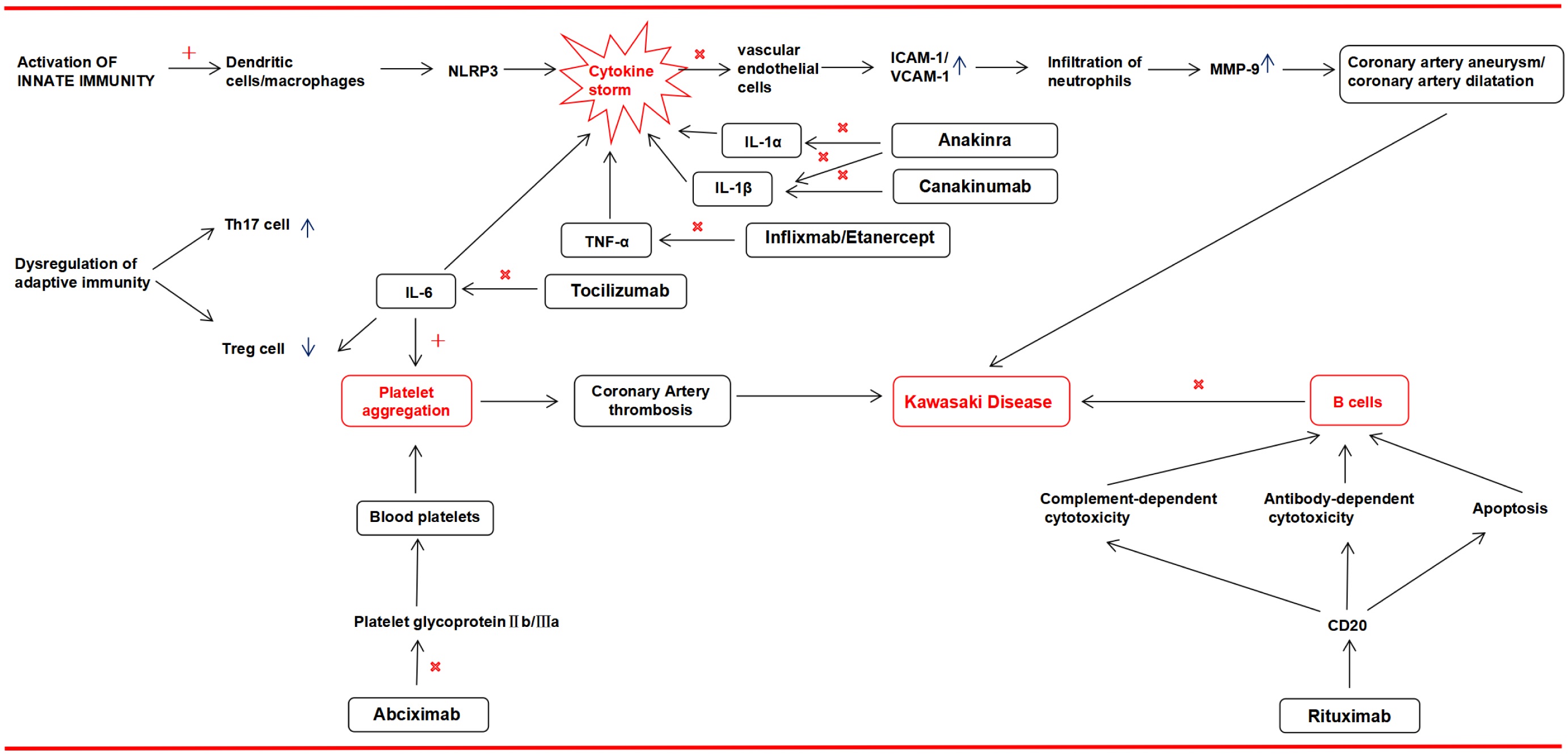
Kawasaki disease (KD), also known as mucocutaneous lymph node syndrome, is an acute febrile systemic vasculitis predominantly affecting children under the age of 5 years. The hallmark of KD is systemic vasculitis, which can lead to coronary artery complications if not promptly treated. Approximately 15%–20% of untreated cases develop coronary artery aneurysms, coronary artery stenosis, or thrombosis, posing significant risks to pediatric health and survival. In recent years, the incidence of KD has shown an upward trend. While intravenous immunoglobulin in combination with aspirin remains the standard first-line therapy for acute KD, some patients exhibit resistance to intravenous immunoglobulin or progress to refractory KD. The rapid advancement of modern biomedicine has led to increased interest in biological agents for KD treatment, yielding promising outcomes.
Citation: Qi-Ling Yin, You-Qiong Liu, Hui-Min Zhang, Wei-Hua Zhang. Clinical advancements of biologic agents in the treatment of Kawasaki disease based on its pathogenesis[J]. AIMS Allergy and Immunology, 2025, 9(2): 108-122. doi: 10.3934/Allergy.2025008
Kawasaki disease (KD), also known as mucocutaneous lymph node syndrome, is an acute febrile systemic vasculitis predominantly affecting children under the age of 5 years. The hallmark of KD is systemic vasculitis, which can lead to coronary artery complications if not promptly treated. Approximately 15%–20% of untreated cases develop coronary artery aneurysms, coronary artery stenosis, or thrombosis, posing significant risks to pediatric health and survival. In recent years, the incidence of KD has shown an upward trend. While intravenous immunoglobulin in combination with aspirin remains the standard first-line therapy for acute KD, some patients exhibit resistance to intravenous immunoglobulin or progress to refractory KD. The rapid advancement of modern biomedicine has led to increased interest in biological agents for KD treatment, yielding promising outcomes.

| [1] |
Miyata K, Miura M, Kaneko T, et al. (2021) Risk factors of coronary artery abnormalities and resistance to intravenous immunoglobulin plus corticosteroid therapy in severe Kawasaki disease: An analysis of post RAISE. Circ Cardiovasc Qual Outcomes 14: e007191. https://doi.org/10.1161/CIRCOUTCOMES.120.007191 
|
| [2] |
Lei WT, Chang LS, Zeng BY, et al. (2022) Pharmacologic interventions for Kawasaki disease in children: A network meta-analysis of 56 randomized controlled trials. EBioMedicine 78: 103946. https://doi.org/10.1016/j.ebiom.2022.103946
|
| [3] |
Kibata T, Suzuki Y, Hasegawa S, et al. (2016) Coronary artery lesions and the increasing incidence of Kawasaki disease resistant to initial immunoglobulin. Int J Cardiol 214: 209-215. https://doi.org/10.1016/j.ijcard.2016.03.017
|
| [4] |
Ohnishi Y, Okada S, Kawakami-Miyake A, et al. (2022) Safety and feasibility of infliximab therapy in children with Kawasaki disease who received live vaccinations. Pediatr Infect Dis J 41: e388-e392. https://doi.org/10.1097/INF.0000000000003611
|
| [5] |
Tang B, Lo HH, Lei C, et al. (2020) Adjuvant herbal therapy for targeting susceptibility genes to Kawasaki disease: An overview of epidemiology, pathogenesis, diagnosis and pharmacological treatment of Kawasaki disease. Phytomedicine 70: 153208. https://doi.org/10.1016/j.phymed.2020.153208
|
| [6] |
Chang L, Yang HW, Lin TY, et al. (2021) Perspective of immunopathogenesis and immunotherapies for Kawasaki disease. Front Pediatr 9: 697632. https://doi.org/10.3389/fped.2021.697632
|
| [7] |
Kumrah R, Vignesh P, Rawat A, et al. (2020) Immunogenetics of Kawasaki disease. Clin Rev Allergy Immunol 59: 122-139. https://doi.org/10.1007/s12016-020-08783-9
|
| [8] |
Paolini L, Guida F, Calvaruso A, et al. (2024) Endothelial dysfunction: Molecular mechanisms and therapeutic strategies in Kawasaki disease. Int J Mol Sci 25: 13322. https://doi.org/10.3390/ijms252413322
|
| [9] |
Rife E, Gedalia A (2020) Kawasaki disease: An update. Curr Rheumatol Rep 22: 75. https://doi.org/10.1007/s11926-020-00941-4
|
| [10] |
Wang W, Zhu L, Li X, et al. (2023) Emerging evidence of microbial infection in causing systematic immune vasculitis in Kawasaki disease. Front Microbiol 14: 1313838. https://doi.org/10.3389/fmicb.2023.1313838
|
| [11] |
Chang LY, Lu CY, Shao PL, et al. (2014) Viral infections associated with Kawasaki disease. J Formos Med Assoc 113: 148-154. https://doi.org/10.1016/j.jfma.2013.12.008
|
| [12] |
McCrindle BW, Rowley AH, Newburger JW, et al. (2017) Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American Heart Association. Circulation 135: e927-e999. https://doi.org/10.1161/CIR.0000000000000484
|
| [13] |
Bordea MA, Costache C, Grama A, et al. (2022) Cytokine cascade in Kawasaki disease versus Kawasaki-like syndrome. Physiol Res 71: 17-27. https://doi.org/10.33549/physiolres.934672
|
| [14] | Zhang H, Song HB, Wang DX, et al. (2022) Correlation between the level of inflammatory cytokines and prognosis in children with IVIG-sensitive Kawasaki disease and IVIG-resistant Kawasaki disease. Pak J Med Sci 38: 1165-1169. https://doi.org/10.12669/pjms.38.5.5408 |
| [15] | Jone PN, Tremoulet A, Choueiter N, et al. (2024) Update on diagnosis and management of Kawasaki disease: A scientific statement from the American Heart Association. Circulation 150: e481-e500. https://doi.org/10.1161/CIR.0000000000001295 |
| [16] | Yamaji N, da Silva Lopes K, Shoda T, et al. (2019) TNF-α blockers for the treatment of Kawasaki disease in children. Cochrane Database Syst Rev 8: CD012448. https://doi.org/10.1002/14651858.CD012448.pub2 |
| [17] |
Li D, Li X, Dou W, et al. (2021) The effectiveness of infliximab for Kawasaki disease in children: Systematic review and meta-analysis. Transl Pediatr 10: 1294-1306. https://doi.org/10.21037/tp-20-482
|
| [18] |
Chen J, Liao J, Xiang L, et al. (2023) Current knowledge of TNF-α monoclonal antibody infliximab in treating Kawasaki disease: A comprehensive review. Front Immunol 14: 1237670. https://doi.org/10.3389/fimmu.2023.1237670
|
| [19] |
Portman MA, Olson A, Soriano B, et al. (2011) Etanercept as adjunctive treatment for acute Kawasaki disease: Study design and rationale. Am Heart J 161: 494-499. https://doi.org/10.1016/j.ahj.2010.12.003
|
| [20] |
Kabbaha S, Milano A, Aldeyab MA, et al. (2023) Infliximab as a second-line therapy for children with refractory Kawasaki disease: A systematic review and meta-analysis of randomized controlled trials. Br J Clin Pharmacol 89: 49-60. https://doi.org/10.1111/bcp.15547
|
| [21] |
Koizumi K, Hoshiai M, Katsumata N, et al. (2018) Infliximab regulates monocytes and regulatory T cells in Kawasaki disease. Pediatr Int 60: 796-802. https://doi.org/10.1111/ped.13555
|
| [22] |
Ishii M, Ebato T, Kato H (2020) History and future of treatment for acute stage Kawasaki disease. Korean Circ J 50: 112-119. https://doi.org/10.4070/kcj.2019.0290
|
| [23] |
Hur G, Song MS, Sohn S, et al. (2019) Infliximab treatment for intravenous immunoglobulin-resistant Kawasaki disease: A multicenter study in Korea. Korean Circ J 49: 183-191. https://doi.org/10.4070/kcj.2018.0214
|
| [24] |
Li X, Tang Y, Ding Y, et al. (2021) Higher efficacy of infliximab than immunoglobulin on Kawasaki disease, a meta-analysis. Eur J Pharmacol 899: 173985. https://doi.org/10.1016/j.ejphar.2021.173985
|
| [25] |
Portman MA, Dahdah NS, Slee A, et al. (2019) Etanercept with IVIG for acute Kawasaki disease: A randomized controlled trial. Pediatrics 143: e20183675. https://doi.org/10.1542/peds.2018-3675
|
| [26] | Ohashi R, Fukazawa R, Watanabe M, et al. (2013) Etanercept suppresses arteritis in a murine model of kawasaki disease: A comparative study involving different biological agents. Int J Vasc Med 2013: 543141. https://doi.org/10.1155/2013/543141 |
| [27] |
Sagiv E, Slee A, Buffone A, et al. (2023) Etanercept with IVIG for acute Kawasaki disease: A long-term follow-up on the EATAK trial. Cardiol Young 33: 613-618. https://doi.org/10.1017/S1047951122001470
|
| [28] |
Tremoulet AH (2018) Adjunctive therapies in Kawasaki disease. Int J Rheum Dis 21: 76-79. https://doi.org/10.1111/1756-185X.13208
|
| [29] |
Lee Y, Wakita D, Dagvadorj J, et al. (2015) IL-1 signaling is critically required in stromal cells in Kawasaki disease vasculitis mouse model: Role of both IL-1α and IL-1β. Arterioscler Thromb Vasc Biol 35: 2605-2616. https://doi.org/10.1161/ATVBAHA.115.306475
|
| [30] |
Cavalli G, Colafrancesco S, Emmi G, et al. (2021) Interleukin 1α: A comprehensive review on the role of IL-1α in the pathogenesis and treatment of autoimmune and inflammatory diseases. Autoimmun Rev 20: 102763. https://doi.org/10.1016/j.autrev.2021.102763
|
| [31] |
Maniscalco V, Abu-Rumeileh S, Mastrolia MV, et al. (2020) The off-label use of anakinra in pediatric systemic autoinflammatory diseases. Ther Adv Musculoskelet Dis 12: 1759720X20959575. https://doi.org/10.1177/1759720X20959575
|
| [32] |
Mastrolia MV, Abbati G, Signorino C, et al. (2021) Early anti IL-1 treatment replaces steroids in refractory Kawasaki disease: Clinical experience from two case reports. Ther Adv Musculoskelet Dis 13: 1759720X211002593. https://doi.org/10.1177/1759720X211002593
|
| [33] |
De Rose DU, Campi F, Maddaloni C, et al. (2025) Off-label use of anakinra in inflammatory conditions in neonates and infants up to 3 months of age: A case series and a review of the literature. Paediatr Drugs 27: 293-305. https://doi.org/10.1007/s40272-024-00679-x
|
| [34] |
Bossi G, Codazzi AC, Vinci F, et al. (2022) Efficacy of anakinra on multiple coronary arteries aneurysms in an infant with recurrent Kawasaki disease, complicated by macrophage activation syndrome. Children 9: 672. https://doi.org/10.3390/children9050672
|
| [35] |
Ferrara G, Giani T, Caparello MC, et al. (2020) Anakinra for treatment-resistant Kawasaki disease: Evidence from a literature review. Paediatr Drugs 22: 645-652. https://doi.org/10.1007/s40272-020-00421-3
|
| [36] |
Malcova H, Milota T, Strizova Z, et al. (2021) Interleukin-1 blockade in polygenic autoinflammatory disorders: Where are we now?. Front Pharmacol 11: 619273. https://doi.org/10.3389/fphar.2020.619273
|
| [37] |
Yang J, Jain S, Capparelli EV, et al. (2021) Anakinra treatment in patients with acute Kawasaki disease with coronary artery aneurysms: A phase I/IIa trial. J Pediatr 243: 173-180.e8. https://doi.org/10.1016/j.jpeds.2021.12.035
|
| [38] |
Lind-Holst M, Hartling UB, Christensen AE (2019) High-dose anakinra as treatment for macrophage activation syndrome caused by refractory Kawasaki disease in an infant. BMJ Case Rep 12: e229708. https://doi.org/10.1136/bcr-2019-229708
|
| [39] |
Shafferman A, Birmingham JD, Cron RQ (2014) High dose anakinra for treatment of severe neonatal Kawasaki disease: A case report. Pediatr Rheumatol Online J 12: 26. https://doi.org/10.1186/1546-0096-12-26
|
| [40] |
Gambacorta A, Buonsenso D, De Rosa G, et al. (2020) Resolution of giant coronary aneurisms in a child with refractory Kawasaki disease treated with anakinra. Front Pediatr 8: 195. https://doi.org/10.3389/fped.2020.00195
|
| [41] |
Sánchez-Manubens J, Gelman A, Franch N, et al. (2017) A child with resistant Kawasaki disease successfully treated with anakinra: A case report. BMC Pediatr 17: 102. https://doi.org/10.1186/s12887-017-0852-6
|
| [42] |
Burns JC, Koné-Paut I, Kuijpers T, et al. (2017) Review: Found in translation: International initiatives pursuing interleukin-1 blockade for treatment of acute Kawasaki disease. Arthritis Rheumatol 69: 268-276. https://doi.org/10.1002/art.39975
|
| [43] |
Martins FR, Azevedo AC, Ganhão S, et al. (2023) Anakinra and hepatotoxicity in pediatric rheumatology: A case series. Pediatr Rheumatol Online J 21: 112. https://doi.org/10.1186/s12969-023-00891-y
|
| [44] |
Malcova H, Strizova Z, Milota T, et al. (2021) IL-1 Inhibitors in the treatment of monogenic periodic fever syndromes: From the past to the future perspectives. Front Immunol 11: 619257. https://doi.org/10.3389/fimmu.2020.619257
|
| [45] |
Renner C (2019) 20 years of rituximab treatment: What have we learnt?. Future Oncol 15: 4119-4121. https://doi.org/10.2217/fon-2019-0694
|
| [46] |
Lucchini E, Zaja F, Bussel J (2019) Rituximab in the treatment of immune thrombocytopenia: What is the role of this agent in 2019?. Haematologica 104: 1124-1135. https://doi.org/10.3324/haematol.2019.218883
|
| [47] |
Sauvaget E, Bonello B, David M, et al. (2012) Resistant Kawasaki disease treated with anti-CD20. J Pediatr 160: 875-876. https://doi.org/10.1016/j.jpeds.2012.01.018
|
| [48] |
Tacke CE, Burgner D, Kuipers IM, et al. (2012) Management of acute and refractory Kawasaki disease. Expert Rev Anti Infect Ther 10: 1203-1215. https://doi.org/10.1586/eri.12.101
|
| [49] |
Wu Y, Liu FF, Xu Y, et al. (2019) Interleukin-6 is prone to be a candidate biomarker for predicting incomplete and IVIG nonresponsive Kawasaki disease rather than coronary artery aneurysm. Clin Exp Med 19: 173-181. https://doi.org/10.1007/s10238-018-00544-5
|
| [50] |
Ling J, Xie F, Zhou Q, et al. (2024) Case series on the efficacy and safety of tocilizumab in IVIG-resistant Kawasaki disease: A retrospective analysis of five patients. J Inflamm Res 17: 10991-10998. https://doi.org/10.2147/JIR.S479879
|
| [51] | Cui HY, Hu CP (2022) Recent research on the application of biologics in the treatment of multisystem inflammatory syndrome in children after SARS-CoV-2 infection. Zhongguo Dang Dai Er Ke Za Zhi 24: 216-222. https://doi.org/10.7499/j.issn.1008-8830.2111005 |
| [52] |
Porritt RA, Chase Huizar C, Dick EJ, et al. (2021) Inhibition of IL-6 in the LCWE mouse model of Kawasaki disease Inhibits acute phase reactant serum amyloid a but fails to attenuate vasculitis. Front Immunol 12: 630196. https://doi.org/10.3389/fimmu.2021.630196
|
| [53] |
Barman P, Pilania RK, Cv G, et al. (2024) Treatment intensification in Kawasaki disease-current perspectives. Expert Rev Clin Immunol 20: 1179-1191. https://doi.org/10.1080/1744666X.2024.2378900
|
| [54] |
Nozawa T, Imagawa T, Ito S (2017) Coronary-artery aneurysm in tocilizumab-treated Children with Kawasaki's Disease. N Engl J Med 377: 1894-1896. https://doi.org/10.1056/NEJMc1709609
|
| [55] |
Bachlava E, Loukopoulou S, Karanasios E, et al. (2016) Management of coronary artery aneurysms using abciximab in children with Kawasaki disease. Int J Cardiol 220: 65-69. https://doi.org/10.1016/j.ijcard.2016.06.062
|
| [56] |
Jone PN, Tapia D, Davidson J, et al. (2015) Successful treatment of myocardial infarction in an infant with Kawasaki disease. Semin Cardiothorac Vasc Anesth 19: 255-259. https://doi.org/10.1177/1089253215573328
|
| [57] |
Garcia Verde MJ, Martinez Roca C, Yanez Gomez P, et al. (2016) Abciximab in refractory Kawasaki disease. Eur J Hosp Pharm 23: A33-A34. https://doi.org/10.1136/ejhpharm-2016-000875.76
|
Figures(1) / Tables(1)

Qi-Ling Yin, You-Qiong Liu, Hui-Min Zhang, Wei-Hua Zhang. Clinical advancements of biologic agents in the treatment of Kawasaki disease based on its pathogenesis[J]. AIMS Allergy and Immunology, 2025, 9(2): 108-122. doi: 10.3934/Allergy.2025008







 DownLoad:
DownLoad: