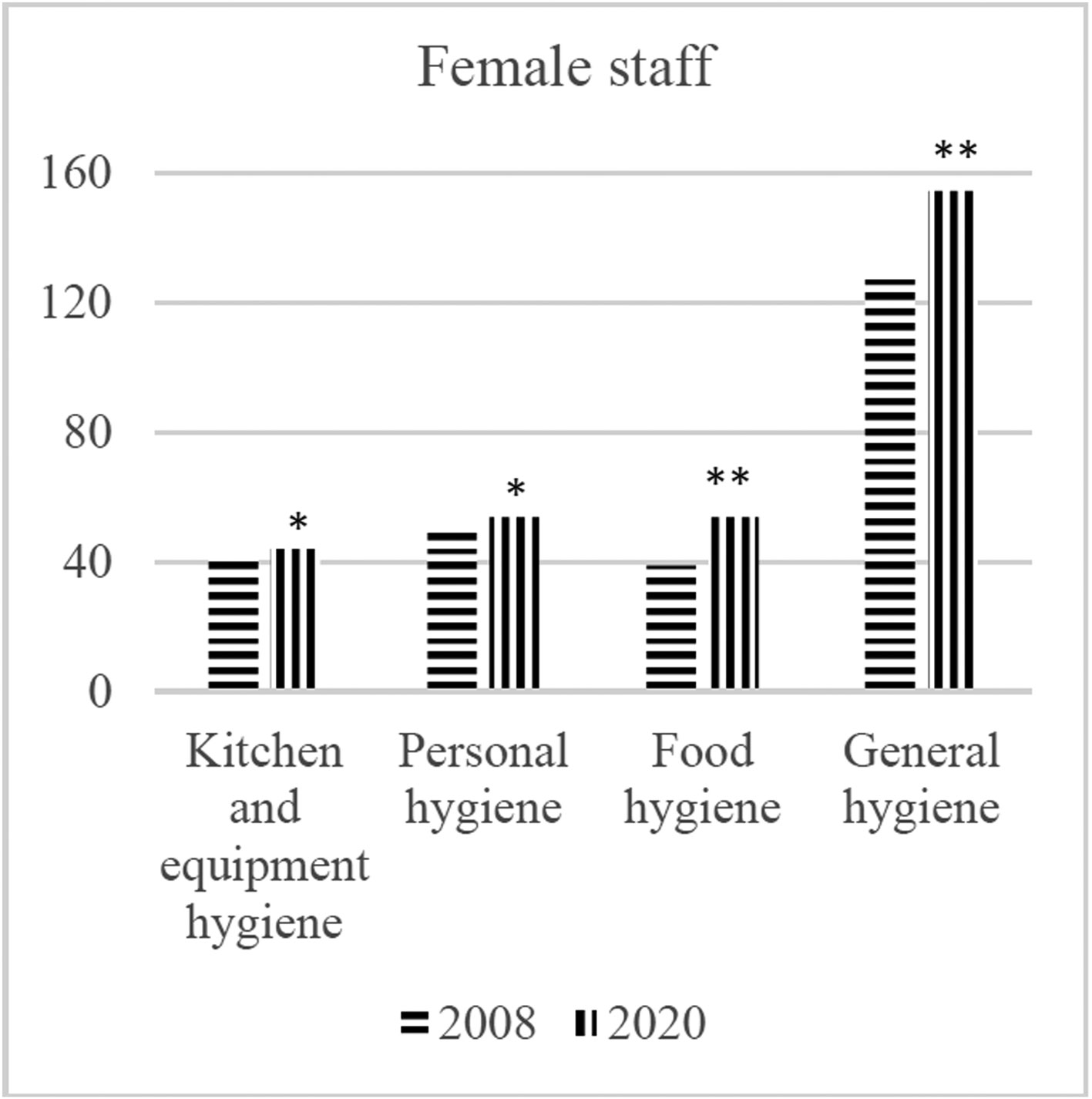
Food safety is a public health concern because foodborne diseases have been increasing in recent years due to several factors such as urbanization, globalization and changes in consumer habits. Many countries in the world, including Turkey have upgraded their laws about food and personnel hygiene in the catering industry and undertaken changes to the organizational structure of their regulatory institutions to protect consumers' health. In this study, it was aimed to evaluate the perceptions of food processors on food safety and to determine whether there has been a change in this matter over the last 12 years. The data has been collected by conducting face to face interviews and having 500 employees from the sector fill in a questionnaire constructed for this purpose. The responses to the questionnaire have been measured by assigning ‘hygiene perception points’ to each respondent according to their replies. These hygiene perception points have been analysed in terms of gender, age, educational level and work experience of the employees involved. The results have revealed that employees between the ages of 26–34, women, university graduates have a higher level of perception of hygiene than other age groups, men, those with lower education levels, respectively. Hygiene perception points were found to be higher compared to the results obtained 12 years ago. The positive changes observed in the hygiene perception points are thought to result from the differences in the legislation of the years in which both studies were conducted. It is thought that the obligatory of providing hygiene and food safety training to individuals working in the catering sector with law changes leads to positive changes in the employees. Legally compulsory training activities can overcome many sanitation and safety problems that result from misinformed or uninformed employees.
Citation: Aslı Uçar, Taha Gökmen Ülger, Funda Pınar Çakıroğlu. What changed between 2008–2020 about Employees' perception of hygiene in the catering industry in Ankara (Turkey)?[J]. AIMS Public Health, 2021, 8(2): 275-284. doi: 10.3934/publichealth.2021021
Food safety is a public health concern because foodborne diseases have been increasing in recent years due to several factors such as urbanization, globalization and changes in consumer habits. Many countries in the world, including Turkey have upgraded their laws about food and personnel hygiene in the catering industry and undertaken changes to the organizational structure of their regulatory institutions to protect consumers' health. In this study, it was aimed to evaluate the perceptions of food processors on food safety and to determine whether there has been a change in this matter over the last 12 years. The data has been collected by conducting face to face interviews and having 500 employees from the sector fill in a questionnaire constructed for this purpose. The responses to the questionnaire have been measured by assigning ‘hygiene perception points’ to each respondent according to their replies. These hygiene perception points have been analysed in terms of gender, age, educational level and work experience of the employees involved. The results have revealed that employees between the ages of 26–34, women, university graduates have a higher level of perception of hygiene than other age groups, men, those with lower education levels, respectively. Hygiene perception points were found to be higher compared to the results obtained 12 years ago. The positive changes observed in the hygiene perception points are thought to result from the differences in the legislation of the years in which both studies were conducted. It is thought that the obligatory of providing hygiene and food safety training to individuals working in the catering sector with law changes leads to positive changes in the employees. Legally compulsory training activities can overcome many sanitation and safety problems that result from misinformed or uninformed employees.

| [1] | World Health Organization Food Safety (2020) .Available from: https://www.who.int/news-room/fact-sheets/detail/food-safety/. |
| [2] |
Velusamy V, Arshak K, Korostynska O, et al. (2010) An overview of foodborne pathogen detection: In the perspective of biosensors. Biotechnol Adv 28: 232-254. doi: 10.1016/j.biotechadv.2009.12.004

|
| [3] | World Health Organization The burden of foodborne diseases in the WHO European region (2017) .Available from: https://www.euro.who.int/__data/assets/pdf_file/0005/402989/50607-WHO-Food-Safety-publicationV4_Web.pdf. |
| [4] | Dewey-Mattia D, Kisselburgh H, Manikonda K, et al. Surveillance for foodborne disease outbreaks–United States, 2016: annual report (2018) .Available from: http://dx.doi.org/10.15585/mmwr.ss6710a1. |
| [5] |
Liu J, Bai L, Li W, et al. (2018) Trends of foodborne diseases in China: lessons from laboratory-based surveillance since 2011. Front Med 12: 48-57. doi: 10.1007/s11684-017-0608-6
|
| [6] |
Urazel B, Çelikel A, Karbeyaz K, et al. (2014) The evaluation of forensic cases reported due to food poisoning. Dicle Med J 41: 113-117. doi: 10.5798/diclemedj.0921.2014.01.0383
|
| [7] |
Özköse Z, Ayoĝlu F (1999) Etiological and demographical characteristics of acute adult poisoning in Ankara, Turkey. Hum Exp Toxicol 18: 614-618. doi: 10.1191/096032799678839446
|
| [8] | Centers for Disease Control and Prevention Burden of Foodborne Illness: Findings (2020) .Available from: https://www.cdc.gov/foodborneburden/burden/index.html. |
| [9] |
Angulo FJ, Jones TF, Angulo FJ, et al. (2006) Eating in restaurants: a risk factor for foodborne disease? Clin Infect Dis 43: 1324-1328. doi: 10.1086/508540
|
| [10] |
Nørrung B, Buncic S (2008) Microbial safety of meat in the European Union. Meat Sci 78: 14-24. doi: 10.1016/j.meatsci.2007.07.032
|
| [11] |
Todd ECD, Greig JD, Bartleson CA, et al. (2007) Outbreaks where food workers have been implicated in the spread of foodborne disease. Part 3. Factors contributing to outbreaks and description of outbreak categories. J Food Prot 70: 2199-2217. doi: 10.4315/0362-028X-70.9.2199
|
| [12] |
Campos AKC, Cardonha ÂMS, Pinheiro LBG, et al. (2009) Assessment of personal hygiene and practices of food handlers in municipal public schools of Natal, Brazil. Food Control 20: 807-810. doi: 10.1016/j.foodcont.2008.10.010
|
| [13] | Motarjemi Y, Lelieveld H (2014) Chapter -1 - Fundamentals in Management of Food Safety in the Industrial Setting: Challenges and Outlook of the 21st Century. Food Safety Management San Diego: Academic Press. |
| [14] |
Sharif L, Al-Malki T (2010) Knowledge, attitude and practice of Taif university students on food poisoning. Food Control 21: 55-60. doi: 10.1016/j.foodcont.2009.03.015
|
| [15] |
Badrie N, Gobin A, Dookeran S, et al. (2006) Consumer awareness and perception to food safety hazards in Trinidad, West Indies. Food Control 17: 370-377. doi: 10.1016/j.foodcont.2005.01.003
|
| [16] |
Jevšnik M, Hlebec V, Raspor P (2008) Food safety knowledge and practices among food handlers in Slovenia. Food Control 19: 1107-1118. doi: 10.1016/j.foodcont.2007.11.010
|
| [17] |
Smigic N, Djekic I, Martins ML, et al. (2016) The level of food safety knowledge in food establishments in three European 492 countries. Food Control 63: 187-194. doi: 10.1016/j.foodcont.2015.11.017
|
| [18] |
Jevšnik M, Hlebec V, Raspor P (2008) Consumers' awareness of food safety from shopping to eating. Food Control 19: 737-745. doi: 10.1016/j.foodcont.2007.07.017
|
| [19] |
Meysenburg R, Albrecht JA, Litchfield R, et al. (2014) Food safety knowledge, practices and beliefs of primary food preparers in families with young children. A mixed methods study. Appetite 73: 121-131. doi: 10.1016/j.appet.2013.10.015
|
| [20] |
Majowicz SE, Diplock KJ, Leatherdale ST, et al. (2015) Food safety knowledge, attitudes and self-reported practices among Ontario high school students. Can J Public Health 106: 520-526. doi: 10.17269/CJPH.106.5213
|
| [21] |
Ovca A, Jevšnik M, Raspor P (2014) Food safety awareness, knowledge and practices among students in Slovenia. Food Control 42: 144-151. doi: 10.1016/j.foodcont.2014.01.036
|
| [22] |
Çakıroğlu FP, Uçar A (2008) Employees' perception of hygiene in the catering industry in Ankara (Turkey). Food Control 19: 9-15. doi: 10.1016/j.foodcont.2007.01.001
|
| [23] | Buyruk L, Şahin N (2002) Otel yiyecek-içecek departmanında çalışan işgörenlerin hijyen algılamaları konusunda bir araştırma Turizmde Sağlık ve Beslenme; Sorunlar ve Çözümler Sempozyumu Bildiriler Kitabı, Haberal Efitim Vakfı, Başkent Üniversitesi, Ankara, Turkey. |
| [24] | Bulduk S (2003) Gıda ve Personel Hijyeni Detay Yayıncılık, Ankara, Turkey. |
| [25] | Astegiano S, Bellio A, Adriano D, et al. (2014) Evaluation of hygiene and safety criteria in the production of a traditional Piedmont cheese. Ital J Food Saf 3: 160-163. |
| [26] |
Bolton DJ, Meally A, Blair IS, et al. (2008) Food safety knowledge of head chefs and catering managers in Ireland. Food Control 19: 291-300. doi: 10.1016/j.foodcont.2007.04.006
|
| [27] |
Cunha DT, Stedefeldt E, Rosso VV (2014) The role of theoretical food safety training on Brazilian food handlers' knowledge, attitude and practice. Food Control 43: 167-174. doi: 10.1016/j.foodcont.2014.03.012
|
| [28] |
Seaman P, Eves A (2006) The management of food safety—the role of food hygiene training in the UK service sector. Int J Hosp M 25: 278-296. doi: 10.1016/j.ijhm.2005.04.004
|
| [29] |
Martins RB, Hogg T, Otero JG (2012) Food handlers' knowledge on food hygiene: The case of a catering company in Portugal. Food Control 23: 184-190. doi: 10.1016/j.foodcont.2011.07.008
|
| [30] |
Gillespie I, Little C, Mitchell R (2000) Microbiological examination of cold ready-to-eat sliced meats from catering establishments in the United Kingdom. J Appl Microbiol 88: 467-474. doi: 10.1046/j.1365-2672.2000.00981.x
|
| [31] |
Al-Shabib NA, Mosilhey SH, Husain FM (2016) Cross-sectional study on food safety knowledge, attitude and practices of male food handlers employed in restaurants of King Saud University, Saudi Arabia. Food Control 59: 212-217. doi: 10.1016/j.foodcont.2015.05.002
|
| [32] |
Ababio PF, Lovatt P (2015) A review on food safety and food hygiene studies in Ghana. Food Control 47: 92-97. doi: 10.1016/j.foodcont.2014.06.041
|
| [33] |
Coleman P, Roberts A (2005) Food hygiene training in the UK: a time for change. Food Serv Technol 5: 17-22. doi: 10.1111/j.1471-5740.2005.00108.x
|
| [34] |
Egan MB, Raats MM, Grubb SM, et al. (2007) A review of food safety and food hygiene training studies in the commercial sector. Food Control 18: 1180-1190. doi: 10.1016/j.foodcont.2006.08.001
|
| [35] |
Faour-Klingbeil D, Todd ECD (2020) Prevention and Control of Foodborne Diseases in Middle-East North African Countries: Review of National Control Systems. Int J Environ Res Public Health 17: 70. doi: 10.3390/ijerph17010070
|
| [36] |
Soon JM, Baines R, Seaman P (2012) Meta-analysis of food safety training on hand hygiene knowledge and attitudes among food handlers. J Food Prot 75: 793-804. doi: 10.4315/0362-028X.JFP-11-502
|
| [37] |
Ghezzi S, Ayoun B (2013) Food safety in the US catering industry: empirical findings. Int J Contemp Hosp M 25: 365-382. doi: 10.1108/09596111311311026
|
| [38] |
Garayoa R, Díez-Leturia M, Bes-Rastrollo M, et al. (2014) Catering services and HACCP: temperature assessment and surface hygiene control before and after audits and a specific training session. Food Control 43: 193-198. doi: 10.1016/j.foodcont.2014.03.015
|
| [39] |
Seaman P (2010) Food hygiene training: Introducing the food hygiene training model. Food Control 21: 381-387. doi: 10.1016/j.foodcont.2009.08.005
|
| [40] |
Pichler J, Ziegler J, Aldrian U, et al. (2014) Evaluating levels of knowledge on food safety among food handlers from restaurants and various catering businesses in Vienna, Austria 2011/2012. Food Control 35: 33-40. doi: 10.1016/j.foodcont.2013.06.034
|
 publichealth-08-02-021-s001.pdf publichealth-08-02-021-s001.pdf |
 |
Figures(2) / Tables(4)

Aslı Uçar, Taha Gökmen Ülger, Funda Pınar Çakıroğlu. What changed between 2008–2020 about Employees' perception of hygiene in the catering industry in Ankara (Turkey)?[J]. AIMS Public Health, 2021, 8(2): 275-284. doi: 10.3934/publichealth.2021021







 DownLoad:
DownLoad: