokines and improves survival in burned rats. JPEN 24: 89–96. doi: 10.1177/014860710002400289
|
| [47] |
Ochoa JB, Strange J, Kearney P, et al. (2001) Effects of L-arginine on the proliferation of T lymphocyte subpopulations. JPEN 25: 23–29. doi: 10.1177/014860710102500123
|
| [48] |
Kirs SJ, Barbul A (1990) Role of arginine in trauma, sepsis, and immunity. JPEN 14: 226–229. doi: 10.1177/014860719001400514
|
| [49] |
Shi HP, Efron DT, Most D, et al. (2000) Supplemental dietary arginine enhances wound healing in normal but not inducible nitric oxide synthase knockout mice. Surgery 128: 374–378. doi: 10.1067/msy.2000.107372
|
| [50] |
Zhu H, Ka B, Murad F (2007) Nitric oxide accelerates the recovery from burn wounds. World J Surg 31: 624–631. doi: 10.1007/s00268-007-0727-3
|
| [51] |
Witte MB, Barbul A (2003) Arginine physiology and its implication for wound healing. Wound Repair Regen 11: 419–423. doi: 10.1046/j.1524-475X.2003.11605.x
|
| [52] |
Matsumoto Y, Arai K, Momose H, et al. (2009) Development of wound dressing composed of hyaluronic acid sponge containing arginine. J Biomat Sci-Polym E 20: 993–1004. doi: 10.1163/156856209X444394
|
| [53] | Marionnet C, Vioux-chagnoleau C, Pierrard C, et al. (2006) Morphogenesis of dermal-epidermal junction in a model of reconstracted skin: beneficial effects of vitamin C. Exp Dermatol 15: 625–633. |
| [54] |
Lima CC, Pereira APC, Silva JRF, et al. (2009) Ascorbic acid for the healing of skin wounds in rats. Braz J Biol 69: 1195–1201. doi: 10.1590/S1519-69842009000500026
|
| [55] |
Wu YL, Gohda E, Iwao M, et al. (1998) Stimulation of hepatocyte growth factor production by ascorbic acid and its stable 2-glucoside. Growth Horm IGF Res 8: 421–428. doi: 10.1016/S1096-6374(98)80313-4
|
| [56] | Niiyama H, Kuroyanagi Y (2014) Development of novel wound dressing composed of hyaluronic acid and collagen sponge containing epidermal growth factor and vitamin C derivative. J Artif Organs 17: 81–87. |
| [57] |
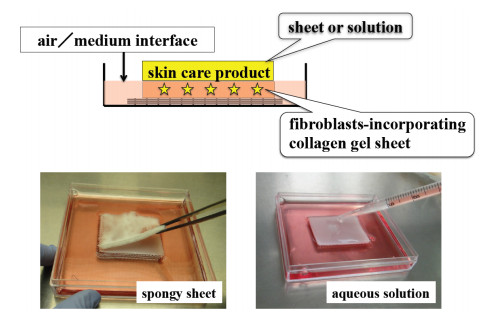
Yamamoto A, Ohno H, Kuroyanagi Y (2016) Evaluation of epidermal growth factor-incorporating skin care product in culture experiment using human fibroblasts. Open J Regen Med 5: 44–54. doi: 10.4236/ojrm.2016.52004
|
| [58] | Mitchell JD, Lee R, Hodakowski GT, et al. (1994) Prevention of postoperative pericardial adhesions with a hyaluronic acid coating solution: Experimental safety and efficacy studies. J Thorac Cardiov Sur 107: 1481–1488. |
| [59] |
Harris ES, Morgan RF, Rodeheaver GT (1995) Analysis of the kinetics of peritoneal adhesion formation in the rat and evaluation of potential antiadhesive agents. Surgery 117: 663–669. doi: 10.1016/S0039-6060(95)80010-7
|
| [60] | Risberg B (1997) Adhesions: preventive strategies. Eur J Surg 577: 32–39. |
| [61] |
Tsai SW, Fang JF, Yang CL, et al. (2005) Preparation and evaluation of a hyaluronate-collagen film for preventing post-surgical adhesion. Int Med Res 33: 68–76. doi: 10.1177/147323000503300106
|
| [62] | Park SN, Jang HJ, Choi YS, et al. (2007) Preparation and characterization of biodegradable anti-adhesive membrane for peritoneal wound healing. J Mater Sci-Mater M 18: 475–482. |
| [63] |
Temiz A, Ozturk C, Bakunov A, et al. (2008) A new material for prevention of peritendinous fibrotic adhesions after tendon repair: oxidized regenerated cellulose (Interceed), an absorbable adheison barrier. Int Orthop 32: 389–394. doi: 10.1007/s00264-007-0335-8
|
| [64] |
Liu Y, Skardal A, Shu XZ, et al. (2008) Prevention of peritendinous adhesions using a hyaluronan-derived hydrogel film following partial-thickness flexor tendon injury. J Orthop Res 26: 562–569. doi: 10.1002/jor.20499
|
| [65] |
Rajab TK, Wallwiener M, Talukdar S, et al. (2009) Adhesion-related complications are common, but rarely discussed in preoperative consent; a multicenter study. World J Surg 33: 748–750. doi: 10.1007/s00268-008-9917-x
|
| [66] |
Cheung J, Tsang H, Cheung J, et al. (2009) Adjuvant therapy for the reduction of postoperative intra-abdominal adhesion formation. Asian J Surg 32: 180–186. doi: 10.1016/S1015-9584(09)60392-4
|
| [67] | Brochhausen C, Schmitt V, Rajab T, et al. (2011) Intraperitoneal adhesions-an ongoing challenge betwenn biomedical engineering and the life sciences. J Biomed Mater Res A 98: 143–156. |
| [68] |
Kuroyanagi M, Yamamoto A, Shimizu N, et al. (2014) Development of anti-adhesive spongy sheet composed of hyaluronic acid and collagen containing epidermal growth factor. J Biomat Sci-Polym E 25: 1253–1265. doi: 10.1080/09205063.2014.926579
|

Figures(14) / Tables(1)

Misato Kuroyanagi, Yoshimitsu Kuroyanagi. Tissue-engineered products capable of enhancing wound healing[J]. AIMS Materials Science, 2017, 4(3): 561-581. doi: 10.3934/matersci.2017.3.561







 DownLoad:
DownLoad: