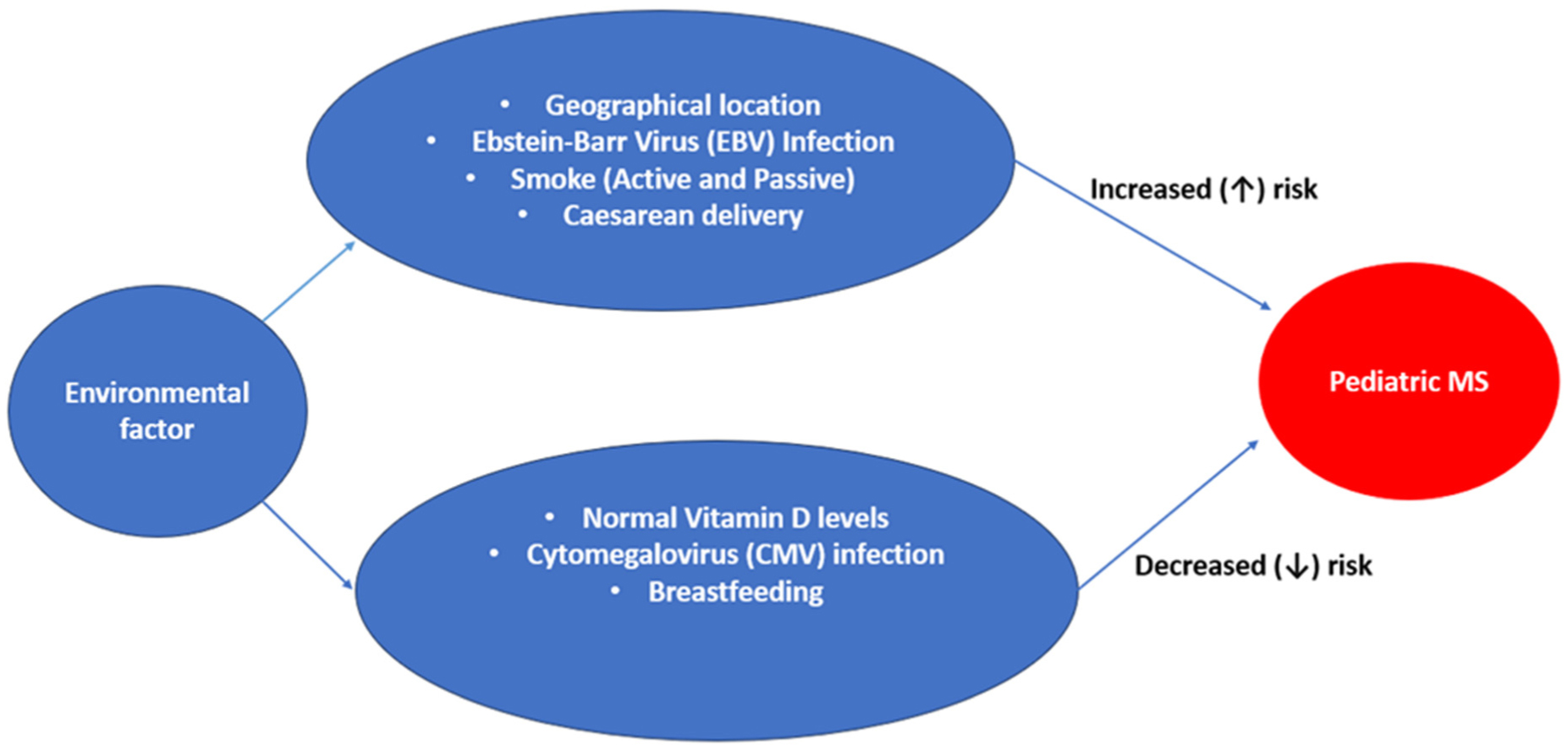
Multiple sclerosis (MS) is a debilitating autoimmune condition caused by demyelination, neurodegeneration and persistent inflammation of the central nervous system. Pediatric multiple sclerosis (PMS) is a relatively rare form of the disease that affects a significant number of individuals with MS. Environmental exposures, such as viral infections and smoking, can interact with MS-associated human leukocyte antigens (HLA) risk alleles and influence the immune response. Upregulation of immune response results in the disruption of immune balance leading to cascade of inflammatory events. It has also been established that gut microbiome dysbiosis poses a higher risk for pro-inflammation, and it is essentially argued to be the greatest environmental risk factor for MS. Dysbiosis can cause an unusual response from the adaptive immune system and significantly contribute to the development of disease in the host by activating pro-inflammatory pathways that cause immune-mediated disorders such as PMS, rendering the body more vulnerable to foreign attacks due to a weakened immune response. All these dynamic interactions between biological, environmental and genetic factors based on epigenetic study has further revealed that upregulation or downregulation of some genes/enzyme in the central nervous system white matter of MS patients produces a less stable form of myelin basic protein and ultimately leads to the loss of immune tolerance. The diagnostic criteria and treatment options for PMS are constantly evolving, making it crucial to have a better understanding of the disease burden on a global and regional scale. The findings from this review will aid in deepening the understanding of the interplay between genetic and environmental risk factors, as well as the role of the gut microbiome in the development of pediatric multiple sclerosis. As a result, healthcare professionals will be kept abreast of the early diagnostic criteria, accurately delineating other conditions that can mimic pediatric MS and to provide comprehensive care to individuals with PMS based on the knowledge gained from this research.
Citation: Uzochukwu Adabanya, Ayoola Awosika, Anosh Khan, Ejike Oluka, Mayowa Adeniyi. Pediatric multiple sclerosis: an integrated outlook at the interplay between genetics, environment and brain-gut dysbiosis[J]. AIMS Neuroscience, 2023, 10(3): 232-251. doi: 10.3934/Neuroscience.2023018
Multiple sclerosis (MS) is a debilitating autoimmune condition caused by demyelination, neurodegeneration and persistent inflammation of the central nervous system. Pediatric multiple sclerosis (PMS) is a relatively rare form of the disease that affects a significant number of individuals with MS. Environmental exposures, such as viral infections and smoking, can interact with MS-associated human leukocyte antigens (HLA) risk alleles and influence the immune response. Upregulation of immune response results in the disruption of immune balance leading to cascade of inflammatory events. It has also been established that gut microbiome dysbiosis poses a higher risk for pro-inflammation, and it is essentially argued to be the greatest environmental risk factor for MS. Dysbiosis can cause an unusual response from the adaptive immune system and significantly contribute to the development of disease in the host by activating pro-inflammatory pathways that cause immune-mediated disorders such as PMS, rendering the body more vulnerable to foreign attacks due to a weakened immune response. All these dynamic interactions between biological, environmental and genetic factors based on epigenetic study has further revealed that upregulation or downregulation of some genes/enzyme in the central nervous system white matter of MS patients produces a less stable form of myelin basic protein and ultimately leads to the loss of immune tolerance. The diagnostic criteria and treatment options for PMS are constantly evolving, making it crucial to have a better understanding of the disease burden on a global and regional scale. The findings from this review will aid in deepening the understanding of the interplay between genetic and environmental risk factors, as well as the role of the gut microbiome in the development of pediatric multiple sclerosis. As a result, healthcare professionals will be kept abreast of the early diagnostic criteria, accurately delineating other conditions that can mimic pediatric MS and to provide comprehensive care to individuals with PMS based on the knowledge gained from this research.

| [1] |
Faissner S, Plemel JR, Gold R, et al. (2019) Progressive multiple sclerosis: from pathophysiology to therapeutic strategies. Nat Rev Drug Discov 18: 905-922. https://doi.org/10.1038/s41573-019-0035-2 
|
| [2] |
Alroughani R, Boyko A (2018) Pediatric multiple sclerosis: a review. BMC Neurol 9: 18: 27. https://doi.org/10.1186/s12883-018-1026-3
|
| [3] | Pena JA, Lotze TE (2013) Pediatric multiple sclerosis: current concepts and consensus definitions. Autoimmune Dis 2013: 673947. https://doi.org/10.1155/2013/673947 |
| [4] |
Pavithra CU, Swetha K, Romauld SI, et al. (2020) A review on multiple sclerosis and its regimens. Res J Pharmacy Technol 13: 3977-3982. https://doi.org/10.5958/0974-360X.2020.00703.9
|
| [5] |
Jancic J, Nikolic B, Ivancevic N, et al. (2016) Multiple Sclerosis in Pediatrics: Current Concepts and Treatment Options. Neurol Ther 5: 131-143. https://doi.org/10.1007/s40120-016-0052-6
|
| [6] |
Vitturi BK, Rahmani A, Dini G, et al. (2022) Occupational outcomes of people with multiple sclerosis: a scoping review. BMJ Open 12: e058948. https://doi.org/10.1136/bmjopen-2021-058948
|
| [7] |
Abdulsalam AJ, Özçakar L (2020) Multiple sclerosis: renaming the notorious and historical diagnosis?. Neurol Sci 41: 2283-2284. https://doi.org/10.1007/s10072-020-04291-y
|
| [8] | Friedman M (2020) There's No Pill for This: A Naturopathic Physician's Personal Prescription for Managing Multiple Sclerosis. Chelsea Green Publishing. |
| [9] |
Redfern JS (2021) Immunopathophysiologic basis of multiple sclerosis and implications for therapy-a narrative review. Pharm Pharmacol Int J 9: 263-271. https://doi.org/10.15406/ppij.2021.09.00355
|
| [10] |
Tauil CB, VON Glehn F, Nonato-Rodrigues R, et al. (2019) From Charcot's descriptions to the current understanding of neuropsychiatric symptoms in multiple sclerosis. Arq Neuropsiquiatr 77: 521-524. https://doi.org/10.1590/0004-282x20190049
|
| [11] |
Segal BM (2014) Stage-specific immune dysregulation in multiple sclerosis. J Interferon Cytokine Res 34: 633-640. https://doi.org/10.1089/jir.2014.0025
|
| [12] |
Kamel FO (2019) Factors Involved in Relapse of Multiple Sclerosis. J Microsc Ultrastruct 7: 103-108. https://doi.org/10.4103/JMAU.JMAU_59_18
|
| [13] |
Daltrozzo T, Hapfelmeier A, Donnachie E, et al. (2018) A Systematic Assessment of Prevalence, Incidence and Regional Distribution of Multiple Sclerosis in Bavaria From 2006 to 2015. Front Neurol 9: 871. https://doi.org/10.3389/fneur.2018.00871
|
| [14] |
Yan K, Balijepalli C, Desai K, et al. (2020) Epidemiology of pediatric multiple sclerosis: A systematic literature review and meta-analysis. Mult Scler Relat Disord 44: 102260. https://doi.org/10.1016/j.msard.2020.102260
|
| [15] |
Wang Y, Kasper LH (2014) The role of microbiome in central nervous system disorders. Brain Behav Immun 38: 1-12. https://doi.org/10.1016/j.bbi.2013.12.015
|
| [16] |
Koutmos M, Kabil O, Smith JL, et al. (2010) Structural basis for substrate activation and regulation by cystathionine beta-synthase (CBS) domains in cystathionine {beta}-synthase. Proc Natl Acad Sci U S A 107: 20958-63. https://doi.org/10.1073/pnas.1011448107
|
| [17] |
Maslowski KM, Mackay CR (2011) Diet, gut microbiota and immune responses. Nat Immunol 12: 5-9. https://doi.org/10.1038/ni0111-5
|
| [18] |
Bäckhed F, Ley RE, Sonnenburg JL, et al. (2005) Host-bacterial mutualism in the human intestine. Science 307: 1915-20. https://doi.org/10.1126/science.1104816
|
| [19] |
Lee YK, Mazmanian SK (2010) Has the microbiota played a critical role in the evolution of the adaptive immune system?. Science 330: 1768-73. https://doi.org/10.1126/science.1195568
|
| [20] |
Harmsen HJ, de Goffau MC (2016) The Human Gut Microbiota. Adv Exp Med Biol 902: 95-108. https://doi.org/10.1007/978-3-319-31248-4_7
|
| [21] |
Eckburg PB, Bik EM, Bernstein CN, et al. (2005) Diversity of the human intestinal microbial flora. Science 308: 1635-8. https://doi.org/10.1126/science.1110591
|
| [22] |
Ghoshal UC, Ghoshal U (2017) Small Intestinal Bacterial Overgrowth and Other Intestinal Disorders. Gastroenterol Clin North Am 46: 103-120. https://doi.org/10.1016/j.gtc.2016.09.008
|
| [23] |
Cebra JJ (1999) Influences of microbiota on intestinal immune system development. Am J Clin Nutr 69: 1046S-1051S. https://doi.org/10.1093/ajcn/69.5.1046s
|
| [24] |
Round JL, Mazmanian SK (2009) The gut microbiota shapes intestinal immune responses during health and disease. Nat Rev Immunol 9: 313-23. https://doi.org/10.1038/nri2515
|
| [25] |
Thaiss CA, Itav S, Rothschild D, et al. (2016) Persistent microbiome alterations modulate the rate of post-dieting weight regain. Nature 540: 544-551. https://doi.org/10.1038/nature20796
|
| [26] |
Bandeira A, Mota-Santos T, Itohara S, et al. (1990) Localization of gamma/delta T cells to the intestinal epithelium is independent of normal microbial colonization. J Exp Med 172: 239-44. https://doi.org/10.1084/jem.172.1.239
|
| [27] |
Crabbé PA, Bazin H, Eyssen H, et al. (1968) The normal microbial flora as a major stimulus for proliferation of plasma cells synthesizing IgA in the gut. The germ-free intestinal tract. Int Arch Allergy Appl Immunol 34: 362-75. https://doi.org/10.1159/000230130
|
| [28] |
Atarashi K, Tanoue T, Oshima K, et al. (2013) Treg induction by a rationally selected mixture of Clostridia strains from the human microbiota. Nature 500: 232-6. https://doi.org/10.1038/nature12331
|
| [29] |
Arpaia N, Campbell C, Fan X, et al. (2013) Metabolites produced by commensal bacteria promote peripheral regulatory T-cell generation. Nature 504: 451-5. https://doi.org/10.1038/nature12726
|
| [30] |
Toor D, Wsson MK, Kumar P, et al. (2019) Dysbiosis Disrupts Gut Immune Homeostasis and Promotes Gastric Diseases. Int J Mol Sci 20: 2432. https://doi.org/10.3390/ijms20102432
|
| [31] |
Ghoshal UC, Srivastava D (2014) Irritable bowel syndrome and small intestinal bacterial overgrowth: meaningful association or unnecessary hype. World J Gastroenterol 20: 2482-91. https://doi.org/10.3748/wjg.v20.i10.2482
|
| [32] |
Trott S, King IL (2018) An introduction to the microbiome and MS. Mult Scler 24: 53-57. https://doi.org/10.1177/1352458517737391
|
| [33] |
Romijn JA, Corssmit EP, Havekes LM, et al. (2008) Gut-brain axis. Curr Opin Clin Nutr Metab Care 11: 518-21. https://doi.org/10.1097/MCO.0b013e328302c9b0
|
| [34] | Chu F, Shi M, Lang Y, et al. (2018) Gut Microbiota in Multiple Sclerosis and Experimental Autoimmune Encephalomyelitis: Current Applications and Future Perspectives. Mediators Inflamm 2018: 8168717. https://doi.org/10.1155/2018/8168717 |
| [35] |
Mayer EA, Tillisch K, Gupta A (2015) Gut/brain axis and the microbiota. J Clin Invest 125: 926-38. https://doi.org/10.1172/JCI76304
|
| [36] |
Adamczyk-Sowa M, Medrek A, Madej P, et al. (2017) Does the Gut Microbiota Influence Immunity and Inflammation in Multiple Sclerosis Pathophysiology?. J Immunol Res 2017: 7904821. https://doi.org/10.1155/2017/7904821
|
| [37] |
Joscelyn J, Kasper LH (2014) Digesting the emerging role for the gut microbiome in central nervous system demyelination. Mult Scler 20: 1553-9. https://doi.org/10.1177/1352458514541579
|
| [38] | Mazmanian SK A microbial system promotes stable colonization by bacteroides of the gut microbiota (2013). In: The Gut Microbiome: The Effector/Regulatory Immune Network ed.^eds., pp. February 10–15, 2013. Keystone Symposia on Molecular and Cellular Biology, Sagebrush Inn & Suites Taos, New Mexico USA |
| [39] |
Tremlett H, Fadrosh DW, Faruqi AA, et al. (2016) US Network of Pediatric MS Centers. Gut microbiota in early pediatric multiple sclerosis: a case-control study. Eur J Neurol 23: 1308-1321. https://doi.org/10.1111/ene.13026
|
| [40] |
Nagalingam NA, Lynch SV (2012) Role of the microbiota in inflammatory bowel diseases. Inflamm Bowel Dis 18: 968-84. https://doi.org/10.1002/ibd.21866
|
| [41] |
Cappa R, Theroux L, Brenton JN (2017) Pediatric Multiple Sclerosis: Genes, Environment, and a Comprehensive Therapeutic Approach. Pediatr Neurol 75: 17-28. https://doi.org/10.1016/j.pediatrneurol.2017.07.005
|
| [42] |
Simpson S, Blizzard L, Otahal P, et al. (2011) Latitude is significantly associated with the prevalence of multiple sclerosis: a meta-analysis. J Neurol Neurosurg Psychiatry 82: 1132-41. https://doi.org/10.1136/jnnp.2011.240432
|
| [43] |
Gale CR, Martyn CN (1995) Migrant studies in multiple sclerosis. Prog Neurobiol 7: 425-48. https://doi.org/10.1016/0301-0082(95)80008-V
|
| [44] |
Van der Mei IA, Ponsonby AL, Blizzard L, et al. (2001) Regional variation in multiple sclerosis prevalence in Australia and its association with ambient ultraviolet radiation. Neuroepidemiology 20: 168-74. https://doi.org/10.1159/000054783
|
| [45] |
Larsen PD, Bloomer LC, Bray PF (1985) Epstein-Barr nuclear antigen and viral capsid antigen antibody titers in multiple sclerosis. Neurology 35: 435-8. https://doi.org/10.1212/WNL.35.3.435
|
| [46] |
Waubant E, Mowry EM, Krupp L, et al. (2011) US Pediatric MS Network. Common viruses associated with lower pediatric multiple sclerosis risk. Neurology 76: 1989-95. https://doi.org/10.1212/WNL.0b013e31821e552a
|
| [47] |
Mikaeloff Y, Caridade G, Tardieu M, et al. (2007) KIDSEP study group. Parental smoking at home and the risk of childhood-onset multiple sclerosis in children. Brain 130: 2589-95. https://doi.org/10.1093/brain/awm198
|
| [48] |
Nielsen NM, Bager P, Stenager E, et al. (2013) Cesarean section and offspring's risk of multiple sclerosis: a Danish nationwide cohort study. Mult Scler 19: 1473-7. https://doi.org/10.1177/1352458513480010
|
| [49] | Brenton J, Goldman M Prolonged breastfeeding as an infant reduces future risk of pediatric onset multiple sclerosis: A Case-Control Study (P1.377). Neurology (2016)86: P1.377. |
| [50] |
Disanto G, Magalhaes S, Handel AE, et al. (2011) Canadian Pediatric Demyelinating Disease Network. HLA-DRB1 confers increased risk of pediatric-onset MS in children with acquired demyelination. Neurology 76: 781-6. https://doi.org/10.1212/WNL.0b013e31820ee1cd
|
| [51] |
Banwell B, Bar-Or A, Arnold DL, et al. (2011) Clinical, environmental, and genetic determinants of multiple sclerosis in children with acute demyelination: a prospective national cohort study. Lancet Neurol 10: 436-45. https://doi.org/10.1016/S1474-4422(11)70045-X
|
| [52] | Barcellos L, Shao X, Rhead B, et al. (2016) First genome-wide analysis in pediatric multiple sclerosis (MS) confirms a role for adult MS risk variants and reveals new candidates (S29.001). Neurology 86. |
| [53] |
Venkateswaran S, Zheng K, Sacchetti M, et al. (2011) Canadian Pediatric Demyelinating Disease Network. Mitochondrial DNA haplogroups and mutations in children with acquired central demyelination. Neurology 76: 774-80. https://doi.org/10.1212/WNL.0b013e31820ee1bb
|
| [54] |
Mastronardi FG, Noor A, Wood DD, et al. (2007) Peptidyl argininedeiminase 2 CpG island in multiple sclerosis white matter is hypomethylated. J Neurosci Res 85: 2006-16. https://doi.org/10.1002/jnr.21329
|
| [55] |
Janson PC, Linton LB, Bergman EA, et al. (2011) Profiling of CD4+ T cells with epigenetic immune lineage analysis. J Immunol 186: 92-102. https://doi.org/10.4049/jimmunol.1000960
|
| [56] |
Kumagai C, Kalman B, Middleton FA, et al. (2012) Increased promoter methylation of the immune regulatory gene SHP-1 in leukocytes of multiple sclerosis subjects. J Neuroimmunol 246: 51-7. https://doi.org/10.1016/j.jneuroim.2012.03.003
|
| [57] |
Hedström AK, Lima Bomfim I, Barcellos L, et al. (2014) Interaction between adolescent obesity and HLA risk genes in the etiology of multiple sclerosis. Neurology 82: 865-72. https://doi.org/10.1212/WNL.0000000000000203
|
| [58] | An Q, Fan CH, Xu SM (2018) Childhood multiple sclerosis: clinical features and recent developments on treatment choices and outcomes. Eur Rev Med Pharmacol Sci 22: 5747-5754. |
| [59] |
Duignan S, Brownlee W, Wassmer E, et al. (2019) Pediatric multiple sclerosis: a new era in diagnosis and treatment. Dev Med Child Neurol 61: 1039-1049. https://doi.org/10.1111/dmcn.14212
|
| [60] |
Gorman MP, Healy BC, Polgar-Turcsanyi M, et al. (2009) Increased relapse rate in pediatric-onset compared with adult-onset multiple sclerosis. Arch Neurol 66: 54-9. https://doi.org/10.1001/archneurol.2008.505
|
| [61] |
Chitnis T, Krupp L, Yeh A, et al. (2011) Pediatric multiple sclerosis. Neurol Clin 29: 481-505. https://doi.org/10.1016/j.ncl.2011.01.004
|
| [62] |
Brola W, Steinborn B (2020) Pediatric multiple sclerosis - current status of epidemiology, diagnosis and treatment. Neurol Neurochir Pol 54: 508-517. https://doi.org/10.5603/PJNNS.a2020.0069
|
| [63] |
Wang CX, Greenberg BM (2018) Pediatric Multiple Sclerosis: From Recognition to Practical Clinical Management. Neurol Clin 36: 135-149. https://doi.org/10.1016/j.ncl.2017.08.005
|
| [64] |
Krupp LB, Tardieu M, Amato MP, et al. (2013) International Pediatric Multiple Sclerosis Study Group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders: revisions to the 2007 definitions. Mult Scler 19: 1261-7. https://doi.org/10.1177/1352458513484547
|
| [65] |
Otallah S, Banwell B (2018) Pediatric Multiple Sclerosis: an Update. Curr Neurol Neurosci Rep 18: 76. https://doi.org/10.1007/s11910-018-0886-7
|
| [66] |
Rostasy K, Bajer-Kornek B, Venkateswaran S, et al. (2016) Differential diagnosis and evaluation in pediatric inflammatory demyelinating disorders. Neurology 87: S28-S37. https://doi.org/10.1212/WNL.0000000000002878
|
| [67] | Galardi MM, Gaudioso C, Ahmadi S, et al. (2019) Differential Diagnosis of Pediatric Multiple Sclerosis. Children 75. https://doi.org/10.3390/children6060075 |
| [68] |
Wynford-Thomas R, Jacob A, Tomassini V (2019) Neurological update: MOG antibody disease. J Neurol 266: 1280-1286. https://doi.org/10.1007/s00415-018-9122-2
|
| [69] |
Ketelslegers IA, Van Pelt DE, Bryde S, et al. (2015) Anti-MOG antibodies plead against MS diagnosis in an acquired demyelinating syndromes cohort. Mult Scler J 21: 1513-20. https://doi.org/10.1177/1352458514566666
|
| [70] |
Tenembaum SN, Banwell B, Pohl D, et al. (2013) Subcutaneous interferon beta-1a in pediatric multiple sclerosis: A retrospective study. J Child Neurol 28: 849-856. https://doi.org/10.1177/0883073813488828
|
| [71] |
Montalban X, Hauser SL, Kappos L, et al. (2017) Ocrelizumab versus placebo in primary progressive multiple sclerosis. New Engl J Med 376: 209-220. https://doi.org/10.1056/NEJMoa1606468
|
| [72] |
Huppke P, Huppke B, Ellenberger D, et al. (2019) Therapy of highly active pediatric multiple sclerosis. Mult Scler J 25: 72-80. https://doi.org/10.1177/1352458517732843
|
| [73] |
Reynolds ER, Ashbaugh AD, Hockenberry BJ, et al. (2018) Multiple Sclerosis and Exercise: A Literature Review. Curr Sports Med Rep 17: 31-35. https://doi.org/10.1249/JSR.0000000000000446
|
Figures(1) / Tables(4)

Uzochukwu Adabanya, Ayoola Awosika, Anosh Khan, Ejike Oluka, Mayowa Adeniyi. Pediatric multiple sclerosis: an integrated outlook at the interplay between genetics, environment and brain-gut dysbiosis[J]. AIMS Neuroscience, 2023, 10(3): 232-251. doi: 10.3934/Neuroscience.2023018







 DownLoad:
DownLoad: