Although antiretroviral therapy is beneficial and available free of cost to patients, several roadblocks still prevent patients from reaching viral suppression. This research aimed to determine the prevalence rate of viral suppression among people living with HIV in the western region of Ghana and identify the factors contributing to viral non-suppression.
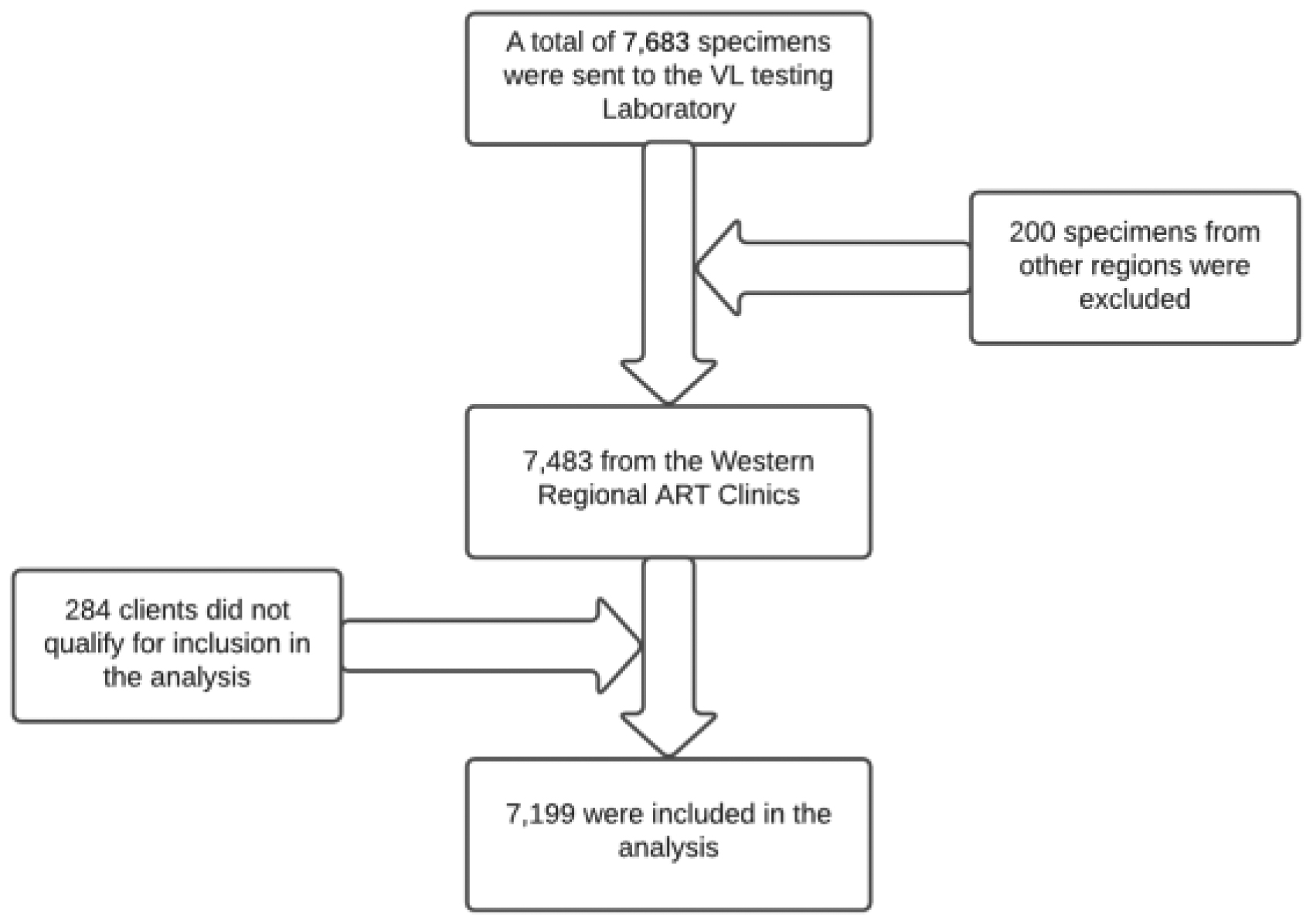
A cross-sectional study was conducted on 7199 HIV-positive adults. All data from the Sekondi Public Health Laboratory database was exported to Microsoft Excel and then verified and filtered before being exported to STATA 16.1. Viral non-suppression was modeled statistically using logistic regression.
Viral load suppression was achieved in 5465 (75.91%) study participants who received antiretroviral treatment. However, 1734 participants (24.0%) did not achieve viral suppression. Patients with poor adherence to ARV (AOR 0.30; 95% CI 0.16, 0.58) and fair adherence to ARV (AOR 0.23; 95% CI 0.12, 0.45) were associated with a lower odd of viral non-suppression. Patients with six (6) months to two (2) years of treatment before viral load testing (AOR 0.67; 95% CI 0.46, 0.98) were also associated with a lower likelihood of viral non-suppression.
The rate of non-suppression was high, and the suppression rate fell short of the UNAIDS target. Poor ARV adherence, fair ARV adherence, and a treatment duration of six (6) months to two (2) years before viral load testing appear to be obstacles to viral load suppression. The research findings seem to suggest that viral load testing supports viral non-suppression. Therefore, using viral load tests to monitor medication's effects on health can motivate patients to adhere to their prescribed medication regimen. More research is needed to determine whether viral load testing can improve adherence. Given the high rate of virologic failure, the study highlights the importance of identifying antiretroviral resistance patterns.
Citation: Philip Boakye, Adwoa Safowaa. Prevalence and predictors of viral load suppression in adults living with HIV in the western region of Ghana: A cross-sectional study[J]. AIMS Public Health, 2023, 10(2): 469-479. doi: 10.3934/publichealth.2023033
Although antiretroviral therapy is beneficial and available free of cost to patients, several roadblocks still prevent patients from reaching viral suppression. This research aimed to determine the prevalence rate of viral suppression among people living with HIV in the western region of Ghana and identify the factors contributing to viral non-suppression.
A cross-sectional study was conducted on 7199 HIV-positive adults. All data from the Sekondi Public Health Laboratory database was exported to Microsoft Excel and then verified and filtered before being exported to STATA 16.1. Viral non-suppression was modeled statistically using logistic regression.
Viral load suppression was achieved in 5465 (75.91%) study participants who received antiretroviral treatment. However, 1734 participants (24.0%) did not achieve viral suppression. Patients with poor adherence to ARV (AOR 0.30; 95% CI 0.16, 0.58) and fair adherence to ARV (AOR 0.23; 95% CI 0.12, 0.45) were associated with a lower odd of viral non-suppression. Patients with six (6) months to two (2) years of treatment before viral load testing (AOR 0.67; 95% CI 0.46, 0.98) were also associated with a lower likelihood of viral non-suppression.
The rate of non-suppression was high, and the suppression rate fell short of the UNAIDS target. Poor ARV adherence, fair ARV adherence, and a treatment duration of six (6) months to two (2) years before viral load testing appear to be obstacles to viral load suppression. The research findings seem to suggest that viral load testing supports viral non-suppression. Therefore, using viral load tests to monitor medication's effects on health can motivate patients to adhere to their prescribed medication regimen. More research is needed to determine whether viral load testing can improve adherence. Given the high rate of virologic failure, the study highlights the importance of identifying antiretroviral resistance patterns.

| [1] |
Degavi G (2021) Influence of Lost to Follow Up from Antiretroviral Therapy Among Retroviral Infected Patients at Tuberculosis Centers in Public Hospitals of Benishangul-Gumuz, Ethiopia. HIV AIDS Res Palliat Care 13: 315-327. https://doi.org/10.2147/HIV.S306257 
|
| [2] | Astuti DA, Dzakiyullah NRD, Yulyani L, et al. (2020) Factors Related to Hiv/Aids Knowledge of Eligible Women. Eur J Nucl Med Mol I 7: 57-69. |
| [3] | UNAIDSFact Sheet-World AIDS Day (2021). |
| [4] |
Chisumpa VH, Odimegwu CO, Saikia N (2019) Adult mortality in sub-Saharan Africa: cross-sectional study of causes of death in Zambia. Trop Med Int Health 24: 1208-1220. https://doi.org/10.1111/tmi.13302
|
| [5] |
Lokpo SY, Ofori-Attah PJ, Ameke LS, et al. (2020) Viral Suppression and Its Associated Factors in HIV Patients on Highly Active Antiretroviral Therapy (HAART): A Retrospective Study in the Ho Municipality, Ghana. Aids Res Treat 2020: 1-7.
|
| [6] | WHOConsolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach (2016). |
| [7] |
Tsegaw A, Abilo T, Lemma D, et al. (2019) Incidence and Predictors of First Line Anti-Retroviral Therapy Failure among Adults Receiving HIV Care in North West Ethiopia: A Hospital-Based Follow-Up Study. J Infect Dis Epidemiol 5: 345. https://doi.org/10.23937/2474-3658/1510072
|
| [8] |
Lailulo Y, Kitenge M, Jaffer S, et al. (2020) Factors associated with antiretroviral treatment failure among people living with HIV on antiretroviral therapy in resource-poor settings: a systematic review and metaanalysis. Syst Rev 9: 292. https://doi.org/10.1186/s13643-020-01524-1
|
| [9] |
Afrane AKA, Goka BQ, Renner L, et al. (2021) HIV virological non-suppression and its associated factors in children on antiretroviral therapy at a major treatment centre in Southern Ghana: a cross-sectional study. BMC Infect Dis 21: 731. https://doi.org/10.1186/s12879-021-06459-z
|
| [10] | UNAIDSUndetectable = Untransmissible, Public Health and HIV Viral Load Suppression (2018). |
| [11] | UNAIDS90–90–90 An ambitious treatment target to help end the AIDS epidemic (2017). |
| [12] | UNAIDSUNAIDS report on the global AIDS epidemic shows that 2020 targets will not be met because of deeply unequal success; COVID-19 risks blowing HIV progress way off course _ UNAIDS (2020). |
| [13] | NACP/GHSAnnual Report. National AIDS Control Programme/Ghana Health Service (2021). |
| [14] | NACP/GHSHIV Sentinel Survey Report. National AIDS Control Programme/Ghana Health Service (2021). |
| [15] |
Desta AA, Woldearegay TW, Futwi N, et al. (2020) HIV virological non-suppression and factors associated with non-suppression among adolescents and adults on antiretroviral therapy in northern Ethiopia: a retrospective study. BMC Infect Dis 20: 4. https://doi.org/10.1186/s12879-019-4732-6
|
| [16] |
Gunthard HF, Saag MS, Benson CA, et al. (2016) Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2016 Recommendations of the International Antiviral Society-USA Panel. JAMA 316: 191-210. https://doi.org/10.1001/jama.2016.8900
|
| [17] |
Hermans LE, Carmona S, Nijhuis M, et al. (2020) Virological suppression and clinical management in response to viremia in South African HIV treatment program: A multicenter cohort study. PLoS Med 17: e1003037.
|
| [18] | GACNational and Sub-National HIV and AIDS Estimates and Projections Report. Ghana AIDS Commission (2020). |
| [19] | AIDSinfo U Key HIV Indicators - AIDSinfo: GHANA (2021). |
| [20] | NACP/GHSNational AIDS Control Programme Annual Report. National AIDS Control Programme (2019). |
| [21] |
Ansah D, Kumah E, Bawontuo V, et al. (2021) Determinants of viral load non-suppression among people living with HIV on antiretroviral therapy in Kumasi, Ghana. Ghana Med J 55: 111-117. https://doi.org/10.4314/gmj.v55i2.3
|
| [22] | UNAIDSPrevailing against pandemics by putting people at the centre. World AIDS Day report (2020). |
| [23] |
Heath K, Levi J, Hill A (2021) The Joint United Nations Programme on HIV/AIDS 95–95–95 targets: worldwide clinical and cost benefits of generic manufacture. AIDS 35: S197-S203. https://doi.org/10.1097/QAD.0000000000002983
|
| [24] |
Frescura L, Godfrey-Faussett P, Feizzadeh AA, et al. (2022) Achieving the 95 95 95 targets for all: A pathway to ending AIDS. PLoS One 17: e0272405. https://doi.org/10.1371/journal.pone.0272405
|
| [25] |
Yotebieng M, Mpody C, Ravelomanana NL, et al. (2019) HIV viral suppression among pregnant and breastfeeding women in routine care in the Kinshasa province: a baseline evaluation of participants in CQI-PMTCT study. J Int AIDS Soc 22: e25376. https://doi.org/10.1002/jia2.25376
|
| [26] |
Abioye AI, Soipe AI, Salako AA, et al. (2015) Are there differences in disease progression and mortality among male and female HIV patients on antiretroviral therapy? A meta-analysis of observational cohorts. AIDS Care 27: 1468-1486. https://doi.org/10.1080/09540121.2015.1114994
|
| [27] |
Beckham SW, Beyrer C, Luckow P, et al. (2016) Marked sex differences in all-cause mortality on antiretroviral therapy in low- and middle-income countries: a systematic review and meta-analysis. J Int AIDS Soc 19: 21106. https://doi.org/10.7448/IAS.19.1.21106
|
| [28] |
Penot P, Hema A, Bado G, et al. (2014) The vulnerability of men to virologic failure during antiretroviral therapy in a public routine clinic in Burkina Faso. J Int AIDS Soc 17: 18646. https://doi.org/10.7448/IAS.17.1.18646
|
| [29] |
Datay MI, Boulle A, Mant D, et al. (2010) Associations with virologic treatment failure in adults on antiretroviral therapy in South Africa. J Acquir Immune Defic Syndr 54: 489-495. https://doi.org/10.1097/QAI.0b013e3181d91788
|
| [30] |
Cornell M, Schomaker M, Garone DB, et al. (2012) Gender differences in survival among adult patients starting antiretroviral therapy in South Africa: a multicentre cohort study. PLoS Med 9: e1001304. https://doi.org/10.1371/journal.pmed.1001304
|
| [31] |
De Beaudrap P, Thiam M, Diouf A, et al. (2013) Risk of virological failure and drug resistance during first and second-line antiretroviral therapy in a 10-year cohort in Senegal: results from the ANRS 1215 cohort. J Acquir Immune Defic Syndr 62: 381-387. https://doi.org/10.1097/QAI.0b013e31827a2a7a
|
| [32] |
Kiweewa F, Esber A, Musingye E, et al. (2019) HIV virologic failure and its predictors among HIV-infected adults on antiretroviral therapy in the African Cohort Study. PLoS One 14: e0211344. https://doi.org/10.1371/journal.pone.0211344
|
| [33] |
Bayu B, Tariku A, Bulti AB, et al. (2017) Determinants of virological failure among patients on highly active antiretroviral therapy in University of Gondar Referral Hospital, Northwest Ethiopia: a case-control study. HIV AIDS Res Palliat Care 9: 153-159. https://doi.org/10.2147/HIV.S139516
|
| [34] | Wakooko P, Gavamukulya Y, Wandabwa JN (2020) Viral load Suppression and Associated Factors among HIV Patients on Antiretroviral Treatment in Bulambuli District, Eastern Uganda: A Retrospective Cohort Study. Infect Dis: Res Treat 13: 1178633720970632. https://doi.org/10.1177/1178633720970632 |
| [35] |
Waju B, Dube L, Ahmed M, et al. (2021) Unsuppressed Viral Load Level in Public Health Facilities: Nonvirological Predictors among Adult Antiretroviral Therapy Users in Southwestern Ethiopia. HIV AIDS Res Palliat Care 13: 513-526. https://doi.org/10.2147/HIV.S304653
|
| [36] |
Desta AA, Woldearegay TW, Futwi N, et al. (2020) HIV virological non-suppression and factors associated with non-suppression among adolescents and adults on antiretroviral therapy in northern Ethiopia: a retrospective study. BMC Infect Dis 20. https://doi.org/10.1186/s12879-019-4732-6
|
| [37] |
Bulage L, Ssewanyana I, Nankabirwa V, et al. (2017) Factors Associated with Virological Non-suppression among HIV-Positive Patients on Antiretroviral Therapy in Uganda, August 2014-July 2015. BMC Infect Dis 17: 326. https://doi.org/10.1186/s12879-017-2428-3
|
| [38] |
Yager JL, Coyle RP, Coleman SS, et al. (2019) Moderately High Tenofovir Diphosphate in Dried Blood Spots Indicates Drug Resistance in Viremic Persons Living with HIV. J Int Assoc Provid AIDS Care 18: 2325958219888457. https://doi.org/10.1177/2325958219888457
|
| [39] |
Waju B, Dube L, Ahmed M, et al. (2021) Unsuppressed Viral Load Level in Public Health Facilities: Nonvirological Predictors among Adult Antiretroviral Therapy Users in Southwestern Ethiopia. HIV AIDS Res Palliat Care 13: 513-526. https://doi.org/10.2147/HIV.S304653
|
| [40] |
Isaac EW, Ajani A, Difa AJ, et al. (2021) Viral Suppression in Adult Nigerians in a Regional Antiretroviral Therapy Programme: A Cross Sectional Descriptive Study. World J AIDS 11: 1-14. https://doi.org/10.4236/wja.2021.111001
|
Figures(1) / Tables(2)

Philip Boakye, Adwoa Safowaa. Prevalence and predictors of viral load suppression in adults living with HIV in the western region of Ghana: A cross-sectional study[J]. AIMS Public Health, 2023, 10(2): 469-479. doi: 10.3934/publichealth.2023033







 DownLoad:
DownLoad: