To investigate the value of urinary suPAR with steroid responsiveness in childhood nephrotic syndrome (NS).
A longitudinal follow-up study was carried out in 92 children diagnosed with nephrotic syndrome (49 initial NS and 43 relapsed NS).
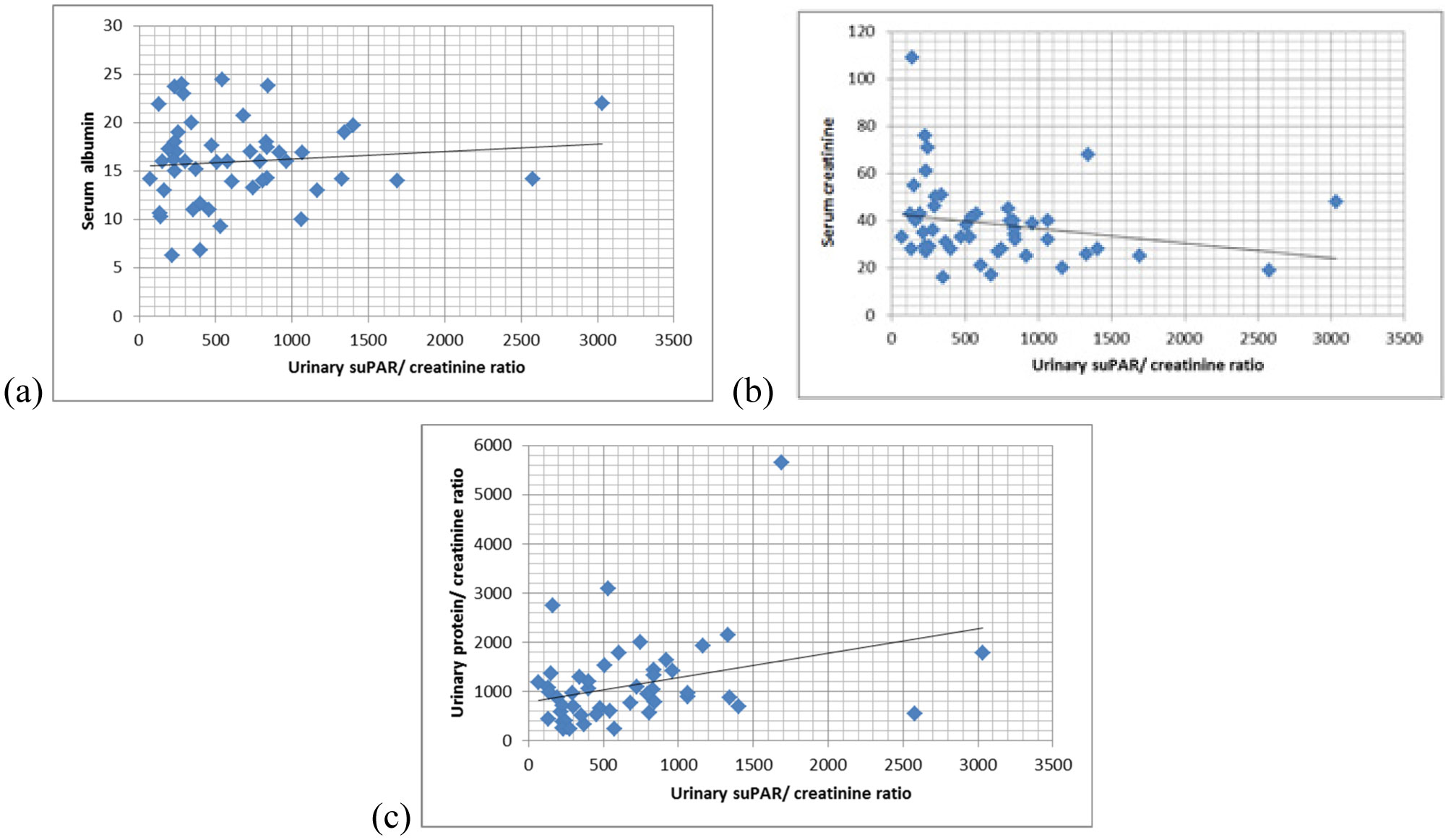
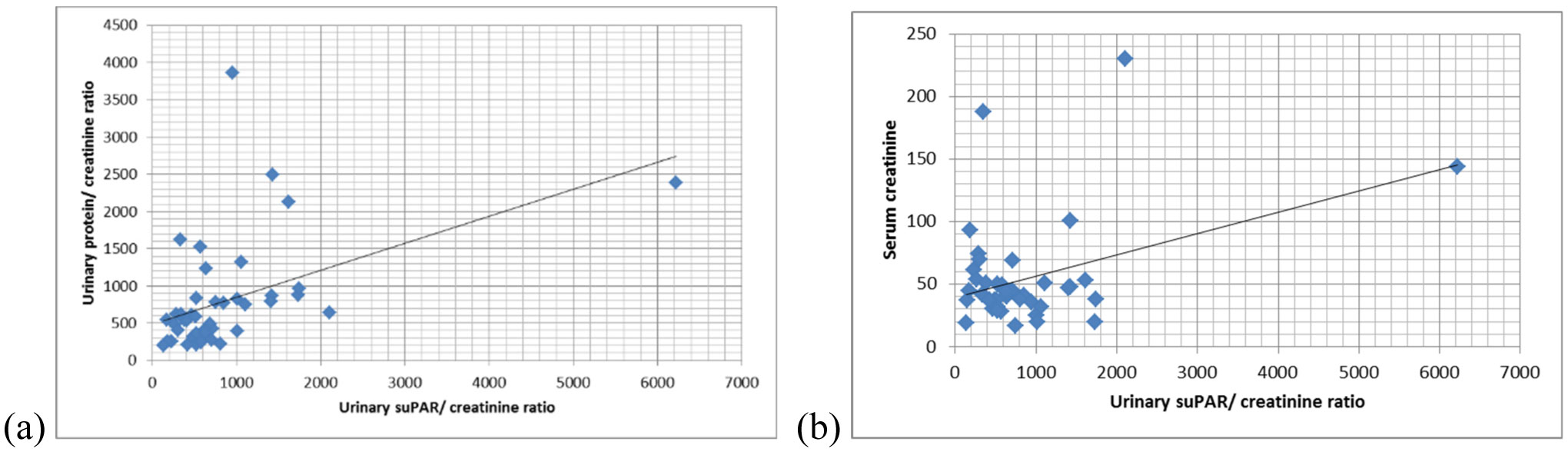
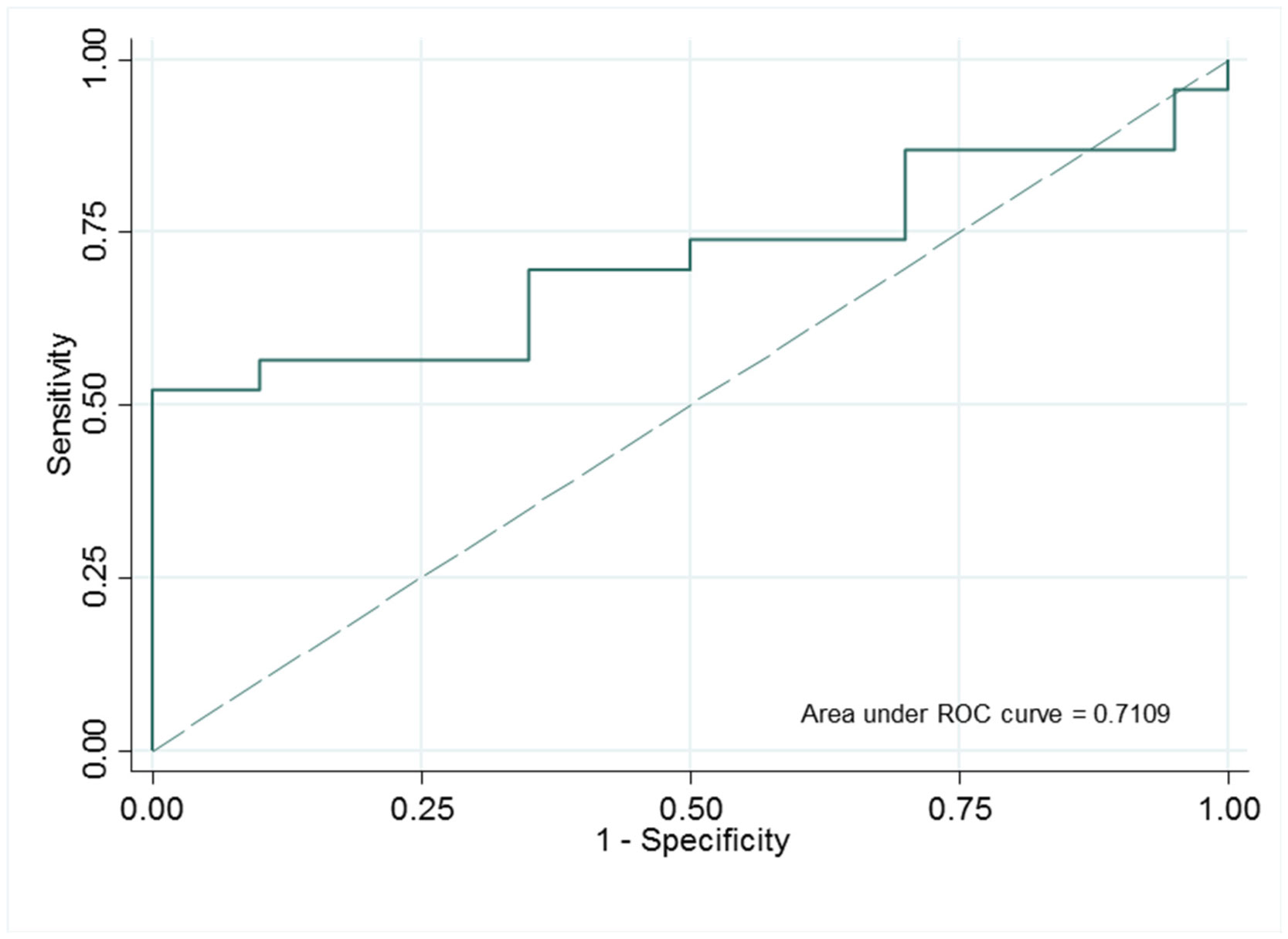
The urinary suPAR/creatinine ratio was significantly high in the relapsed NS group (with a mean = 628 (386–1015) pg/µmol) compared with the initial NS group (mean = 509 (237–840) pg/µmol) and the control group (mean = 248 (88–609) pg/µmol) (p = 0.001). In the initial group, the concentration of urinary suPAR/creatinine ratio was higher in steroid-resistant NS (SRNS) than in steroid-sensitive NS (SSNS) after 6 weeks and 6 months of treatment, but the difference was not significant (p > 0.05). In the relapsed NS group, the concentration of urinary suPAR/creatinine ratio was higher in SRNS than that in SSNS (p = 0.02). The urinary suPAR/creatinine ratio had sensitivity (73.9%) and specificity (89.5%) at the cut-off point of 950 pg/µmol to predict SRNS (p < 0.001).
Urinary suPAR could help distinguish the steroid responsiveness between SRNS and SSNS in children.
Citation: Phuong Anh Le Thy, Kiem Hao Tran, Thuy Yen Hoang Thi, Minh Phuong Phan Thi, Huu Son Nguyen. The value of urinary soluble urokinase plasminogen activator receptor (suPAR) in children with nephrotic syndrome[J]. AIMS Medical Science, 2021, 8(2): 163-174. doi: 10.3934/medsci.2021015
To investigate the value of urinary suPAR with steroid responsiveness in childhood nephrotic syndrome (NS).
A longitudinal follow-up study was carried out in 92 children diagnosed with nephrotic syndrome (49 initial NS and 43 relapsed NS).
The urinary suPAR/creatinine ratio was significantly high in the relapsed NS group (with a mean = 628 (386–1015) pg/µmol) compared with the initial NS group (mean = 509 (237–840) pg/µmol) and the control group (mean = 248 (88–609) pg/µmol) (p = 0.001). In the initial group, the concentration of urinary suPAR/creatinine ratio was higher in steroid-resistant NS (SRNS) than in steroid-sensitive NS (SSNS) after 6 weeks and 6 months of treatment, but the difference was not significant (p > 0.05). In the relapsed NS group, the concentration of urinary suPAR/creatinine ratio was higher in SRNS than that in SSNS (p = 0.02). The urinary suPAR/creatinine ratio had sensitivity (73.9%) and specificity (89.5%) at the cut-off point of 950 pg/µmol to predict SRNS (p < 0.001).
Urinary suPAR could help distinguish the steroid responsiveness between SRNS and SSNS in children.

| [1] | Hari P, Tarafdar S (2020) Nephrotic Syndrome. Nephrology: A Comprehensive Guide to Renal Medicine Wiley-Blackwell, 112-122. |
| [2] |
Hjorten R, Anwar Z, Reidy KJ (2016) Long-term outcomes of childhood onset nephrotic syndrome. Front Pediatr 4: 53. doi: 10.3389/fped.2016.00053

|
| [3] |
Ibrahim T, Flamini E, Mercatali L, et al. (2010) Pathogenesis of osteoblastic bone metastases from prostate cancer. Cancer 116: 1406-1418. doi: 10.1002/cncr.24896
|
| [4] | Alfano M, Cinque P, Giusti G, et al. (2015) Full-length soluble urokinase plasminogen activator receptor down-modulates nephrin expression in podocytes. Sci Rep 5: 1-12. |
| [5] |
Kim EY, Khayyat NH, Dryer SE (2018) Mechanisms underlying modulation of podocyte TRPC6 channels by suPAR: role of NADPH oxidases and Src family tyrosine kinases. Biochim Biophys Acta Mol Basis Dis 1864: 3527-3536. doi: 10.1016/j.bbadis.2018.08.007
|
| [6] |
Wei C, El Hindi S, Li J, et al. (2011) Circulating urokinase receptor as a cause of focal segmental glomerulosclerosis. Nature Med 17: 952-960. doi: 10.1038/nm.2411
|
| [7] | Segarra A, Jatem E, Quiles MT, et al. (2014) Diagnostic value of soluble urokinase-type plasminogen activator receptor serum levels in adults with idiopathic nephrotic syndrome. Nefrología (English Edition) 34: 46-52. |
| [8] |
Palacios CRF, Lieske JC, Wadei HM, et al. (2013) Urine but not serum soluble urokinase receptor (suPAR) may identify cases of recurrent FSGS in kidney transplant candidates. Transplantation 96: 394-399. doi: 10.1097/TP.0b013e3182977ab1
|
| [9] |
Huang J, Liu G, Zhang YM, et al. (2014) Urinary soluble urokinase receptor levels are elevated and pathogenic in patients with primary focal segmental glomerulosclerosis. BMC Med 12: 1-11. doi: 10.1186/1741-7015-12-1
|
| [10] |
Fujimoto K, Imura J, Atsumi H, et al. (2015) Clinical significance of serum and urinary soluble urokinase receptor (suPAR) in primary nephrotic syndrome and MPO-ANCA-associated glomerulonephritis in Japanese. Clin Exp Nephrol 19: 804-814. doi: 10.1007/s10157-014-1067-x
|
| [11] |
Fujimoto K, Kagaya Y, Fujii A, et al. (2020) P0221 soluble urokinase receptor (suPAR) is a predictor of disease state and renal prognosis in primary nephrotic syndrome. Nephrol Dial Transplant 35: gfaa142. P0221. doi: 10.1093/ndt/gfaa142.P0221
|
| [12] |
Cattran DC, Feehally J, Cook HT, et al. (2012) Kidney disease: improving global outcomes (KDIGO) glomerulonephritis work group. KDIGO clinical practice guideline for glomerulonephritis. Kidney Int Suppl 2: 139-274. doi: 10.1038/kisup.2012.9
|
| [13] |
Gordillo R, Spitzer A (2009) The nephrotic syndrome. Pediatr Review 30: 94. doi: 10.1542/pir.30-3-94
|
| [14] |
Schlöndorff D (2014) Are serum suPAR determinations by current ELISA methodology reliable diagnostic biomarkers for FSGS? Kidney Int 85: 499-501. doi: 10.1038/ki.2013.549
|
| [15] |
Winnicki W, Sunder-Plassmann G, Sengölge G, et al. (2019) Diagnostic and prognostic value of soluble urokinase-type plasminogen activator receptor (suPAR) in focal segmental glomerulosclerosis and impact of detection method. Sci Rep 9: 1-9. doi: 10.1038/s41598-019-50405-8
|
| [16] |
Bock ME, Price HE, Gallon L, et al. (2013) Serum soluble urokinase-type plasminogen activator receptor levels and idiopathic FSGS in children: a single-center report. Clin J Am Soc Nephrol 8: 1304-1311. doi: 10.2215/CJN.07680712
|
| [17] |
Peng Z, Mao J, Chen X, et al. (2015) Serum suPAR levels help differentiate steroid resistance from steroid-sensitive nephrotic syndrome in children. Pediatr Nephrol 30: 301-307. doi: 10.1007/s00467-014-2892-6
|
| [18] | Ochocińska A, Jarmużek W, Janas R (2018) The clinical pattern of nephrotic syndrome in children has no effect on the concentration of soluble urokinase receptor (suPAR) in serum and urine. Pol Merkur Lekarski 44: 183-187. |
| [19] |
Mousa SO, Saleh SM, Aly HM, et al. (2018) Evaluation of serum soluble urokinase plasminogen activator receptor as a marker for steroid-responsiveness in children with primary nephrotic syndrome. Saudi J Kidney Dis Transpl 29: 290-296. doi: 10.4103/1319-2442.229266
|
| [20] |
Sun P, Yu L, Huang J, et al. (2019) Soluble urokinase receptor levels in secondary focal segmental glomerulosclerosis. Kidney Dis 5: 239-246. doi: 10.1159/000497353
|
| [21] |
Weidemann DK, Abraham AG, Roem JL, et al. (2020) Plasma soluble urokinase plasminogen activator receptor (suPAR) and CKD progression in children. Am J Kidney Dis 76: 194-202. doi: 10.1053/j.ajkd.2019.11.004
|
| [22] |
Nourbakhsh N, Mak RH (2017) Steroid-resistant nephrotic syndrome: past and current perspectives. Pediatric Health Med Ther 8: 29-37. doi: 10.2147/PHMT.S100803
|
| [23] |
Li F, Zheng C, Zhong Y, et al. (2014) Relationship between serum soluble urokinase plasminogen activator receptor level and steroid responsiveness in FSGS. Clin J Am Soc Nephrol 9: 1903-1911. doi: 10.2215/CJN.02370314
|
| [24] |
Königshausen E, Sellin L (2016) Circulating permeability factors in primary focal segmental glomerulosclerosis: a review of proposed candidates. BioMed Res Int 2016. doi: 10.1155/2016/3765608
|
| [25] |
McCarthy ET, Sharma M, Savin VJ (2010) Circulating permeability factors in idiopathic nephrotic syndrome and focal segmental glomerulosclerosis. Clin J Am Soc Nephrol 5: 2115-2121. doi: 10.2215/CJN.03800609
|
| [26] |
Shuai T, Jing YP, Huang Q, et al. (2019) Serum soluble urokinase type plasminogen activated receptor and focal segmental glomerulosclerosis: a systematic review and meta-analysis. BMJ Open 9: e031812. doi: 10.1136/bmjopen-2019-031812
|
| [27] |
Verdelho M, Ferreira AC, Santos MC, et al. (2018) Soluble urokinase-type plasminogen activator receptor as a biomarker for focal segmental glomerulosclerosis; a retrospective analysis. J Nephropathol 7: 182-187. doi: 10.15171/jnp.2018.38
|
| [28] |
Wada T, Nangaku M (2015) A circulating permeability factor in focal segmental glomerulosclerosis: the hunt continues. Clin Kidney J 8: 708-715. doi: 10.1093/ckj/sfv090
|
Figures(3) / Tables(5)

Phuong Anh Le Thy, Kiem Hao Tran, Thuy Yen Hoang Thi, Minh Phuong Phan Thi, Huu Son Nguyen. The value of urinary soluble urokinase plasminogen activator receptor (suPAR) in children with nephrotic syndrome[J]. AIMS Medical Science, 2021, 8(2): 163-174. doi: 10.3934/medsci.2021015







 DownLoad:
DownLoad: