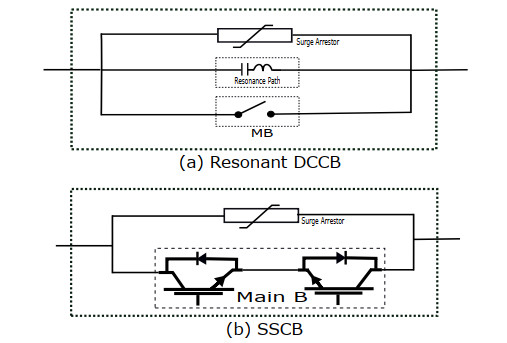
DC system has the potential of vast and rapid fault current generation due to multiple (line and converters) discharge capacitors and small impedance of DC lines. DC fault current spreads through the system exponentially compared to AC. Such an unexpected huge current causes a voltage drop, impacts the normal operation of system components and exposes the system to a great challenge for fault detection and interruption. For prevention of system destruction during the fault, multiple approaches such as application of Mechanical Circuit Breakers (MCBs), fuses, Solid State Circuit Breaker (SSCB), and Hybrid Solid-State Circuit Breaker (HSSCB) have been proposed and applied. In DC fault applications, fast fault detection and interruption without any interference to the other components are quite important. Therefore, semiconductor breakers have been implemented to meet the DC fault protection requirements with a high-speed operation where traditional MBs have failed. Due to the high conduction loss and low efficiency of semiconductor switches, for fast and efficient DC fault interruption, different Fault Current Limiter (FCL) types are suggested. Although a high impedance FCL can prevent the voltage fluctuations due to the current decline, it can cause operation speed issues, coordination troubles, overheat, and malfunction of protective components in a fault situation.
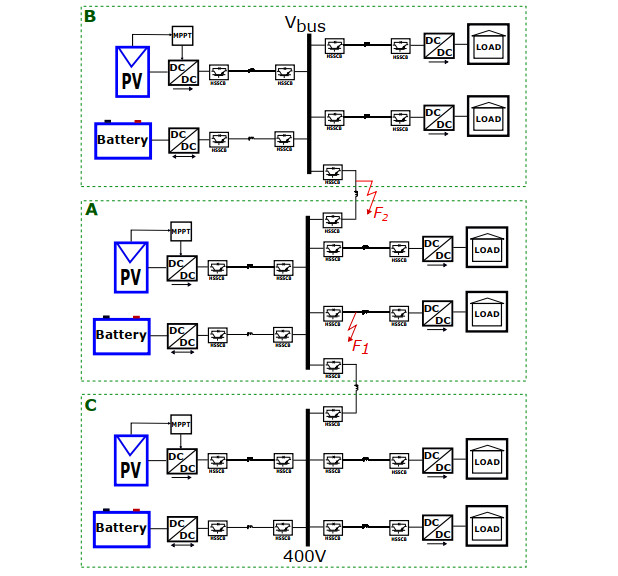
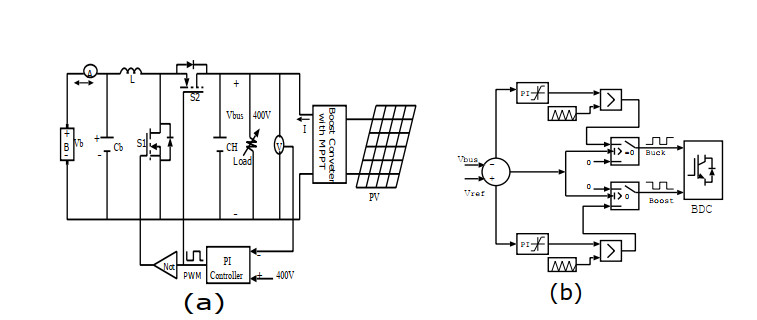
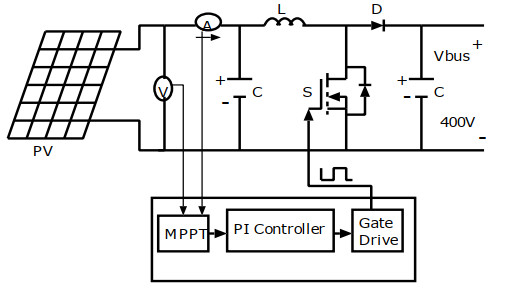
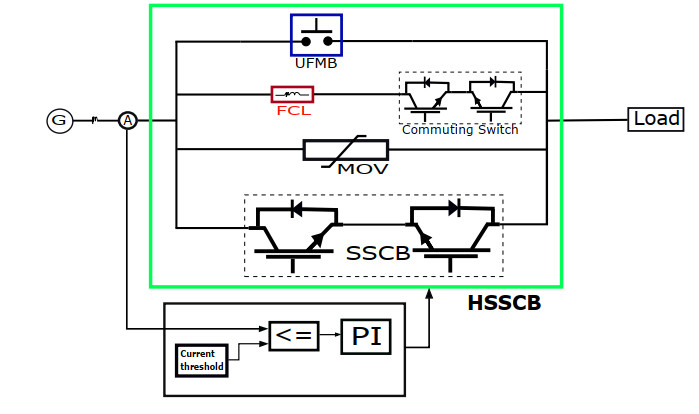
This paper focused on a combination of two-way HSSCB with a self-adapt DC short current limiter, ultra-fast switch, and power electronic switch to overcome the above challenges. It can efficiently and fast fault current limiting response with low conducting loss and appropriate cooperation among protective components in a low voltage DC system. The MATLAB/Simulink is used to analyze the effectiveness and consistency of the proposed FCL-HSSCB in 400 V interconnected standalone DC microgrids.
Citation: Mohammad Aman YAQOBI, Hidehito Matayoshi, Natarajan Prabaharan, Hiroshi Takahashi, Ashraf M. Hemeida, Senjyu Tomonobu. Interconnected standalone DC microgrid fault protection based on Self-Adaptive DC fault current limiter with hybrid solid state circuit breaker[J]. AIMS Energy, 2021, 9(5): 991-1008. doi: 10.3934/energy.2021045
DC system has the potential of vast and rapid fault current generation due to multiple (line and converters) discharge capacitors and small impedance of DC lines. DC fault current spreads through the system exponentially compared to AC. Such an unexpected huge current causes a voltage drop, impacts the normal operation of system components and exposes the system to a great challenge for fault detection and interruption. For prevention of system destruction during the fault, multiple approaches such as application of Mechanical Circuit Breakers (MCBs), fuses, Solid State Circuit Breaker (SSCB), and Hybrid Solid-State Circuit Breaker (HSSCB) have been proposed and applied. In DC fault applications, fast fault detection and interruption without any interference to the other components are quite important. Therefore, semiconductor breakers have been implemented to meet the DC fault protection requirements with a high-speed operation where traditional MBs have failed. Due to the high conduction loss and low efficiency of semiconductor switches, for fast and efficient DC fault interruption, different Fault Current Limiter (FCL) types are suggested. Although a high impedance FCL can prevent the voltage fluctuations due to the current decline, it can cause operation speed issues, coordination troubles, overheat, and malfunction of protective components in a fault situation.
This paper focused on a combination of two-way HSSCB with a self-adapt DC short current limiter, ultra-fast switch, and power electronic switch to overcome the above challenges. It can efficiently and fast fault current limiting response with low conducting loss and appropriate cooperation among protective components in a low voltage DC system. The MATLAB/Simulink is used to analyze the effectiveness and consistency of the proposed FCL-HSSCB in 400 V interconnected standalone DC microgrids.

| [1] |
Oh YS, Han J, Gwon G-H, et al. (2016) Detection of high-impedance fault in low-voltage DC distribution system via mathematical morphology. J Int Counc Electr Eng 6: 194-201. doi: 10.1080/22348972.2016.1228493

|
| [2] |
Yang J, Fletcher JE, O'Reilly J (2012) Short-circuit and ground fault analyses and location in VSC-based DC network cables. IEEE Trans Ind Electron 59: 3827-3837. doi: 10.1109/TIE.2011.2162712
|
| [3] |
Satpathi K, Ukil A, Pou J (2018) Short-Circuit fault management in DC electric ship propulsion system: Protection requirements, review of existing technologies and future research trends. IEEE Trans Trans Electrif 4: 272-291. doi: 10.1109/TTE.2017.2788199
|
| [4] |
Kim S, Kim SN, Dujic D (2020) Extending protection selectivity in DC shipboard power systems by means of additional bus capacitance. IEEE Trans Ind Electron Control Instrum 67: 3673-3683. doi: 10.1109/TIE.2019.2916371
|
| [5] | Liu K, Yang X, Li Y, et al. (2018) Study of protection for serial multi-terminal DC grids. J Int Counc Electr Eng 8: 70-78. |
| [6] |
Lacerda VA, Monaro RM, Peña-Alzola R, et al. (2020) Control-based fault current limiter for modular multilevel voltage-source converters. Int J Electr Power Energy Syst 118: 105-150. doi: 10.1016/j.ijepes.2019.105750
|
| [7] | Lee KH (2009) Prospect of DC distribution systems and safety issues. J Korean Institute Power Electron 14: 21-28. |
| [8] |
Fletcher SDA, Norman PJ, Fong K, et al. (2014) High-Speed differential protection for smart DC distribution systems. IEEE Trans Smart Grid 5: 2610-2617. doi: 10.1109/TSG.2014.2306064
|
| [9] |
Miao H, Sabui G, Roshandeh AM, et al. (2016) Design and analysis of DC Solid-State circuit breakers using SiC JFETs. IEEE Emerging Sel Top Power Electron 4: 863-873. doi: 10.1109/JESTPE.2016.2558448
|
| [10] |
Salomonsson D, Sannino A (2007) Low-Voltage DC distribution system for commercial power systems with sensitive electronic loads. IEEE Trans Power Delivery 22: 1620-1627. doi: 10.1109/TPWRD.2006.883024
|
| [11] | Liu YC, Chang EC, Lin YL, et al. (2018) A Novel online insulation fault detection circuit for DC power supply systems. Int J Smart Grid Clean Energy 7: 194-201. |
| [12] | Li LQ, Antonello A, Luca R (2017) Detection of high-impedance fault in low-voltage DC distribution system via mathematical morphology. Design of solid-state circuit breaker-based protection for DC shipboard power systems 5: 260-268. |
| [13] | Salato M, Zolj A, Becker D-J, et al. (2012) Power system architectures for 380 V dc distribution in telecom datacenters. Proc IEEE Int 23: 23-46. |
| [14] |
Liu F, Liu W-J, Zha X-M, et al. (2017) Solid-state circuit breaker snubber design for transient overvoltage suppression at bus fault interruption in low-voltage dc microgrid. IEEE Trans Power Electron 32: 3007-3021. doi: 10.1109/TPEL.2016.2574751
|
| [15] | Rashad M, Raoof U, Ashraf M, et al. (2018) Proportional load sharing and stability of DC microgrid with distributed architecture using SM controller. Math Probl Eng 3: 271-279. |
| [16] |
Shuai Z, He N, Xiong Z, et al. (2018) Comparative study of Short-Circuit fault characteristics for VSC-Based DC distribution networks with different distributed generators. IEEE J Emerging Sel Top Power Electron 7: 528-540. doi: 10.1109/JESTPE.2018.2834542
|
| [17] | Jae S-H, Khan UA, Shin W-J, et al. (2016) Validity analysis on the positioning of superconducting fault current limiter in neighboring AC and DC microgrid. IEEE Trans Appl Supercond 23: 204-256. |
| [18] |
Jovcic D, Zhang L, Hajian M (2013) LCL VSC converter for high-power applications. IEEE Trans Power Delivery 28: 137-144. doi: 10.1109/TPWRD.2012.2219560
|
| [19] | Nasereddine R, Amor I, Massoud A, et al. (2013) AC solid state circuit breakers for fault current limitation in distributed generation. IEEE GCC Conference and Exhibition (GCC) 7: 446-449. |
| [20] |
Janowski T, Glowacki BA, Wojtasiewicz G, et al. (2011) Fault current limitation in power network by the superconducting transformers made of 2G HTS. IEEE Trans Appl Supercond 21: 1413-1416. doi: 10.1109/TASC.2011.2112325
|
| [21] | Chen L (2019) Application and design of a resistive-type superconducting fault current limiter for efficient protection of a DC microgrid. IEEE Trans Appl Supercond 29: 56-67. |
| [22] | Nair1 AA, Krishna KT (2016) Micogrid protection using superconducting fault current limiter. Int Res J Eng Technol (IRJET) 3: 72-95. |
| [23] |
Xue S, Gao F, Sun W, et al. (2015) Protection principle for a DC distribution system with a resistive superconductive fault current limiter. Energies 8: 4839-4852. doi: 10.3390/en8064839
|
| [24] | Khan UA, Lee JG, Amir F, et al. (2015)A novel model of HVDC hybrid-type superconducting circuit breaker and its performance analysis for limiting and breaking dc fault currents. IEEE Trans Appl Supercond 25: 560-3009. |
| [25] | Xiaomin Q (2019) Analysis on characteristic of DC short-circuit fault in multi-terminal AC/DC hybrid distribution network. J Eng 16: 2051-3305. |
| [26] | Chaudhuri NR, Chaudhuri B, Majumder R, et al. (2014) Modeling, analysis, and simulation of AC–MTDC grids, in Multi-Terminal DC grids: Modeling, analysis, and control. John Wiley and Sons, Inc 33: 231-235. |
| [27] |
Nag SS, Mishra S, Joshi S (2016) A passive filter building block for input or output current ripple cancellation in a power converter. IEEE J Emerging Sel Top Power Electron 4: 564-575. doi: 10.1109/JESTPE.2015.2496146
|
| [28] |
Yeap YM, Geddada N, Ukil A (2017) Capacitive discharge based transient analysis with fault detection methodology in DC system. Int J Electr Porwer Energy Syst 97: 127-137. doi: 10.1016/j.ijepes.2017.10.023
|
| [29] | Zhang J, Gao Y, Xiao F, et al. (2019) Study on DC breaker fault current and its limiting method of multiterminal flexible DC distribution system. MDPI 12: 840-859. |
| [30] |
Huaren W, Ling Y, Lin S, et al. (2015) Modeling of Current-Limiting circuit breakers for the calculation of Short-Circuit current. Power Del, IEEE Trans 30: 652-656. doi: 10.1109/TPWRD.2014.2305166
|
| [31] |
Li B, He J, Li Y, et al. (2019) A novel Solid-State circuit breaker with Self-Adapt fault current limiting capability for LVDC distribution network. IEEE Trans Power Electron 34: 3516-3529. doi: 10.1109/TPEL.2018.2850441
|
| [32] |
Li H, Yu R, Zhong Y, et al. (2019) Design of 400 V miniature DC solid state circuit breaker with SiC MOSFET. Micromachines 10: 314. doi: 10.3390/mi10050314
|
| [33] |
Yaqobi AM, Matayoshi H, Danish MSS, et al. (2019) Low-Voltage Solid-State DC breaker for fault protection applications in isolated DC microgrid cluster. Appl Sci 9: 723. doi: 10.3390/app9040723
|
| [34] | May-Ostendorp P, Porter SF, Denkenberger D, et al. (2014) Reviving the war of currents: Opportunities to save energy with DC distribution in commercial buildings. ECOVA 72: 342-365. |
| [35] |
Sano K, Takasaki M (2014) Review of DC power distribution in buildings: A technology and market assessment. IEEE Trans Ind Appl 50: 2690-2699. doi: 10.1109/TIA.2013.2293819
|
| [36] | Andersson D, Henriksson A (2011) Passive and active DC breakers in the three gorges changahou hvdc project. International Conference on Power System, Wuhan, China: CIGRE: 391-395. |
| [37] | Mitra B, Chowdhury B (2017) Comparative analysis of hybrid DC breaker and assembly HVDC breaker. IEEE Xplore. |
| [38] |
Planas E, Andreu J, Gárate JI, et al. (2015) AC and DC technology in microgrids: A review. Renewable Sustainable Energy Rev 43: 726-749. doi: 10.1016/j.rser.2014.11.067
|
| [39] |
Alam MS, Abido MAY, El-Amin I (2018) Fault current limiters in power systems: A comprehensive review. MDPI Energies 11: 1025. doi: 10.3390/en11051025
|
Figures(15) / Tables(2)

Mohammad Aman YAQOBI, Hidehito Matayoshi, Natarajan Prabaharan, Hiroshi Takahashi, Ashraf M. Hemeida, Senjyu Tomonobu. Interconnected standalone DC microgrid fault protection based on Self-Adaptive DC fault current limiter with hybrid solid state circuit breaker[J]. AIMS Energy, 2021, 9(5): 991-1008. doi: 10.3934/energy.2021045







 DownLoad:
DownLoad: