Grewia asiatica, commonly known as phalsa, is a widely cultivated fruit in Pakistan, valued for its nutritional and medicinal benefits. Being a perishable fruit with limited shelf life and rapid spoilage, a preservation approach is needed to extend fruit shelf life and product development. In this context, we aimed to extend the shelf life of G. asiatica fruit pulp using conventional and lyophilization drying and to evaluate their impact on nutritional composition, phytochemicals attributes, sensory evaluation and product shelf life for fruit pulp powder stored at ambient conditions for 3 months (0, 45th and 90th day). For the study, ripe G. asiatica fruit sourced from local farms were subjected to cleaning followed by drying using conventional and lyophilization processes. The resulting fruit powder was packed in sealed foil bags and stored at room temperature for 3 months, subjected to nutritional properties, phytochemicals, antioxidant capacity, and sensory evaluation on the 0, 45th, and 90th storage days. The results showed that both techniques increased the shelf life of powder. However, lyophilization resulted in better retention of vitamin C, antioxidant activity, and better free radical scavenging activity in fruit powder than conventional drying. Color parameters and sensory evaluation were also affected by drying and storage conditions as an advancement of storage resulted in decreased consumer acceptability. These findings demonstrate that lyophilization effectively preserves nutritional and phytochemical qualities of G. asiatica powder, making it a viable preservation approach for prolonging fruit shelf life while maintaining its health promoting compounds and functional properties. The lyophilized G. asiatica fruit pulp powder may have potential use in the food industry as an additive in ready-to-use products to enhance nutritional attributes, color, and better consumer acceptability for dried powders.
Citation: Saima Latif, Muhammad Sohaib, Sanaullah Iqbal, Muhammad Hassan Mushtaq, Muhammad Tauseef Sultan. Comparative evaluation of nutritional composition, phytochemicals and sensorial attributes of lyophilized vs conventionally dried Grewia asiatica fruit pulp powder[J]. AIMS Agriculture and Food, 2025, 10(1): 247-265. doi: 10.3934/agrfood.2025013
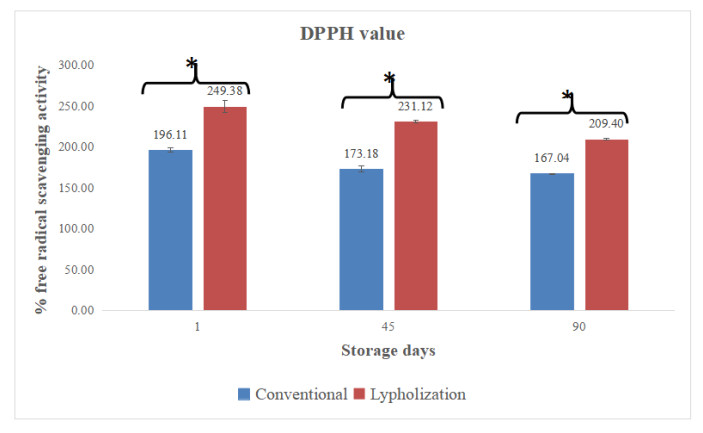
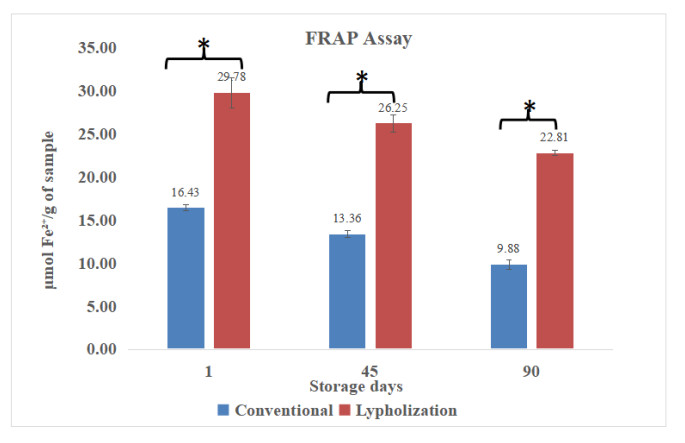
Grewia asiatica, commonly known as phalsa, is a widely cultivated fruit in Pakistan, valued for its nutritional and medicinal benefits. Being a perishable fruit with limited shelf life and rapid spoilage, a preservation approach is needed to extend fruit shelf life and product development. In this context, we aimed to extend the shelf life of G. asiatica fruit pulp using conventional and lyophilization drying and to evaluate their impact on nutritional composition, phytochemicals attributes, sensory evaluation and product shelf life for fruit pulp powder stored at ambient conditions for 3 months (0, 45th and 90th day). For the study, ripe G. asiatica fruit sourced from local farms were subjected to cleaning followed by drying using conventional and lyophilization processes. The resulting fruit powder was packed in sealed foil bags and stored at room temperature for 3 months, subjected to nutritional properties, phytochemicals, antioxidant capacity, and sensory evaluation on the 0, 45th, and 90th storage days. The results showed that both techniques increased the shelf life of powder. However, lyophilization resulted in better retention of vitamin C, antioxidant activity, and better free radical scavenging activity in fruit powder than conventional drying. Color parameters and sensory evaluation were also affected by drying and storage conditions as an advancement of storage resulted in decreased consumer acceptability. These findings demonstrate that lyophilization effectively preserves nutritional and phytochemical qualities of G. asiatica powder, making it a viable preservation approach for prolonging fruit shelf life while maintaining its health promoting compounds and functional properties. The lyophilized G. asiatica fruit pulp powder may have potential use in the food industry as an additive in ready-to-use products to enhance nutritional attributes, color, and better consumer acceptability for dried powders.

| [1] |
Zia-Ul-Haq M, Stanković MS, Rizwan K, et al. (2015) Compositional study and antioxidant capacity of Grewia asiatica L. seeds grown in Pakistan. Molecules 18: 2663–2676. https://doi.org/10.3390/molecules18032663 doi: 10.3390/molecules18032663

|
| [2] |
Khan RS, Asghar W, Khalid N, et al. (2019) Phalsa (Grewia asiatica L) fruit berry a promising functional food ingredient: A comprehensive review. J Berry Res 9: 179–193. https://doi.org/10.3233/JBR-180332 doi: 10.3233/JBR-180332
|
| [3] |
Barkaoui S, Madureira J, Mihoubi Boudhrioua N, et al. (2023) Berries: effects on health, preservation methods, and uses in functional foods: A review. Eur Food Res Technol 249: 1–27. https://doi.org/10.1007/s00217-023-04257-2 doi: 10.1007/s00217-023-04257-2
|
| [4] |
Ahmad K, Afridi M, Khan N, et al. (2021) Quality deterioration of postharvest fruits and vegetables in developing country Pakistan: A mini overview. Asian J Agric Food Sci 9: 83–90. http://dx.doi.org/10.24203/ajafs.v9i2.6615 doi: 10.24203/ajafs.v9i2.6615
|
| [5] |
Kaur S, Shams R, Dash KK, et al. (2024) Phytochemical and pharmacological characteristics of phalsa (Grewia asiatica L.): A comprehensive review. Heliyon 10: e25046. https://doi.org/10.1016/j.heliyon.2024.e25046 doi: 10.1016/j.heliyon.2024.e25046
|
| [6] | Bekić Šarić B (2022) Processing of agricultural products by lyophilization. http://repository.iep.bg.ac.rs/602/1/1.%20%C5%A0ari%C4%87%20Beki%C4%87.pdf |
| [7] |
Knorr D, Augustin MA, Smetanska I, et al. (2023) Preserving the food preservation legacy. Crit Rev Food Sci Nutr 63: 9519–9538. http://doi.org/10.1080/10408398.2022.2065459 doi: 10.1080/10408398.2022.2065459
|
| [8] | Prakash V, Ahirwar CS, Prashad V (2014) Studies on preparation and preservation of beverages from Phalsa fruit (Grewia subinaequalis L.). Ann Hortic 7: 92–96. |
| [9] |
Irigoytia MB, Irigoytia K, Sosa N, et al. (2022) Blueberry byproduct as a novel food ingredient: Physicochemical characterization and study of its application in a bakery product. J Sci Food Agric 102: 455. https://doi.org/10.1002/jsfa.11812 doi: 10.1002/jsfa.11812
|
| [10] |
Koley TK, Khan Z, Oulkar D, et al. (2020) Profiling of polyphenols in phalsa (Grewia asiatica L.) fruits based on liquid chromatography high-resolution mass spectrometry. J Food Sci Technol 57: 606–616. https://doi.org/10.1007/s13197-019-04092-y doi: 10.1007/s13197-019-04092-y
|
| [11] |
Khanal DP, Raut B, Kafle M, et al. (2016) A comparative study on phytochemical and biological activities of two Grewia species. J Manmohan Memorial Inst Health Sci 2: 53–60. https://doi.org/10.3126/jmmihs.v2i0.15797 doi: 10.3126/jmmihs.v2i0.15797
|
| [12] |
Xiao J, Li S, Sui Y, et al. (2015) In vitro antioxidant activities of proanthocyanidins extracted from the lotus seedpod and ameliorative effects on learning and memory impairment in scopolamine-induced amnesia mice. J Food Sci 24: 1487–1494. https://doi.org/10.1007/s10068-015-0192-y doi: 10.1007/s10068-015-0192-y
|
| [13] | AOAC International, Latimer GW (2016) Official Methods of Analysis of AOAC International. 20th ed., AOAC International. |
| [14] | Trejo-Téllez LI, Gómez-Merino FC (2014) Nutrient management in strawberry: Effects on yield, quality, and plant health. In: Malone N (Ed.), Strawberries: Cultivation, antioxidant properties and health benefits, 239–267. |
| [15] | Igwemmar NC, Kolawole SA, Imran I (2013) Effect of heating on vitamin C content of some selected vegetables. Int J Sci Technol Res 2: 209–212. |
| [16] |
Tzanova MT, Stoilova TD, Todorova MH, et al. (2023) Antioxidant potentials of different genotypes of cowpea (Vigna unguiculata L. Walp.) cultivated in Bulgaria, Southern Europe. Agronomy 13: 1684. http://dx.doi.org/10.3390/agronomy13071684 doi: 10.3390/agronomy13071684
|
| [17] |
Nicoue EE, Savard S, Belkacemi K, et al. (2007) Anthocyanins in wild blueberries of Quebec: Extraction and identification. J Agric Food Chem 55: 5626–5635. https://doi.org/10.1021/jf0703304 doi: 10.1021/jf0703304
|
| [18] |
Bochnak-Niedźwiecka J, Świeca M, Szymańska G, et al. (2020) Quality of new functional powdered beverages enriched with lyophilized fruits—Potentially bioaccessible antioxidant properties, nutritional value, and consumer analysis. Appl Sci 10: 3668. https://doi.org/10.3390/app10113668 doi: 10.3390/app10113668
|
| [19] |
Zorzi M, Gai F, Medana C, et al. (2020) Bioactive compounds and antioxidant capacity of small berries. Foods 9: 623. https://doi.org/10.3390/foods9050623 doi: 10.3390/foods9050623
|
| [20] |
Katekhong W, Wongphan P, Klinmalai P, et al. (2022) Thermoplastic starch blown films functionalized by plasticized nitrite blended with PBAT for superior oxygen barrier and active biodegradable meat packaging. Food Chem 374: 131709. https://doi.org/10.1016/j.foodchem.2021.131709 doi: 10.1016/j.foodchem.2021.131709
|
| [21] |
Agulheiro‐Santos AC, Ricardo‐Rodrigues S, Laranjo M, et al. (2022) Non‐destructive prediction of total soluble solids in strawberry using near infrared spectroscopy. J Food Sci 102: 4866–4872. https://doi.org/10.1002/jsfa.11849 doi: 10.1002/jsfa.11849
|
| [22] |
Bochnak-Niedźwiecka J, Świeca M, Gawlik-Dziki U, et al. (2020) Quality of new functional powdered beverages enriched with lyophilized fruits—Potentially bioaccessible antioxidant properties, nutritional value, and consumer analysis. Appl Sci 10: 3668. https://doi.org/10.3390/app10113668 doi: 10.3390/app10113668
|
| [23] |
Qamar M, Akhtar S, Ismail T, et al. (2020) Anticancer and anti-inflammatory perspectives of Pakistan's indigenous berry Grewia asiatica Linn (Phalsa). J Berry Res 10: 115–131. https://doi.org/10.3233/JBR-190459 doi: 10.3233/JBR-190459
|
| [24] |
Dalmau E, Araya-Farias M, Ratti C, et al. (2024) Cryogenic pretreatment enhances drying rates in whole berries. Foods 13: 1524. https://doi.org/10.3390/foods13101524 doi: 10.3390/foods13101524
|
| [25] |
Detoni E, Kalschne DL, Bendendo A, et al. (2021) Guabijú (Myrcianthes pungens): Characterization of in natura and lyophilized Brazilian berry. Res Soc Dev 10: e37810313337. https://doi.org/10.33448/rsd-v10i3.13337 doi: 10.33448/rsd-v10i3.13337
|
| [26] |
Bala K, Barmanray AJ, et al. (2019) Bioactive compounds, vitamins, and minerals composition of freeze-dried Grewia asiatica L. (Phalsa) pulp and seed powder. Food Res 38: 237–241. http://doi.org/10.18805/ag.DR-1474 doi: 10.18805/ag.DR-1474
|
| [27] |
Nemzer B, Vargas L, Xia X, et al. (2018) Phytochemical and physical properties of blueberries, tart cherries, strawberries, and cranberries as affected by different drying methods. Food Chem 262: 242–250. https://doi.org/10.1016/j.foodchem.2018.04.047 doi: 10.1016/j.foodchem.2018.04.047
|
| [28] |
Samoticha J, Wojdyło A, Lech K, et al. (2016) The influence of different drying methods on chemical composition and antioxidant activity in chokeberries. LWT-Food Sci Technol 66: 484–489. https://doi.org/10.1016/j.lwt.2015.10.073 doi: 10.1016/j.lwt.2015.10.073
|
| [29] |
Reyes A, Bubnovich V, Bustos R, et al. (2010) Comparative study of different process conditions of freeze drying of 'Murtilla' berry. Dry Technol 28: 1416–1425. https://doi.org/10.1080/07373937.2010.482687 doi: 10.1080/07373937.2010.482687
|
| [30] |
Kamanova S, Temirova I, Aldiyeva A, et al. (2023) Effects of freeze-drying on sensory characteristics and nutrient composition in black currant and sea buckthorn berries. Appl Sci 13: 12709. https://doi.org/10.3390/app132312709 doi: 10.3390/app132312709
|
| [31] |
Bustos Shmidt MC, Rocha Parra DF, Sampedro I, et al. (2018) The influence of different air-drying conditions on bioactive compounds and antioxidant activity of berries. J Agric Food Chem 66: 2714–2723. https://doi.org/10.1021/acs.jafc.7b05395 doi: 10.1021/acs.jafc.7b05395
|
| [32] |
Shishehgarha F, Makhlouf J, Ratti C, et al. (2002) Freeze-drying characteristics of strawberries. Dry Technol 20: 131–145. https://doi.org/10.1081/DRT-120001370 doi: 10.1081/DRT-120001370
|
| [33] |
Sette P, Franceschinis L, Schebor C, et al. (2017) Fruit snacks from raspberries: Influence of drying parameters on colour degradation and bioactive potential. Int J Food Sci Technol 52: 313–328. http://dx.doi.org/10.1111/ijfs.13283 doi: 10.1111/ijfs.13283
|
| [34] |
Ajayi MG, Lajide L, Amoo IA, et al. (2023) Proximate, mineral and antioxidant activity of wonderful kola (Buchholzia coriacea) seed (fresh and freeze-dried). GSC Biol Pharm Sci 22: 261–271. https://doi.org/10.30574/gscbps.2023.22.2.0074 doi: 10.30574/gscbps.2023.22.2.0074
|
| [35] |
Souza DS, Marques LG, Gomes EdB, et al. (2015) Lyophilization of avocado (Persea americana Mill.): Effect of freezing and lyophilization pressure on antioxidant activity, texture, and browning of pulp. Dry Technol 33: 194–204. https://doi.org/10.1080/07373937.2014.943766 doi: 10.1080/07373937.2014.943766
|
| [36] |
Hammami C, René F, et al. (1997) Determination of freeze-drying process variables for strawberries. J Food Eng 32: 133–154. https://doi.org/10.1016/S0260-8774(97)00023-X doi: 10.1016/S0260-8774(97)00023-X
|
Figures(2) / Tables(6)

Saima Latif, Muhammad Sohaib, Sanaullah Iqbal, Muhammad Hassan Mushtaq, Muhammad Tauseef Sultan. Comparative evaluation of nutritional composition, phytochemicals and sensorial attributes of lyophilized vs conventionally dried Grewia asiatica fruit pulp powder[J]. AIMS Agriculture and Food, 2025, 10(1): 247-265. doi: 10.3934/agrfood.2025013







 DownLoad:
DownLoad: