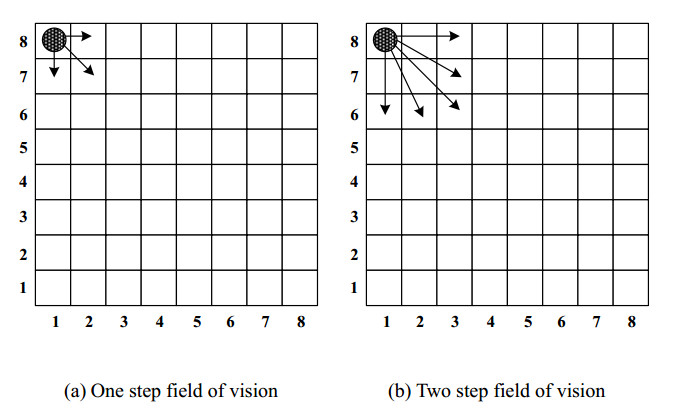
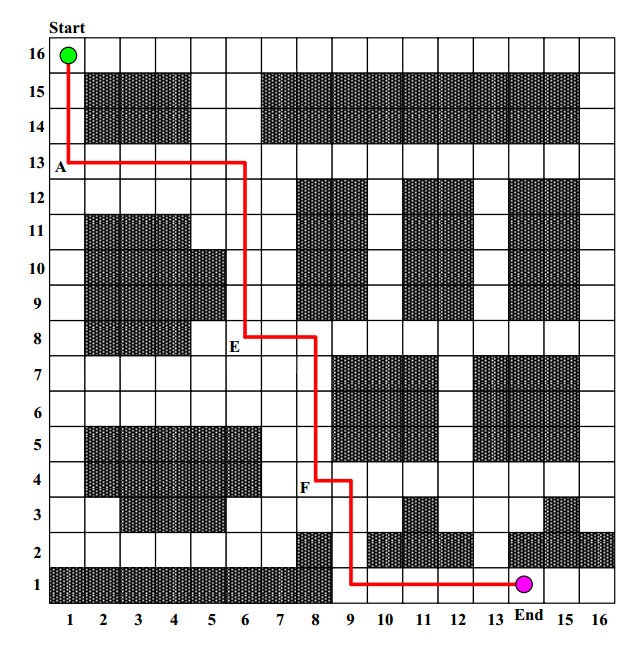
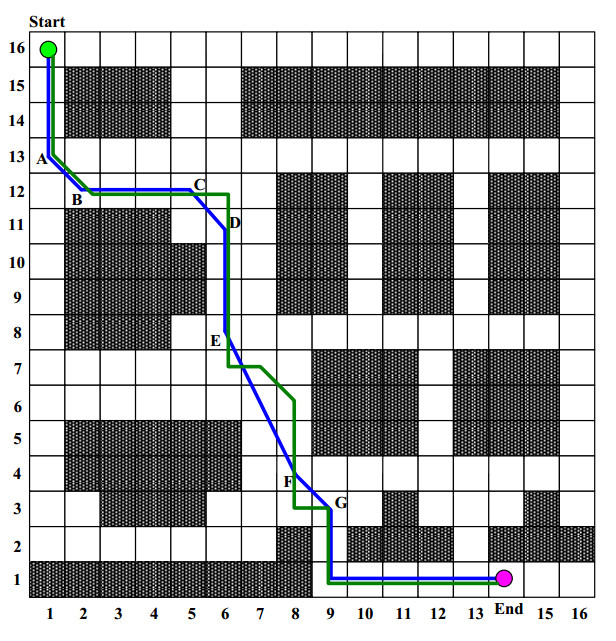
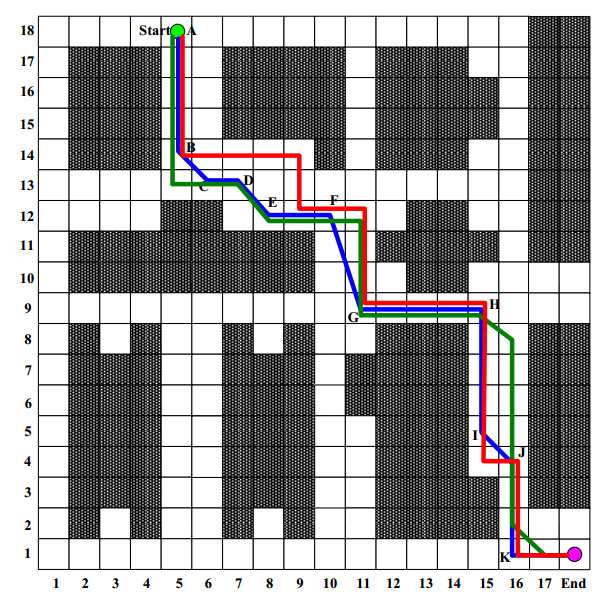
The path planning of robot is of great significance for the logistics industry, which helps to improve the efficiency of warehousing, sorting and distribution. On the basis of ant colony algorithm, multi step search strategy is used instead of single step search strategy, pheromone update mechanism is redesigned, and path smoothing is configured to improve the performance of the algorithm. The experimental results show that the improved ant colony algorithm proposed in this paper can plan a shorter optimal path on the 16 * 16 grid logistics storage site, and the path length is saved by 9.21%.
Citation: Tian Xue, Liu Li, Liu Shuang, Du Zhiping, Pang Ming. Path planning of mobile robot based on improved ant colony algorithm for logistics[J]. Mathematical Biosciences and Engineering, 2021, 18(4): 3034-3045. doi: 10.3934/mbe.2021152
The path planning of robot is of great significance for the logistics industry, which helps to improve the efficiency of warehousing, sorting and distribution. On the basis of ant colony algorithm, multi step search strategy is used instead of single step search strategy, pheromone update mechanism is redesigned, and path smoothing is configured to improve the performance of the algorithm. The experimental results show that the improved ant colony algorithm proposed in this paper can plan a shorter optimal path on the 16 * 16 grid logistics storage site, and the path length is saved by 9.21%.

| [1] |
H. Fazlollahtabar, Comparative simulation study for configuring turning point in multiple robot path planning: Robust data envelopment analysis, Robotica, 38 (2020), 925-939. doi: 10.1017/S0263574719001164

|
| [2] |
B. P. Huynh, Y. L. Kuo, Dynamic filtered path tracking control for a 3RRR robot using optimal recursive path planning and vision-based pose estimation, IEEE Access, 8 (2020), 174736-174750. doi: 10.1109/ACCESS.2020.3025952
|
| [3] | B. Li, H. Liang, Multi-robot path planning method based on prior knowledge and Q-learning algorithms, in Journal of Physics: Conference Series, IOP Publishing, 1624 (2020), 042008. |
| [4] |
R. S. Pol, B. S. Rani, M. Murugan, Socio-realistic optimal path planning for indoor real-time autonomous mobile robot navigation, Int. J. Veh. Auton. Syst., 15 (2020), 101-113. doi: 10.1504/IJVAS.2020.108399
|
| [5] |
Q. Qian, J. Wu, Z. Wang, Optimal path planning for two-wheeled self-balancing vehicle pendulum robot based on quantum-behaved particle swarm optimization algorithm, Pers. Ubiquitous Comput., 23 (2019), 393-403. doi: 10.1007/s00779-019-01216-1
|
| [6] | A. K. Rath, D. R. Parhi, H. C. Das, Design of a hybrid controller using genetic algorithm and neural network for path planning of a humanoid robot, Int. J. Intell. Unmanned Syst., 2020. |
| [7] | F. Gul, W. Rahiman, S. S. N. Alhady, A. Ali, I. Mir, A. Jalil, Meta-heuristic approach for solving multi-objective path planning for autonomous guided robot using PSO-GWO optimization algorithm with evolutionary programming, J. Ambient Intell. Humanized Comput., (2020), 1-18. |
| [8] |
A. H. Hasan, A. T. Sadiq, Robot path planning based on hybrid improved D* with particle swarm optimization algorithms in dynamic environment, J. Comput. Theor. Nanosci., 16 (2019), 1062-1073. doi: 10.1166/jctn.2019.7998
|
| [9] | R. K. Dewangan, A. Shukla, W. W. Godfrey, A solution for priority-based multi-robot path planning problem with obstacles using ant lion optimization, Mod. Phys. Lett. B, 34 (2020), 2050137. |
| [10] |
Y. Kawasaki, A. Yorozu, M. Takahashi, E. Pagello, A multimodal path planning approach to human robot interaction based on integrating action modeling, J. Intell. Rob. Syst., 100 (2020), 955-972. doi: 10.1007/s10846-020-01244-7
|
| [11] | K. I. Ghathwan, A. J. Mohammed, Y. Yusof, Optimal robot path planning using enhanced particle swarm optimization algorithm, Iraqi J. Sci., 61 (2020), 178-184. |
| [12] |
T. Zhang, G. Chen, Q. Zeng, G. Song, C. Li, H. Duan, Routing clustering protocol for 3d wireless sensor networks based on fragile collection ant colony algorithm, IEEE Access, 8 (2020), 58874-58888. doi: 10.1109/ACCESS.2020.2982691
|
| [13] |
S. Chaouch, A. Moussa, I. B. Marzoug, N. Ladhari, Colour recipe prediction using ant colony algorithm: principle of resolution and analysis of performances, Color. Technol., 135 (2019), 349-360. doi: 10.1111/cote.12409
|
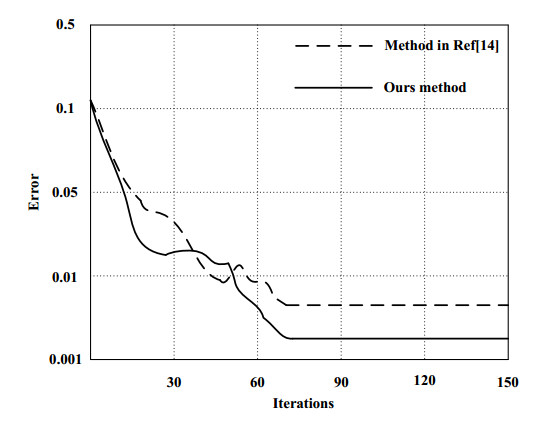
| [14] | K. Akka, F. Khaber, Mobile robot path planning using an improved ant colony optimization, Int. J. Adv. Robotic Syst., 15 (2018). |
Figures(5) / Tables(2)

Tian Xue, Liu Li, Liu Shuang, Du Zhiping, Pang Ming. Path planning of mobile robot based on improved ant colony algorithm for logistics[J]. Mathematical Biosciences and Engineering, 2021, 18(4): 3034-3045. doi: 10.3934/mbe.2021152







 DownLoad:
DownLoad: