Citation: Tran Thi Tuyet-Hanh, Tran Khanh Long, Hoang Van Minh, Le Thi Thanh Huong. Longitudinal Household Trends in Access to Improved Water Sources and Sanitation in Chi Linh Town, Hai Duong Province, Viet Nam and Associated Factors[J]. AIMS Public Health, 2016, 3(4): 880-890. doi: 10.3934/publichealth.2016.4.880

| [1] |
Prüss-Ustün A, Bartram J, Clasen T, et al. (2014) Burden of disease from inadequate water, sanitation and hygiene in low- and middle-income settings: a retrospective analysis of data from 145 countries. Trop Med Int Health 19: 894-905. doi: 10.1111/tmi.12329

|
| [2] | Hunter PR, MacDonald AM, Carter RC (2010) Water supply and health. PLoS Med 7: e361. |
| [3] | Curtis V, Cairncross S (2003) Effect of washing hands with soap on diarrhoea risk in the community: a systematic review. Lancet Infect Dis 3: 275-281. |
| [4] | Prüss-Üstün A, Bos R, Gore F, et al. (2008) Safer water, better health: costs, benefits and sustainability of interventions to protect and promote health. Geneva: World Health Organization. |
| [5] | United Nation (2015) Millennium Development Goal (MDG)—GOAL 7: Ensure environmental sustainability. |
| [6] | World Health Organization, UNICEF (2014) Progress on sanitation and drinking-water—2014 update. Geneva, Switzerland. |
| [7] | Tuyet-Hanh TT, Lee JK, Oh J, et al. (2016) Household trends in access to improved water sources and sanitation facilities in Vietnam and associated factors: findings from the Multiple Indicator Cluster Surveys, 2000–2011. Glob Health Action 9: 29434. |
| [8] | General Statistics Office, UNICEF (2015) Viet Nam Multiple Indicator Cluster Survey 2014 Final Report. Hanoi, Vietnam: General Statistics Office and UNICEF. |
| [9] |
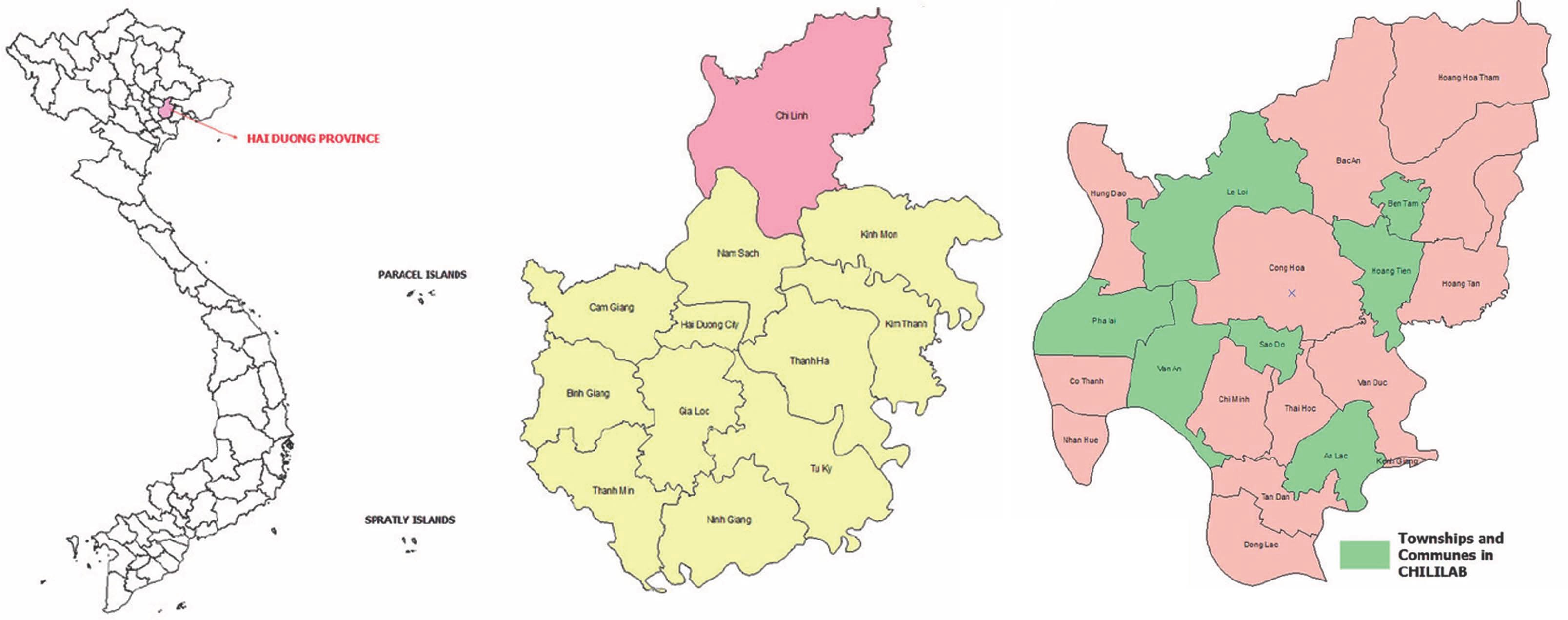
Tran BH NH, Ho HT, Pham CV, Le VT, Le AV. (2013) The Chi Linh Health and Demographic Surveillance System (CHILILAB HDSS). Int J Epidemiol 42: 750-757. doi: 10.1093/ije/dyt053
|
| [10] | JMP Improved and unimproved water sources and sanitation facilities. |
| [11] | The prime Minister of Government (2011) Issuing poverty standard, poor households apply for the period 2011–2015. Decision 09/2011/QĐ-TTg. |
| [12] | International Decade for Action. “Water For Life” 2005–2015 (2012) Gender and Water, Human Right to Water, Water and Cities, and Water Scarcity. United Nations Department of Economic and Social Affairs. |
| [13] | The World Bank (2016) VN-Red River Delta Rural Water Supply and Sanitation Project. Hanoi. |
| [14] |
Bartram J, Cairncross S (2010) Hygiene, Sanitation, and Water: Forgotten Foundations of Health. PLoS Med 7: e1000367. doi: 10.1371/journal.pmed.1000367
|
| [15] | Bartram J, Lewis K, Lenton R, et al. (2005) Focusing on improved water and sanitation for health. Lancet 365: 810-812. |
| [16] | Esrey SA, Potash JB, Roberts L, et al. (1991) Effects of Improved Water Supply and Sanitation on Ascariasis, Diarrhoea, Dracunculiasis, Hookworm Infection, Schistosomiasis and Trachoma. Bull W H O 69: 609-621. |
| [17] |
Bain R, Cronk R, Hossain R, et al. (2014) Global assessment of exposure to faecal contamination through drinking water based on a systematic review. Trop Med Int Health 19: 917-927. doi: 10.1111/tmi.12334
|
| [18] |
Bain R, Cronk R, Wright J, et al. (2014) Fecal Contamination of Drinking-Water in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. PLoS Med 11: e1001644. doi: 10.1371/journal.pmed.1001644
|
| [19] | Shields K, Bain R, Cronk R, et al. (2015) Association of Water Supply Type with Fecal Contamination of Source Water and Household Stored Drinking Water in Developing Countries: A Bivariate Meta-analysis. Environ Health Perspect 123: 1222-1231. |
| [20] | Ministry of agriculture and rural development (2014) Report on the result of the national target program on clean water and rural sanitation in 2013. Ministry of agriculture and rural development. |
Figures(2) / Tables(2)

Tran Thi Tuyet-Hanh, Tran Khanh Long, Hoang Van Minh, Le Thi Thanh Huong. Longitudinal Household Trends in Access to Improved Water Sources and Sanitation in Chi Linh Town, Hai Duong Province, Viet Nam and Associated Factors[J]. AIMS Public Health, 2016, 3(4): 880-890. doi: 10.3934/publichealth.2016.4.880







 DownLoad:
DownLoad: