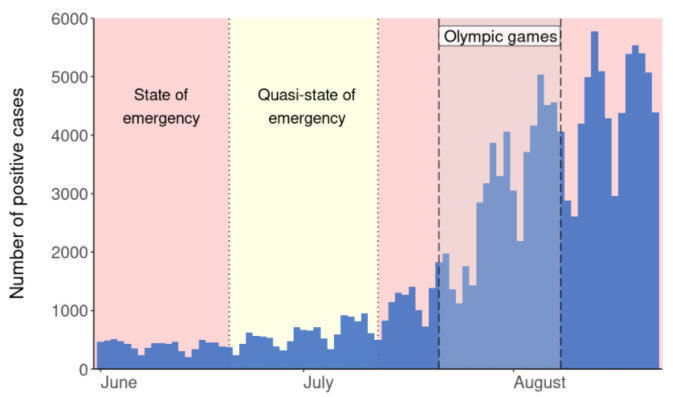
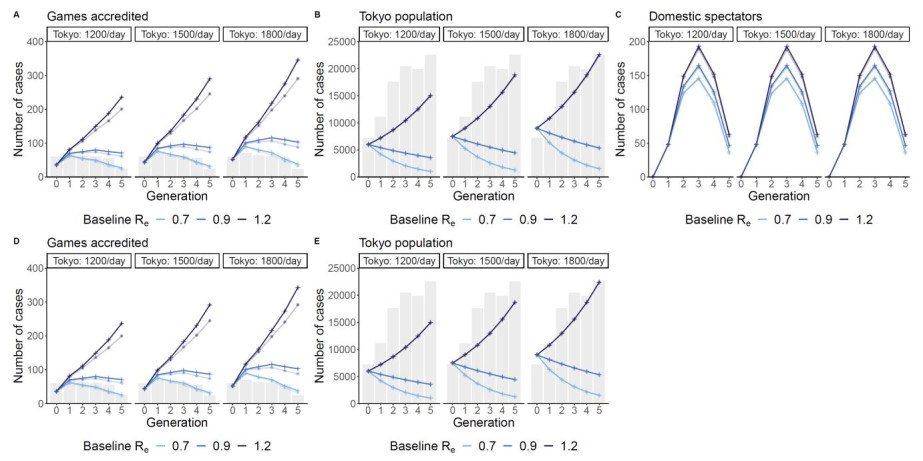
The Tokyo 2020 Olympic and Paralympic Games represent the most diverse international mass gathering event held since the start of the coronavirus disease 2019 (COVID-19) pandemic. Postponed to summer 2021, the rescheduled Games were set to be held amidst what would become the highest-ever levels of COVID-19 transmission in the host city of Tokyo. At the same time, the Delta variant of concern was gaining traction as the dominant viral strain and Japan had yet to exceed fifteen percent of its population fully vaccinated against COVID-19. To quantify the potential number of secondary cases that might arise during the Olympic Games, we performed a scenario analysis using a multitype branching process model. We considered the different contributions to transmission of Games accredited individuals, the general Tokyo population, and domestic spectators. In doing so, we demonstrate how transmission might evolve in these different groups over time, cautioning against any loosening of infection prevention protocols and supporting the decision to ban all spectators. If prevention measures were well observed, we estimated that the number of new cases among Games accredited individuals would approach zero by the end of the Games. However, if transmission was not controlled our model indicated hundreds of Games accredited individuals would become infected and daily incidence in Tokyo would reach upwards of 4,000 cases. Had domestic spectators been allowed (at 50% venue capacity), we estimated that over 250 spectators might have arrived infected to Tokyo venues, potentially generating more than 300 additional secondary infections while in Tokyo/at the Games. We also found the number of cases with infection directly attributable to hypothetical exposure during the Games was highly sensitive to the local epidemic dynamics. Therefore, reducing and maintaining transmission levels below epidemic levels using public health measures would be necessary to prevent cross-group transmission.
Citation: Natalie M. Linton, Sung-mok Jung, Hiroshi Nishiura. Not all fun and games: Potential incidence of SARS-CoV-2 infections during the Tokyo 2020 Olympic Games[J]. Mathematical Biosciences and Engineering, 2021, 18(6): 9685-9696. doi: 10.3934/mbe.2021474
The Tokyo 2020 Olympic and Paralympic Games represent the most diverse international mass gathering event held since the start of the coronavirus disease 2019 (COVID-19) pandemic. Postponed to summer 2021, the rescheduled Games were set to be held amidst what would become the highest-ever levels of COVID-19 transmission in the host city of Tokyo. At the same time, the Delta variant of concern was gaining traction as the dominant viral strain and Japan had yet to exceed fifteen percent of its population fully vaccinated against COVID-19. To quantify the potential number of secondary cases that might arise during the Olympic Games, we performed a scenario analysis using a multitype branching process model. We considered the different contributions to transmission of Games accredited individuals, the general Tokyo population, and domestic spectators. In doing so, we demonstrate how transmission might evolve in these different groups over time, cautioning against any loosening of infection prevention protocols and supporting the decision to ban all spectators. If prevention measures were well observed, we estimated that the number of new cases among Games accredited individuals would approach zero by the end of the Games. However, if transmission was not controlled our model indicated hundreds of Games accredited individuals would become infected and daily incidence in Tokyo would reach upwards of 4,000 cases. Had domestic spectators been allowed (at 50% venue capacity), we estimated that over 250 spectators might have arrived infected to Tokyo venues, potentially generating more than 300 additional secondary infections while in Tokyo/at the Games. We also found the number of cases with infection directly attributable to hypothetical exposure during the Games was highly sensitive to the local epidemic dynamics. Therefore, reducing and maintaining transmission levels below epidemic levels using public health measures would be necessary to prevent cross-group transmission.

| [1] |
T. Hale, N. Angrist, R. Goldszmidt, B. Kira, A. Petherick, T. Phillips, et al., A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker), Nat. Hum. Behav., 5 (2021), 529–538. doi: 10.1038/s41562-021-01079-8 doi: 10.1038/s41562-021-01079-8

|
| [2] |
M. Kosaka, T. Hashimoto, A. Ozaki, T. Tanimoto, M. Kami, Delayed COVID-19 vaccine roll-out in Japan, Lancet, 397 (2021), 2334–2335. doi: 10.1016/S0140-6736(21)01220-4 doi: 10.1016/S0140-6736(21)01220-4
|
| [3] | The Lancet, "We need a global conversation on the 2020 Olympic Games, " Lancet, vol. 397, no. 10291, p. 2225, 2021, doi: 10.1016/s0140-6736(21)01293-9 |
| [4] | H. Anan, et al., Statement regarding infectious disease risk of the Tokyo 2020 Olympic and Paralympic Games, 2021, https://mainichi.jp/graphs/20210618/hpj/00m/040/004000g/4 |
| [5] | International Olympic Committee, "Tokyo 2020 Playbooks, " 2021. https://olympics.com/ioc/tokyo-2020-playbooks |
| [6] |
H. Nishiura, N. M. Linton, A. R. Akhmetzhanov, Serial interval of novel coronavirus (COVID-19) infections. Int. J. Infect. Dis., 2020, 113332. doi: 10.1016/j.ijid.2020.02.060 doi: 10.1016/j.ijid.2020.02.060
|
| [7] | N. M. Linton, A. R. Akhmetzhanov, H. Nishiura, Correlation between times to SARS-CoV-2 symptom onset and secondary transmission undermines epidemic control efforts, medRxiv, doi: 10.1101/2021.08.29.21262512 |
| [8] | 10,000 Olympic volunteers quit, First announcement of the number of people involved in the Games, Asahi Shimbun, https://www.asahi.com/articles/ASP626JJCP62UTQP01X.html |
| [9] | COVID-19 Advisory Board: Professor Nishiura (June 9, 2021), Ministry of Health Labour and Welfare (MHLW), Available from: https://www.mhlw.go.jp/content/10900000/000790389.pdf |
| [10] | COVID-19 Advisory Board: Professor Nishiura (July 21, 2021), Ministry of Health Labour and Welfare (MHLW), Available from: https://www.mhlw.go.jp/content/10900000/000809638.pdf |
| [11] |
K. Ito, C. Piantham, H. Nishiura, Predicted domination of variant Delta of SARS-CoV-2 before Tokyo Olympic Games, Japan, July 2021, Euro. Surveill., 26 (2021), 4–12. doi: 10.2807/1560-7917.ES.2021.26.27.2100570 doi: 10.2807/1560-7917.ES.2021.26.27.2100570
|
| [12] |
H. Nishiura, A. R. Cook, B. J. Cowling, Assortativity and the probability of epidemic extinction: A case study of pandemic influenza A (H1N1-2009), Interdiscip. Perspect. Infect. Dis., 2011 (2011), 194507. doi: 10.1155/2011/194507 doi: 10.1155/2011/194507
|
| [13] | J. O. Lloyd-Smith, S. J. Schreiber, W. M. Getz, "Moving beyond averages: Individual-level variation in disease transmission. In: Mathematical studies of human disease dynamics: Emerging paradigms and challenges, " in Contemporary Mathematics, 2006, pp. 235–258. |
| [14] | R Core Team, "R: A language and environment for statistical computing, " R Foundation for Statistical Computing, Vienna, Austria, 2019, [Online]. Available: https://www.r-project.org/ |
| [15] | J. Lessler, I. Rodriguez-Barraquer, D. A. T. Cummings, T. Garske, M. Van Kerkhove, H. Mills, et al., Estimating potential incidence of MERS-CoV associated with Hajj pilgrims to Saudi Arabia, 2014, PLoS Curr., 6 (2014), 1–16. doi: 10.1371/currents.outbreaks.c5c9c9abd636164a9b6fd4dbda 974369 |
| [16] | Quantitative evaluation of the effects of priority measures and emergency declarations on the epidemic dynamics of COVID-19 (Provisional Version), National Institute of Infectious Diseases (NIID). 2021. Available from: https://www.niid.go.jp/niid/ja/diseases/ka/corona-virus/2019-ncov/2484-idsc/10437-covid19-47.html |
| [17] | COVID-19 Positive Case List, Tokyo 2020. Available from: https://olympics.com/tokyo-2020/en/notices/covid-19-positive-case-list. |
| [18] | Consensus Statement on COVID-19, Scientific Pandemic Influenza Group on Modelling Operational sub-group (SPI-M-O). Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/993321/S1267_SPI-M-O_Consensus_Statement.pdf. |
| [19] | COVID-19 Advisory Board: Professor Nishiura (August 11, 2021), Ministry of Health Labour and Welfare (MHLW). Available from: https://www.mhlw.go.jp/content/10900000/000818359.pdf. |
| [20] |
K. Nakajo, H. Nishiura, Transmissibility of asymptomatic COVID-19: Data from Japanese clusters, Int. J. Infect. Dis., 105 (2021), 236–238. doi: 10.1016/j.ijid.2021.02.065 doi: 10.1016/j.ijid.2021.02.065
|
| [21] |
A. Tariq, Y. Lee, K. Roosa, S. Blumberg, P. Yan, S. Ma, G. Chowell, Real-time monitoring the transmission potential of COVID-19 in Singapore, March 2020, BMC Med., 18 (2020), 166. doi:10.1186/s12916-020-01615-9. doi: 10.1186/s12916-020-01615-9
|
 mbe-18-06-474 Supplementary.docx mbe-18-06-474 Supplementary.docx |
 |
Figures(3) / Tables(3)

Natalie M. Linton, Sung-mok Jung, Hiroshi Nishiura. Not all fun and games: Potential incidence of SARS-CoV-2 infections during the Tokyo 2020 Olympic Games[J]. Mathematical Biosciences and Engineering, 2021, 18(6): 9685-9696. doi: 10.3934/mbe.2021474







 DownLoad:
DownLoad: