Citation: Lourdes Franco, Luís J. del Valle, Jordi Puiggalí. Smart systems related to polypeptide sequences[J]. AIMS Materials Science, 2016, 3(1): 289-323. doi: 10.3934/matersci.2016.1.289

| [1] | Deming TJ (2014) Preparation and development of block copolypeptide vesicles and hydrogels for biological and medical applications. Wiley Interdiscip Rev Nanomed Nanobiotechnol 6: 283–297. |
| [2] |
Crucho CIC (2015) Stimuli-Responsive Polymeric Nanoparticles for Nanomedicine. Chem Med Chem 10: 24–38. doi: 10.1002/cmdc.201402290

|
| [3] |
Hamidi M, Shahbazi MA, Rostamizadeh K (2012) Copolymers: efficient carriers for intelligent nanoparticulate drug targeting and gene therapy. Macromol Biosci 12: 144–164. doi: 10.1002/mabi.201100193
|
| [4] |
Kamaly N, Xiao Z, Valencia PM, et al (2012) Targeted polymeric therapeutic nanoparticles: design, development and clinical translation. Chem Soc Rev 41: 2971–3010. doi: 10.1039/c2cs15344k
|
| [5] |
Fleige E, Quadir MA, Haag R (2012) Stimuli-responsive polymeric nanocarriers for the controlled transport of active compounds: concepts and applications. Adv Drug Deliv Rev 64: 866–884. doi: 10.1016/j.addr.2012.01.020
|
| [6] |
Motornov M, Roiter, Y, Tokarev I, et al. (2010) Stimuli-responsive nanoparticles, nanogels and capsules for integrated multifunctional intelligent systems. Prog Polym Sci 35: 174–211. doi: 10.1016/j.progpolymsci.2009.10.004
|
| [7] | Gong J, Chen M, Zheng Y, et al (2012) Polymeric micelles drug delivery system in oncology. J Control Release 159: 312–323. |
| [8] |
Kowalczuk A, Trzcinska R, Trzebicka B, et al. (2014) Loading of polymer nanocarriers: factors, mechanisms and applications. Prog Polym Sci 39: 43–86. doi: 10.1016/j.progpolymsci.2013.10.004
|
| [9] | Zhang Y, Wang C, Huang Y, et al. (2015) Core-crosslinked polymeric micelles with high doxorubicin loading capacity and intracellular pH- and redox-triggered payload release. Eur Polym J 68: 104–114. |
| [10] |
Aluri S, Janib SM, Mackay JA (2009) Environmentallyresponsivepeptides as anticancer drug carriers. Adv Drug Deliver Rev 61: 940–952. doi: 10.1016/j.addr.2009.07.002
|
| [11] | Doty P, Yang JT (1956) Polypeptides VII. Poly-gamma-benzyl-L-glutamate—the helix-coil transition in solution. J Am Chem Soc 78:498–500. |
| [12] |
Blout ER, Lenormant H (1957) Reversible configurational changes in poly-L-lysine hydrochloride induced by water. Nature 179: 960–963. doi: 10.1038/179960a0
|
| [13] |
Applequist J (1963) On helix-coil equilibrium in polypeptides. J Chem Phys 38: 934–941. doi: 10.1063/1.1733787
|
| [14] |
Soliman M, Allen S, Davies MC, et al. (2010) Responsive polyelectrolyte complexes for triggered release of nucleic acid therapeutics. Chem Commun 46: 5421–5433. doi: 10.1039/c0cc00794c
|
| [15] |
Rosu C, Selcuk S, Soto-Cantu E, et al. (2014) Progress in silica polypeptide composite colloidal hybrids: from silica cores to fuzzy shells. Colloid Polym Sci 292: 1009-1040. doi: 10.1007/s00396-014-3170-7
|
| [16] | Holowka EP, Sun VZ, Kamei DT, et al. (2007) Polyarginine segments in block copolypeptides drive both vesicular assembly and intracellular delivery. Nat Mater 6 :52–57. |
| [17] | Battaglia G, Ryan AJ (2005) Bilayers and Interdigitation in Block Copolymer Vesicles. J Am Chem Soc 127: 8757–8764. |
| [18] | Won YY, Davis HT, Bates FS (1999) Giant Wormlike Rubber Micelles. Science 283: 960–963. |
| [19] |
Geng Y, Dalhaimer P, Cai S, et al. (2007) Shape Effects of Filaments versus Spherical Particles in Flow and Drug Delivery. Nat Nanotechnol 2: 249–255. doi: 10.1038/nnano.2007.70
|
| [20] |
Robertson JD, Yealland G, Avila-Olias, et al. (2014) pH-sensitive tubular polymersomes: Formation and applications in cellular delivery. ACS Nano 8: 4650–4661. doi: 10.1021/nn5004088
|
| [21] |
Quadir MA, Martin M, Hammond PT (2014) Clickable Synthetic Polypeptides—Routes to New Highly Adaptive Biomaterials. Chem Mater 26: 461–476. doi: 10.1021/cm4023997
|
| [22] |
Such GK, Yan Y, Johnston APR, et al. (2015) Interfacing Materials Science and Biology for Drug Carrier Design. Adv Mater 27: 2278–2297. doi: 10.1002/adma.201405084
|
| [23] | Van Sluis R,Bhujwalla ZM,Raghunand N, et al. (1999) In Vivo Imaging of Extracellular pH Using 1H MRSI. Magnet Reson Med 41:743–750. |
| [24] | Brahimi-Horn MC,Pouyssegur J (2007)Hypoxia in cancer cell metabolism and pH regulation. Essays Biochem 43: 165–178. |
| [25] |
Qiu Y, Park K (2001) Environment-sensitive hydrogels for drug delivery. Adv Drug Deliv Rev 53: 321–39. doi: 10.1016/S0169-409X(01)00203-4
|
| [26] | Majedi FS, Hasani-Sadrabadi MM, VanDersarl JJ, et al. (2013) On-Chip Fabrication of Paclitaxel-Loaded Chitosan Nanoparticles for Cancer Therapeutics. Adv Funct Mater 24: 432–41. |
| [27] |
Bajaj I, Singhal R (2011) Poly (glutamic acid)—an emerging biopolymer of commercial interest. Bioresource Technol 102: 5551–5561. doi: 10.1016/j.biortech.2011.02.047
|
| [28] |
Kim W, Yamasaki Y, Jang WD, at al. (2010) Thermodynamics of DNA condensation induced by poly (ethylene glycol)-block-polylysine through polyion complex micelle formation. Biomacromolecules 11: 1180–1186. doi: 10.1021/bm901305p
|
| [29] | Bellomo E, Wyrsta MD, Pakstis L, et al. (2004) Stimuli-responsive polypeptide vesicles by conformation-specific assembly. Nat Mater 3: 244−248. |
| [30] | Nowak AP, Breedveld V, Pakstis L, et al. (2002) Rapidly recovering hydrogel scaffolds from self-assembling diblock copolypeptide amphiphiles. Nature 417: 424−428. |
| [31] |
Holowka EP, Pochan DJ, Deming TJ (2005) Charged Polypeptide Vesicles with Controllable Diameter. J Am Chem Soc 127: 12423–12428. doi: 10.1021/ja053557t
|
| [32] |
Carlsen A, Lecommandoux S (2009) Self-assembly of polypeptide-based block copolymer amphiphiles. Curr Opin Colloid In 14: 329–339. doi: 10.1016/j.cocis.2009.04.007
|
| [33] | Quadir MA, Morton SW, Deng ZJ, et al. (2014) PEG–Polypeptide Block Copolymers as pH-Responsive Endosome-Solubilizing Drug Nanocarriers. Mol Pharmaceutics11: 2420–2430. |
| [34] |
Yin H, Kang SW, Bae YH (2009) Polymersome Formation from AB2 Type 3-Miktoarm Star Copolymers. Macromolecules 42: 7456–7464. doi: 10.1021/ma901701w
|
| [35] | Yin H, Kang HC, Huh KM, et al. (2012) Biocompatible, pH-sensitive AB2 miktoarm polymer-based polymersomes: preparation, characterization, and acidic pH-activated nanostructural transformation. J Mater Chem 22: 19168–19178. |
| [36] |
Kragh-Hansen H, Chuang VT, Otagiri M (2002) Practical aspects of the ligand-binding and enzymatic properties of human serum albumin. Bio Pharm Bull 25: 695–704 doi: 10.1248/bpb.25.695
|
| [37] |
Ming X, Carver K, Wu L (2013) Albumin-Based Nanoconjugates for Targeted Delivery of Therapeutic Oligonucleotides. Biomaterials 34: 7939–7949. doi: 10.1016/j.biomaterials.2013.06.066
|
| [38] |
Du C, Deng D, Shan L, at al. (2013) A pH-sensitive doxorubicin prodrug based on folate-conjugated BSA for tumor-targeted drug delivery. Biomaterials 34: 3087–3097. doi: 10.1016/j.biomaterials.2013.01.041
|
| [39] |
Xia W, Low PS (2010) Folate-targeted therapies for cancer. J Med Chem 53: 6811–6824. doi: 10.1021/jm100509v
|
| [40] |
Sudimack J, Lee RJ (2000) Targeted drug delivery via the folate receptor. Adv Drug Deliv Rev 41: 147–162. doi: 10.1016/S0169-409X(99)00062-9
|
| [41] |
Lu Y, Low PS (2002) Folate-mediated delivery of macromolecular anticancer therapeutic agents. Adv Drug Deliv Rev 54: 675–693. doi: 10.1016/S0169-409X(02)00042-X
|
| [42] |
Nistor MT, Chiriac AP, Nita LE, et al. (2013) Semi-interpenetrated polymer networks of hyaluronic acid modified with poly(aspartic acid). J Polym Res 20: 86. doi: 10.1007/s10965-013-0086-8
|
| [43] |
Mackay JA, Chilkoti A (2008) Temperature sensitive peptides: engineering hyperthermia-directed therapeutics. Int J Hypertherm 24: 483–495. doi: 10.1080/02656730802149570
|
| [44] |
Aluri S, Janib SM, Mackay JA (2009) Environmentally responsive peptides as anticancer drug carriers. Adv Drug Deliver Rev 61: 940–952. doi: 10.1016/j.addr.2009.07.002
|
| [45] |
Ruszczak Z (2003) Effect of collagen matrices on dermal wound healing. Adv Drug Deliv Rev 55: 1595–1611. doi: 10.1016/j.addr.2003.08.003
|
| [46] |
Lupas A (1996) Coiled coils: new structures and new functions. Trends Biochem Sci 21: 375–382. doi: 10.1016/S0968-0004(96)10052-9
|
| [47] | Petka WA, Harden JL, McGrath KP, et al. (1998) Reversible hydrogels from self-assembling artificial proteins. Science 281: 389–392. |
| [48] |
Al-Ahmady ZS, Al-Jamal WT, Bossche JV, et al. (2012) Lipid–Peptide Vesicle Nanoscale Hybrids for Triggered Drug Release by Mild Hyperthermia in Vitro and in Vivo. ACS Nano 6: 9335–9346. doi: 10.1021/nn302148p
|
| [49] |
Banta S, Wheeldon IR, Blenner M (2010) Protein engineering in the development of functional hydrogels. Annu Rev Biomed Eng 12:167–186. doi: 10.1146/annurev-bioeng-070909-105334
|
| [50] |
Huang HC, Koria P, Parker S, et al. (2008) Optically responsive gold nanorod-polypeptide assemblies. Langmuir 24: 14139–14144. doi: 10.1021/la802842k
|
| [51] | Lin Y, Xia X, Wang M, et al. (2014) Genetically programmable thermoresponsive plasmonic gold/silk-elastin protein core/shell nanoparticles. Langmuir 30: 4406–4414. |
| [52] |
Chilkoti A, Dreher MR, Meyer DE, et al. (2002) Targeted drug delivery by thermally responsive polymers. Adv Drug Deliver Rev 54: 613–630. doi: 10.1016/S0169-409X(02)00041-8
|
| [53] |
Maeda H, Seymour LW, Miyamoto Y (1992) Conjugates of anticancer agents and polymers: advantages of macromolecular therapeutics in vivo. Bioconjug Chem 3: 351–362. doi: 10.1021/bc00017a001
|
| [54] | Schmaljohann D (2006) Thermo- and pH-responsive polymers in drug delivery. Adv Drug Deliver Rev 58: 1655–1670. |
| [55] |
Raucher D, Massodi I, Bidwell GL (2008) Thermally targeted delivery of chemotherapeutics and anti-cancer peptides by elastin like polypeptide. Expert Opin Drug Deliver 5: 353–369. doi: 10.1517/17425247.5.3.353
|
| [56] |
Massodi I, Thomas E, Raucher D (2009) Application of thermally responsive elastin-like polypeptide fused to a lactoferrin-derived peptide for treatment of pancreatic cancer. Molecules 14: 1999–2015. doi: 10.3390/molecules14061999
|
| [57] |
MacEwan SR, Chilkoti A (2010) Elastin-like polypeptides: biomedical applications of tunable biopolymers. Biopolymers 94: 60–77. doi: 10.1002/bip.21327
|
| [58] |
Liu W, Dreher MR, Furgeson DY, et al (2006) Tumor accumulation, degradation and pharmacokinetics of elastin-like polypeptides in nude mice. J Control Release 116: 170–178. doi: 10.1016/j.jconrel.2006.06.026
|
| [59] |
McDaniel JR, Callahan DJ, Chilkoti A, et al. (2010) Drug delivery to solid tumors by elastin-like polypeptides. Adv Drug Deliver Rev 62: 1456–1467. doi: 10.1016/j.addr.2010.05.004
|
| [60] |
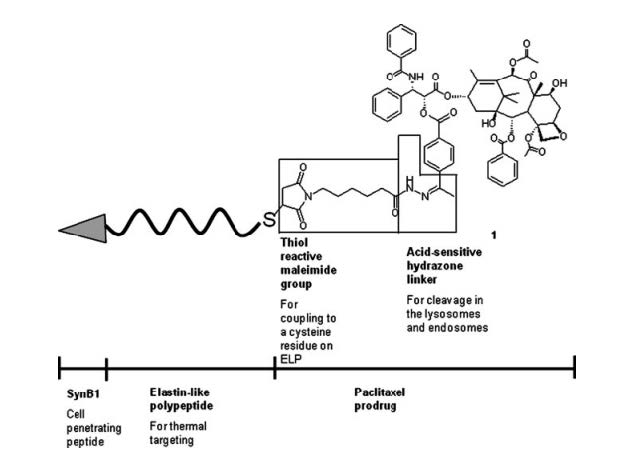
Moktan S, Ryppa C, Kratz F, et al. (2012) A thermally responsive biopolymer conjugated to an acid-sensitive derivative of paclitaxel stabilizes microtubules, arrests cell cycle, and induces apoptosis. Invest New Drugs 30: 236–248. doi: 10.1007/s10637-010-9560-x
|
| [61] | Rousselle C, Smirnova M, Clair P, et al. (2001) Enhanced delivery of doxorubicin into the brain via a peptide-vector-mediated strategy: saturation kinetics and specificity. J Pharmacol Exp Ther 296: 124–13. |
| [62] | Jiang C, Tsukruk VV, et al. (2006) Freestanding Nanostructures via Layer-by-Layer Assembly. Adv Mater 18: 829–840. |
| [63] | Johnston APR, Cortez C, Angelatos AS, et al. (2006) Layer-by-layer engineered capsules and their applications. Curr Opin Colloid Interface Sci 11: 203–209. |
| [64] | Wattendorf U, Kreft O, Textor M, et al. (2008) Stable stealth function for hollow polyelectrolyte microcapsules through a poly(ethylene glycol) grafted polyelectrolyte adlayer. Biomacromolecules 9: 100–108. |
| [65] | Kamphuis MM, Johnston AP, Such GK, et al. (2010) Targeting of cancer cells using click-functionalized polymer capsules. J Am Chem Soc 132: 15881–15883. |
| [66] |
Golonka M, Bulwan M, Nowakowska M, et al. (2011) Thermoresponsive multilayer films based on ionic elastin-like recombinamers. Soft Matter 7: 9402–9409. doi: 10.1039/c1sm06276j
|
| [67] |
Chen X, Zhang W, Li K, et al. (2012) Thermoresponsive oligoprolines. Soft Matter 8: 4869–4872. doi: 10.1039/c2sm25451d
|
| [68] |
Chen C, Wang Z, Li Z (2011) Thermoresponsive Polypeptides from Pegylated Poly-l-glutamate. Biomacromolecules 12: 2859–2863. doi: 10.1021/bm200849m
|
| [69] | Fu X, Shen Y, Fu W (2013) Thermoresponsive Oligo(ethylene glycol) Functionalized Poly-l-cysteine. Macromolecules46: 3753–3760. |
| [70] |
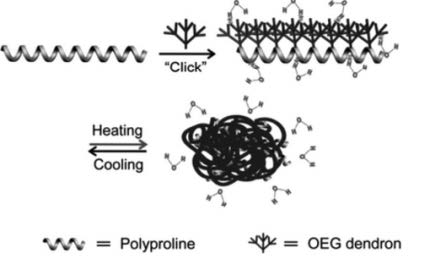
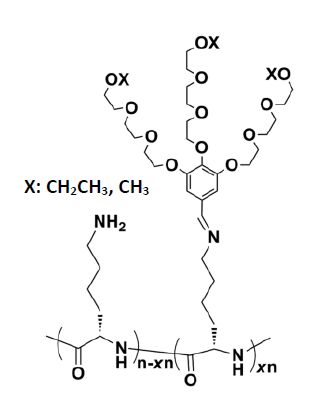
Zhang X, Li W, Zhao X, et al. (2013) Thermoresponsive Dendronized Polyprolines via the “Grafting to” Route. Macromol Rapid Commun 34: 1701–1707. doi: 10.1002/marc.201300605
|
| [71] |
Yan J, Liu K, Zhang X, at al. (2015) Dynamic covalent polypeptides showing tunable secondary structures and thermoresponsiveness. J Polym Sci A 53: 33–41. doi: 10.1002/pola.27433
|
| [72] |
Lam RTS, Belenguer A, Roberts SL (2005) Amplification of Acetylcholine-Binding Catenanes from Dynamic Combinatorial Libraries. Science 308: 667–669. doi: 10.1126/science.1109999
|
| [73] |
Carnall JMA, Waudby CA, Belenguer AM, et al (2010) Mechanosensitive Self-Replication Driven by Self-Organization. Science 327: 1502–1506. doi: 10.1126/science.1182767
|
| [74] |
Li J, Nowak P, Otto S (2013) Dynamic Combinatorial Libraries: From Exploring Molecular Recognition to Systems Chemistry. J Am Chem Soc 135: 9222–9239. doi: 10.1021/ja402586c
|
| [75] | Matanović MR, Kristl J, Grabnar PA (2014) Thermoresponsive polymers: Insights into decisive hydrogel characteristics, mechanisms of gelation, and promising biomedical applications. Int J Pharm 472: 262–275. |
| [76] | Joly-Duhamel C, Hellio D, Djabourov M (2002) All gelatin networks: 1. Biodiversity and physical chemistry. Langmuir 18: 7208–7217. |
| [77] | Yang H, Kao W (2006) Thermoresponsive gelatin/monomethoxy poly(ethylene glycol)–poly(d,l-lactide) hydrogels: formulation, characterization, and antibacterial drug delivery. Pharm Res 23: 205–214. |
| [78] | Ohya S, Matsuda T (2005) Poly(N-isopropylacrylamide) (PNIPAM)-grafted gelatin as thermoresponsive three-dimensional artificial extracellular matrix: molecular and formulation parameters vs. cell proliferation potential. J Biomat Sci-Polym 16: 809–827. |
| [79] |
Huang J, Hastings CL, Duffy GP, et al. (2013) Supramolecular Hydrogels with Reverse Thermal Gelation Properties from (Oligo)tyrosine Containing Block Copolymers. Biomacromolecules 14: 200–206. doi: 10.1021/bm301629f
|
| [80] |
Cheng Y, He C, Xiao C, et al. (2012) Decisive Role of Hydrophobic Side Groups of Polypeptides in Thermosensitive Gelation. Biomacromolecules 13: 2053–2059. doi: 10.1021/bm3004308
|
| [81] | Park MH, Joo MK, Choi BG, et al. (2012) Biodegradable Thermogels. Acc Chem Res 45: 424–433. |
| [82] | Oh HJ, Joo MK, Sohn YS, et al. (2008) Secondary Structure Effect of Polypeptide on Reverse Thermal Gelation and Degradation of l/dl-Poly(alanine)–Poloxamer–l/dl-Poly(alanine) Copolymers. Macromolecules 41:8204–8209. |
| [83] | Zhang S, Fu W, Li Z (2014) Supramolecular hydrogels assembled from nonionic poly(ethylene glycol)-b-polypeptide diblocks containing OEGylated poly-L-glutamate. Polym Chem 5: 3346–3351. |
| [84] | Zhang DJ, Alvarez MV, Sofroniew TJ (2015) Deming. Design and Synthesis of Nonionic Copolypeptide Hydrogels with Reversible Thermoresponsive and Tunable Physical Properties. Biomacromolecules16: 1331–1340. |
| [85] |
Huang J, Bonduelle C, Thévenot J, et al. (2012) Biologically Active polymersomes from Amphiphilic Glycopeptides. J Am Chem Soc 134: 119–122. doi: 10.1021/ja209676p
|
| [86] |
Schatz C, Louguet S, Meins JFL, et al. (2009) Polysaccharide block polypeptide copolymers vesicles towards synthetic viral capsids. Angew Chem Int Ed 48: 2572–2575. doi: 10.1002/anie.200805895
|
| [87] |
Zhang A, Zhang Z, Shi F, et al. (2013) Redox-Sensitive Shell-Crosslinked Polypeptide-block-Polysaccharide Micelles for Efficient Intracellular Anticancer Drug Delivery. Macromol Biosci 13: 1249–1258. doi: 10.1002/mabi.201300175
|
| [88] |
Liu L, Liu P (2015) Synthesis strategies for disulfide bond-containing polymer-based drug delivery system for reduction-responsive controlled release. Front Mater Sc 9: 211–226. doi: 10.1007/s11706-015-0283-y
|
| [89] |
Wang K, Luo GF, Liu Y, et al. (2012) Redox-sensitive shell cross-linked PEG-polypeptidehybrid micelles for controlled drug release. Polym Chem 3: 1084–1090. doi: 10.1039/c2py00600f
|
| [90] |
Beloor J, Ramakrishna S, Nam K, et al. (2015) Effective Gene Delivery into Human Stem Cells with a Cell-Targeting Peptide-Modified Bioreducible Polymer. Small 11: 2069–2079. doi: 10.1002/smll.201402933
|
| [91] |
Burnett JC, Rossi JJ (2012) RNA-Based Therapeutics: Current Progress and Future Prospects. Chem Biol 19: 60–71. doi: 10.1016/j.chembiol.2011.12.008
|
| [92] |
Cavalieri F, Beretta G, Cui J, et al. (2015) Redox-Sensitive PEG–Polypeptide Nanoporous Particles for Survivin Silencing in Prostate Cancer Cells. Biomacromolecules 16: 2168–2178. doi: 10.1021/acs.biomac.5b00562
|
| [93] |
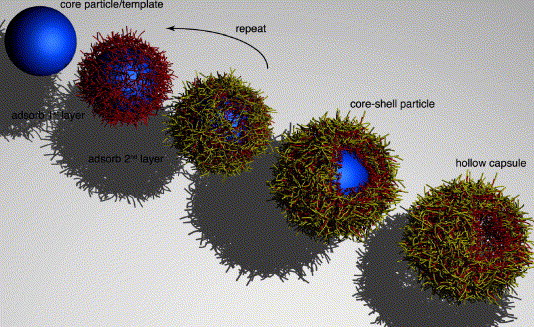
Wang Y, Yu A, Caruso F (2005) Nanoporous Polyelectrolyte Spheres Prepared by Sequentially Coating Sacrificial Mesoporous Silica Spheres. Angew Chem Int Ed 44: 2888–2892. doi: 10.1002/anie.200462135
|
| [94] | Manickam DS, Oupický D (2006) Multiblock Reducible Copolypeptides Containing Histidine-Rich and Nuclear Localization Sequences for Gene Delivery. Bioconjugate Chem17: 1395–1403. |
| [95] | Rosengart AJ, Kaminski MD, Chen HT, et al. (2005) Magnetizable implants and functionalized magnetic carriers: a novel approach for noninvasive yet targeted drug delivery. J Magn Magn Mater 293: 633–638 |
| [96] |
Mornet S, Vasseur S, Grasset F, et al. (2006) Magnetic nanoparticle design for medical applications. Prog Solid State Ch 34: 237–47. doi: 10.1016/j.progsolidstchem.2005.11.010
|
| [97] | Lee H, Shao HP, Huang YQ, et al. (2005) Synthesis of MRI contrast agent by coating superparamagnetic iron oxide with chitosan. IEEE T Magn 41:4102–4. |
| [98] |
Liu XQ, Kaminski MD, Riffle JS, et al. (2007) Preparation and characterization of biodegradable magnetic carriers by single emulsion-solvent evaporation. J Magn Magn Mater 311: 84–7. doi: 10.1016/j.jmmm.2006.10.1170
|
| [99] |
Ju XJ, Xie R, Yang L (2009) Biodegradable ‘intelligent’ materials in response to physical stimuli for biomedical applications. Expert Opin Ther Pat 19: 493–507. doi: 10.1517/13543770902771282
|
| [100] |
Aili D, Stevens MM (2010) Bioresponsive peptide-inorganic hybrid nanomaterials. Chem Soc Rev 39: 3358–3370. doi: 10.1039/b919461b
|
| [101] |
Pan BF, Cui DX, Sheng Y, et al. (2007) Dendrimer-modified magnetic nanoparticles enhance efficiency of gene delivery system. Cancer Res 67: 8156–8163. doi: 10.1158/0008-5472.CAN-06-4762
|
| [102] | Digigow RG, Dechézelles JF, Dietsch H, et al. (2014) Preparation and characterization of functional silica hybrid magnetic nanoparticles. J Magn Magn Mater 362: 72–79. |
| [103] | Digigow RG, Vanhecke D, Rothen-Rutishauser B, et al. (2015)Uptake and Intracellular Fate of Peptide Surface-Functionalized Silica Hybrid Magnetic Nanoparticles In Vitro. Part Part Syst Char 33: 188–196. |
| [104] | Lerche MH, Jensen PR, Karlsson M, et al. (2015) NMR Insights into the Inner Workings of Living Cells. Anal Chem 87: 119–132. |
| [105] |
Boutin C, Desvaux H, Carrière M, et al. (2011) Hyperpolarized129Xe NMR signature of living biological cells. NMR Biomed 24: 1264–1269. doi: 10.1002/nbm.1686
|
| [106] |
Kotera N, Dubost E, Milanole G, et al. (2015) A doubly responsive probe for the detection of Cys4-tagged proteins. Chem Commun 51: 11482–11484. doi: 10.1039/C5CC04721H
|
| [107] |
Kwon S, Kim BJ, Lim HK, et al. (2015) Magnetotactic molecular architectures from self-assembly of β-peptide foldamers. Nat Commun 6: 8747. doi: 10.1038/ncomms9747
|
| [108] |
Goodman CM, Choi S, Shandler S, et al. (2007) Foldamers as versatile frameworks for the design and evolution of function. Nat Chem Biol 3: 252–262. doi: 10.1038/nchembio876
|
| [109] |
Kwon S, Jeon A, Yoo S, et al. (2010) Unprecedented Molecular Architectures by the Controlled Self-Assembly of a β-Peptide Foldamer. Angew Chem Int Ed 49: 8232–8236. doi: 10.1002/anie.201003302
|
| [110] | Lefèvre CT, Abreu F, Lins U, et al. (2011) A bacterial backbone: magnetosomes in magnetotactic bacteria. M. Rai, N. Duran (Eds.) in Metal nanoparticles in microbiology, Springer-Verlag, Berlin (2011), 75–102. |
| [111] |
Unger E, Metzger P, Krupinski E, et al. (2000) The use of a thrombus-specific ultrasound contrast agent to detect thrombus in arteriovenous fistulae. Invest Radiol 35: 86–89. doi: 10.1097/00004424-200001000-00010
|
| [112] | Weller GER, Wong MKK, Modzelewski RA, et al. (2005) Ultrasonic imaging of tumor angiogenesis using contrast microbubbles targeted via the tumor-binding peptide arginine-arginine-leucine. Cancer Res 65: 533–539. |
| [113] | Linker RA, Reinhardt M, Bendszus M, et al. (2005) In vivo molecular imaging of adhesion molecules in experimental autoimmune encephalomyelitis (EAE). J Autoimmun 25:199–205. |
| [114] |
Sirsi S, Borden M (2009) Microbubble compositions, properties and biomedical applications. Bubble Sci Eng Technol 1: 3–17. doi: 10.1179/175889709X446507
|
| [115] |
Cochran MC, Eisenbrey J, Ouma RO, et al. (2011) Doxorubicin and paclitaxel loaded microbubbles for ultrasound triggered drug delivery. Int J Pharm 414:161–170. doi: 10.1016/j.ijpharm.2011.05.030
|
| [116] | Borden MA, Sarantos MR, Stieger SM (2006) Ultrasound radiation force modulates ligand availability on targeted contrast agents. Mol Imag 5:139–147. |
| [117] |
Lum AFH, Borden MA, Dayton PA (2006) Ultrasound radiation force enables targeted deposition of model drug carriers loaded on microbubbles. J Control Release 111: 128–134. doi: 10.1016/j.jconrel.2005.11.006
|
| [118] |
Borden MA,Zhang H, Gillies RJ, et al. (2008) A stimulus-responsive contrast agent for ultrasound molecular imaging. Biomaterials 29: 597–606. doi: 10.1016/j.biomaterials.2007.10.011
|
| [119] |
Bloch M, Jablonowski L, Yavin E, et al. (2015) Multi-modal detection of colon malignancy by NIR-tagged recognition polymers and ultrasound contrast agents. Int J Pharm 478: 504–516. doi: 10.1016/j.ijpharm.2014.11.066
|
| [120] |
Eisenbrey JR, Burstein OM, Kambhampati R, et al. (2010) Development and optimization of a doxorubicin loaded poly(lactic acid) contrast agent for ultrasound directed drug delivery. J Control Release 143: 38–44. doi: 10.1016/j.jconrel.2009.12.021
|
| [121] |
Eisenbrey JR, Soulen MC, Wheatley MA (2010) Delivery of encapsulated doxorubicin by ultrasound-mediated size reduction of drug-loaded polymer contrast agents. IEEE Trans Biomed Eng 57: 24–28. doi: 10.1109/TBME.2009.2030497
|
| [122] |
Duncan R, Gac-Breton S, Keane R (2001) Polymer-drug conjugates, PDEPT and PELT: basic principles for design and tranfer from the laboratory to clinic. J Control Release 74: 135–46. doi: 10.1016/S0168-3659(01)00328-5
|
| [123] | Terada T, Iwai M, Kawakami S (2006) Novel PEG-matrix metalloproteinase-2 cleavable peptide-lipid containing galactosylated liposomes for hepatocellular carcinoma-selective targeting. J Control Release 111: 333–42. |
| [124] | Lee SJ, Jeong YI, Park HK, et al. (2015) Enzyme-responsive doxorubicin release from dendrimer nanoparticles for anticancerdrug delivery. Int J Nano 10: 5489–550. |
| [125] |
Secret E, Kelly SJ, Crannell KE, et al. (2014) Enzyme-Responsive Hydrogel Microparticles for Pulmonary Drug Delivery. ACS Appl Mater Interfaces 6: 10313–10321. doi: 10.1021/am501754s
|
| [126] |
Secret E, Crannell KE, Kelly SJ, et al. (2015) Matrix metalloproteinase-sensitive hydrogel microparticles for pulmonary drug delivery of small molecule drugs or proteins. J Mater Chem B 3: 5629–5634. doi: 10.1039/C5TB00443H
|
| [127] | Angelos S, Khashab NM, Yang YW, et al. (2009) pH clock-operated mechanized nanoparticles. J Am Chem Soc 131: 12912–12914. |
| [128] |
Luo Z, Ding X, Hu Y, et al. (2013) Engineering a hollow nanocontainer platform with multifunctional molecular machines for tumor-targeted therapy in vitro and in vivo. ACS Nano 7: 10271–10284. doi: 10.1021/nn404676w
|
| [129] |
Li J, Liu F, Shao Q, et al. (2014) Enzyme-Responsive Cell-Penetrating Peptides Conjugated Mesoporous Silica Quantum Dots Nanocarriers for Controlled Release of Nucleus-Targeted Drug Molecules and Real-Time Intracellular Fluorescence Imaging of Tumor Cells. Adv Healthcare Mater 3: 1230–123. doi: 10.1002/adhm.201300613
|
| [130] | Cheng YJ, Luo GF, Zhu JY, et al. (2015) Enzyme-Induced and Tumor-Targeted Drug Delivery System Based on Multifunctional Mesoporous Silica Nanoparticles. ACS Appl Mater Interfaces7: 9078–9087. |
| [131] |
Liu J, Zhang B, Luo Z, et al. (2015) Enzyme responsive mesoporous silica nanoparticles for targeted tumor therapy in vitro and in vivo. Nanoscale 7: 3614–3626. doi: 10.1039/C5NR00072F
|
| [132] |
del Mercato LL, Ferraro MM, Baldassarre F, et al. (2014) Biological applications of LbL multilayer capsules: From drug delivery to sensing. Adv Colloid Interface Sci 207: 139–154. doi: 10.1016/j.cis.2014.02.014
|
| [133] |
De Geest BG, Vandenbroucke RE, Guenther AM, et al. (2006) Intracellularly degradable polyelectrolyte microcapsules. Adv Mater 18: 1005–1009. doi: 10.1002/adma.200502128
|
| [134] |
Ochs CJ, Such GK, Yan Y, et al. (2010) Biodegradable click capsules with engineered drug-loaded multilayers. Acs Nano 4: 1653–1663. doi: 10.1021/nn9014278
|
| [135] |
Aller SG, Yu J, Ward A, et al. (2009) Structure of P-Glycoprotein Reveals a Molecular Basis for Poly-Specific Drug Binding. Science 323: 1718–1722. doi: 10.1126/science.1168750
|
| [136] |
Yan Y, Ochs C, Such G, et al. (2010) Bypassing multidrug resistance in cancer cells with biodegradable polymer capsules. Adv Mater 22: 5398–5403. doi: 10.1002/adma.201003162
|
| [137] |
Zhao Y (2007) Rational design of light-controllable polymer micelles. Chem Rec 7: 286–294. doi: 10.1002/tcr.20127
|
| [138] | Alatorre-Meda M, Alvarez-Lorenzo C, Concheiro A, et al. (2013) UV and Near-IR Triggered Release from Polymeric Micelles and Nanoparticles, in Smart Materials for Drug Delivery (Eds.: C. Alvarez-Lorenzo, A. Concheiro), RSC Publishing,Cambridge 304–348. |
| [139] |
Hernanz D, Nunez V, Sancho A, et al. (2001) Hydroxycinnamic acids and ferulic acid dehydrodimers in barley and processed barley. J Agric Food Chem 49: 4884–4888. doi: 10.1021/jf010530u
|
| [140] |
Hoff WD, Dux P, Hard K, et al. (1994) Thiol ester-linked p-coumaric acid as a new photoactive prosthetic group in a protein with rhodopsin-like photochemistry. Biochemistry 33: 13959–13962. doi: 10.1021/bi00251a001
|
| [141] |
Wang G, Tong X, Zhao Y (2004) Preparation of Azobenzene-Containing Amphiphilic Diblock Copolymers for Light-Responsive Micellar Aggregates. Macromolecules 37: 8911–8917. doi: 10.1021/ma048416a
|
| [142] |
Shi D, Matsusaki M, Kaneko T, et al. (2008) Photo-Cross-Linking and Cleavage Induced Reversible Size Change of Bio-Based Nanoparticles. Macromolecules 41: 8167–8172. doi: 10.1021/ma800648e
|
| [143] |
Zhao Y (2012) Light-Responsive Block Copolymer Micelles. Macromolecules 45: 3647–3657. doi: 10.1021/ma300094t
|
| [144] |
Kotharangannagari VK, Sánchez-Ferrer A, Ruokolainen J, et al. (2011) Photo-Responsive Reversible Aggregation and Dissolution of Rod-Coil Polypeptide Diblock Copolymers. Macromolecules 44: 4569–4573. doi: 10.1021/ma2008145
|
| [145] |
Kumar S, Allard JF, Morris D, et al. (2012) Near-infrared light sensitive polypeptide block copolymer micelles for drug delivery. J Mater Chem 22: 7252–7257. doi: 10.1039/c2jm16380b
|
| [146] |
Li Y, Qian Y, Liu T, et al. (2012) Light-triggered concomitant enhancement of magnetic resonance imaging contrast performance and drug release rate of functionalized amphiphilic diblock copolymer micelles. Biomacromolecules 13: 3877–3886. doi: 10.1021/bm301425j
|
| [147] | Liu G, Liu N, Zhou L, et al. (2015) NIR-responsive polypeptide copolymer upconversion composite nanoparticles for triggered drug release and enhanced cytotoxicity. Polym Chem 6: 4030–4039 |
| [148] |
Martinez-Cuezva A, Valero-Moya S, Alajarin M, et al. (2015) Light-responsive peptide [2]rotaxanes as gatekeepers of mechanised nanocontainers. Chem Commun 51: 14501–14504. doi: 10.1039/C5CC04365D
|
| [149] | Stoddart JF (ed) (2001) Special issue on molecular machines. Acc Chem Res 34: 410 (2001). |
| [150] |
Cavallini M, Biscarini F, Leon S (2003) Information Storage Using Supramolecular Surface Patterns.Science 299: 531–531. doi: 10.1126/science.1078012
|
| [151] | Bottari G, Leigh DA, Pérez EM (2003) Chiroptical Switching in a Bistable Molecular Shuttle. J Am Chem.Soc125: 13360–13361. |
| [152] |
Pernites RB, Santos CM, Maldonado M, et al. (2012) Tunable Protein and Bacterial Cell Adsorption on Colloidally Templated Superhydrophobic Polythiophene Films. Chem Mater 24: 870–880. doi: 10.1021/cm2007044
|
| [153] | Gomez N, Schmidt CE (2007) Nerve growth factor-immobilized polypyrrole: Bioactive electrically conducting polymer for enhanced neurite extension. J Biomed Mater Res 81: 135–149. |
| [154] |
Green RA, Lovell NH, Poole-Warren LA (2009) Cell attachment functionality of bioactive conducting polymers for neural interfaces. Biomaterials 30: 3637–3644. doi: 10.1016/j.biomaterials.2009.03.043
|
| [155] | Zhong Y, Yu X, Gilbert R, et al (2001) Stabilizing electrode-host interfaces: a tissue engineering approach. J Rehabil Res Dev 38: 627–632. |
| [156] |
Fabregat G, Ballano G, Armelin E (2013) An electroactive and biologically responsive hybrid conjugate based on chemical similarity. Polym Chem 4: 1412–1424. doi: 10.1039/C2PY20894F
|
| [157] |
Maione S, Gil AM, Fabregat G, et al. (2015) Electroactive polymer–peptide conjugates for adhesive biointerfaces. Biomater Sci 3: 1395–1405. doi: 10.1039/C5BM00160A
|
| [158] |
Jeon G, Yang SY, Byun J, et al. (2011) Electrically actuatable smart nanoporous membrane for pulsatile drug release. Nano Lett 11: 1284–1288. doi: 10.1021/nl104329y
|
| [159] |
Ge J, Neofytou E, Cahill TJ, et al. (2012) Drug release from electric-field-responsive nanoparticles. ACS Nano 6: 227–233. doi: 10.1021/nn203430m
|
| [160] |
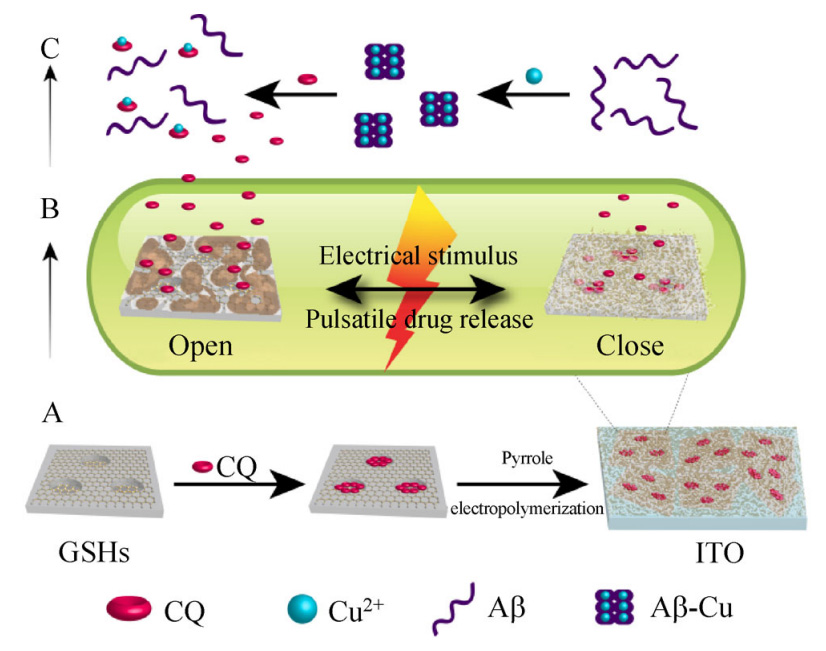
Wu L, Wang J, Gao N, et al. (2015) Electrically pulsatile responsive drug delivery platform for treatment of Alzheimer’s disease. Nano Res 8: 2400–2414. doi: 10.1007/s12274-015-0750-x
|
| [161] | Santos JL, Li Y, Culver HR, et al. (2014) Conducting polymer nanoparticles decorated with collagen mimetic peptides for collagen targeting. Chem Commun 50: 15045–15048. |
| [162] |
Cheng R, Meng F, Deng C, et al. (2013) Dual and multi-stimuli responsive polymeric nanoparticles for programmed site-specific drug delivery. Biomaterials 34: 3647–3657. doi: 10.1016/j.biomaterials.2013.01.084
|
| [163] |
Dai J, Lin SD, Cheng D, et al. (2011) Interlayer-crosslinked micelle with partially hydrated core showing reduction and pH dual sensitivity for pinpointed intracellular drug release. Angew Chem Int Ed 50: 9404–9408. doi: 10.1002/anie.201103806
|
| [164] |
Yu S, Wu G, Gu X, et al. (2013) Magnetic and pH-sensitive nanoparticles for antitumor drug deliver. Colloids Surf B 103: 15–22. doi: 10.1016/j.colsurfb.2012.10.041
|
| [165] | Remant BKC, Thapa B, Xu P (2012) pH and Redox Dual Responsive Nanoparticle for Nuclear Targeted Drug Delivery. Mol Pharmaceutics 9: 2719–2729. |
| [166] |
Gupta MK, Lee SH, Crowder SW, et al. (2015) Oligoproline-derived nanocarrier for dual stimuli-responsive gene delivery. J Mater Chem 3: 7271–7280. doi: 10.1039/C5TB00988J
|

Figures(19)

Lourdes Franco, Luís J. del Valle, Jordi Puiggalí. Smart systems related to polypeptide sequences[J]. AIMS Materials Science, 2016, 3(1): 289-323. doi: 10.3934/matersci.2016.1.289







 DownLoad:
DownLoad: