Weeds are one of the significant problems that impact agriculture production. Farmers have been using synthetic herbicides to control weed infestations in the field. However, the excessive usage of herbicides has led to various environmental concerns, including the emergence of herbicide resistant weeds. Allelopathy is an environment-friendly alternative that can control weeds. Here, we performed a systematic literature review to assess the potential and effects of allelopathy under laboratory, greenhouse and field conditions. Articles were collected by searching the SCOPUS database and guided by PRISMA. Of 371 studies identified, forty-three articles used allelopathy to control weeds under greenhouse and field conditions, with Poaceae being the prominent family studied as donor plants. Six articles reported up to 80% weed growth suppression when spraying allelopathy extract under greenhouse conditions, while mulch and soil incorporated with donor plants contributed over 50% suppression under field conditions. The findings revealed that 20 studies had conducted metabolite identification to determine the allelochemicals with phytotoxic activity against target plants. However, the mechanism of allelopathy was not thoroughly investigated. In conclusion, we found an increasing trend of allelopathy experiments conducted under greenhouse and field conditions. Furthermore, field trials should be included to validate laboratory data and to provide insight into allelochemical action and its relationship with the environment.
Citation: Muhd Arif Shaffiq Sahrir, Nornasuha Yusoff, Kamalrul Azlan Azizan. Allelopathy activity under laboratory, greenhouse and field conditions: A review[J]. AIMS Agriculture and Food, 2023, 8(1): 78-104. doi: 10.3934/agrfood.2023004
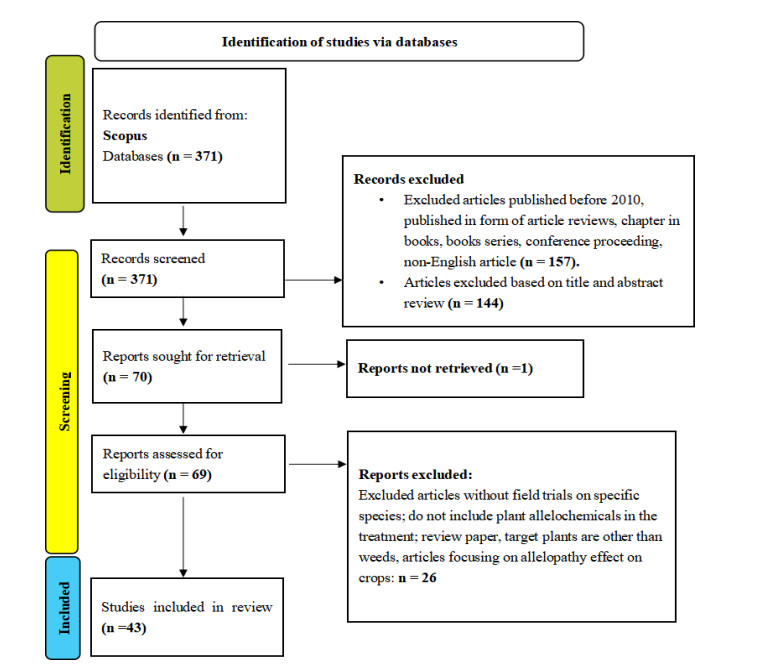
Weeds are one of the significant problems that impact agriculture production. Farmers have been using synthetic herbicides to control weed infestations in the field. However, the excessive usage of herbicides has led to various environmental concerns, including the emergence of herbicide resistant weeds. Allelopathy is an environment-friendly alternative that can control weeds. Here, we performed a systematic literature review to assess the potential and effects of allelopathy under laboratory, greenhouse and field conditions. Articles were collected by searching the SCOPUS database and guided by PRISMA. Of 371 studies identified, forty-three articles used allelopathy to control weeds under greenhouse and field conditions, with Poaceae being the prominent family studied as donor plants. Six articles reported up to 80% weed growth suppression when spraying allelopathy extract under greenhouse conditions, while mulch and soil incorporated with donor plants contributed over 50% suppression under field conditions. The findings revealed that 20 studies had conducted metabolite identification to determine the allelochemicals with phytotoxic activity against target plants. However, the mechanism of allelopathy was not thoroughly investigated. In conclusion, we found an increasing trend of allelopathy experiments conducted under greenhouse and field conditions. Furthermore, field trials should be included to validate laboratory data and to provide insight into allelochemical action and its relationship with the environment.

| [1] |
Heap I (2014) Global perspective of herbicide-resistant weeds. Pest Manag Sci 70: 1306–1315. https://doi.org/10.1002/ps.3696 doi: 10.1002/ps.3696

|
| [2] |
Bhadoria P (2010) Allelopathy: A natural way towards weed management. Am J Exp Agric 1: 7–20. https://doi.org/10.9734/ajea/2011/002 doi: 10.9734/ajea/2011/002
|
| [3] |
Mardani H, Kazantseva E, Onipchenko V, et al. (2016) Evaluation of allelopathic activity of 178 Caucasian plant species. Int J Basic Appl Sci 5: 75–81. http://dx.doi.org/10.14419/ijbas.v5i1.5631 doi: 10.14419/ijbas.v5i1.5631
|
| [4] | Nornasuha Y, Ismail BS (2017) Sustainable weed management using allelopathic approach. Malays Appl Biol 46: 1–10. |
| [5] | Heap I (2021) The International Herbicide-Resistant Weed Database. Herbicide Resistance Action Committee. Available form: http://www.weedscience.org/Pages/ChronologicalIncrease.aspx |
| [6] | Rice EL (1984) Allelopathy. New York: Academic Press. |
| [7] | Wan Zateel Aeeda WAH, Nornasuha Y, Muhd Arif Shaffiq S, et al. (2022) Allelopathic potential assessment of root exudates and rhizosphere soil of Turnera subulata. Biosci Res 18: 145–152. |
| [8] | Soltys D, Krasuska U, Bogatek R, et al. (2013) Allelochemicals as bioherbicides—Present and perspectives. In: Price AJ, Kelton JA (Eds), Herbicides—Current Research and Case Studies in Use, United Kingdom: InTech, 542. Available from: https://doi.org/10.5772/56185. |
| [9] |
Li ZH, Wang Q, Ruan X, et al. (2010) Phenolics and plant allelopathy. Molecules 15: 8934–8950. https://doi.org/10.3390/molecules15128933 doi: 10.3390/molecules15128933
|
| [10] | Einhellig FA (1994) Mechanism of action of allelochemicals in allelopathy. In: Inderjit, Dakshini KMM, Einhellig FA (Eds.), Allelopathy: Organisms, Processes, and Applications, Washington: American Chemical Society, 96–116. |
| [11] |
Staszek P, Krasuska U, Ciacka K, et al. (2021) ROS Metabolism perturbation as an element of mode of action of allelochemicals. Antioxidants 10: 1648. https://doi.org/10.3390/antiox10111648 doi: 10.3390/antiox10111648
|
| [12] |
Yu J, Morishita DW (2014) Response of seven weed species to corn gluten meal and white mustard (Sinapis alba) seed meal rates. Weed Technol 28: 259–265. https://doi.org/10.1614/wt-d-13-00116.1 doi: 10.1614/wt-d-13-00116.1
|
| [13] |
Harker KN, O'Donovan JT (2013) Recent weed control, weed management, and integrated weed management. Weed Technol 27: 1–11. https://doi.org/10.1614/WT-D-12-00109.1 doi: 10.1614/WT-D-12-00109.1
|
| [14] | Duke SO (1985) Biosynthesis of phenolic compounds. In: Thompson AC (Eds.), The chemistry of allelopathy: Biochemical interaction among plants, Michigan: American Chemical Society, 113–131. https://doi.org/10.1021/bk-1985-0268.ch008 |
| [15] | Azmi M, Abdullah MZ, Fujii Y (2000) Exploratory study on allelopathic effect of selected Malaysian rice varieties and rice field weed species. J Trop Agric Fd 28: 39–54. |
| [16] |
Page MJ, McKenzie JE, Bossuyt PM, et al. (2021) The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br Med J 372: 1–8. https://doi.org/10.1136/bmj.n71 doi: 10.1136/bmj.n71
|
| [17] |
Mohamed Shaffril HA, Ahmad N, Samsuddin SF, et al. (2020) Systematic literature review on adaptation towards climate change impacts among indigenous people in the Asia Pacific regions. J Cleaner Prod 258: 120595. https://doi.org/10.1016/j.jclepro.2020.120595 doi: 10.1016/j.jclepro.2020.120595
|
| [18] | Uddin MR, Park KW, Han SM, et al. (2012) Effects of sorgoleone allelochemical on chlorophyll fluorescence and growth inhibition in weeds. Allelopathy 30: 61–70. |
| [19] | Uddin MR, Park KW, Pyon JY, et al. (2013) Combined herbicidal effect of two natural products (sorgoleone and hairy root extract of tartary buckwheat) on crops and weeds. Aust J Crop Sci 7: 227–233. |
| [20] | Alsaadawi IS, Khaliq A, Lahmod NR, et al. (2013) Weed management in broad bean (Vicia faba L.) through allelopathic Sorghum bicolor (L.) Moench residues and reduced rate of a pre-plant herbicide. Allelopathy J 32: 203–212. |
| [21] |
Murimwa JC, Rugare JT, Mabasa S, et al. (2019) Allelopathic effects of aqueous extracts of sorghum (Sorghum bicolor L. Moench) on the early seedling growth of sesame (Sesamum indicum L.) varieties and selected weeds. Int J Agron 2019: 5494756. https://doi.org/10.1155/2019/5494756 doi: 10.1155/2019/5494756
|
| [22] |
Farooq M, Khan I, Nawaz A, et al. (2020) Using sorghum to suppress weeds in autumn planted maise. Crop Prot 133: 105162. https://doi.org/10.1016/j.cropro.2020.105162 doi: 10.1016/j.cropro.2020.105162
|
| [23] | Zawia AA, Nesseef L, Elahmar MA, et al. (2021) Fluorescence and chlorophyll content as indicators of the efficacy of plant extracts of Ambrosia artemisiifolia and Sorghum halepense in weed control. Fresenius Environ Bull 30: 707–715. |
| [24] | Asad M, Mubeen K, Sarwar N, et al. (2019) Congress grass possess herbicidal potential against weeds in wheat fields. Asian J Agric Biol 7: 501–511. |
| [25] |
Han C, Shao H, Zhou S, et al. (2021) Chemical composition and phytotoxicity of essential oil from invasive plant, Ambrosia artemisiifolia L. Ecotoxicol Environ Saf 211: 111879. https://doi.org/10.1016/j.ecoenv.2020.111879 doi: 10.1016/j.ecoenv.2020.111879
|
| [26] |
Boydston RA, Morra MJ, Borek V, et al. (2011) Onion and weed response to mustard (Sinapis alba) seed meal. Weed Sci 59: 546–552. https://doi.org/10.1614/ws-d-10-00185.1 doi: 10.1614/ws-d-10-00185.1
|
| [27] | Ahmed SAA, Messiha NK, Kowthar El-Rokiek G, et al. (2016) The allelopathic efficiency of two Brassicaceae plant seeds in controlling weeds associating sunflower plants. Res J Pharm Biol Chem Sci 7: 158–165. |
| [28] |
Gad El-Rokiek K, El-Din SAS, Shehata AN, et al. (2016) A study on controlling Setaria viridis and Corchorus olitorius associated with Phaseolus vulgaris growth using natural extracts of Chenopodium album. J Plant Prot Res 56: 186–192. https://doi.org/10.1515/jppr-2016-0031 doi: 10.1515/jppr-2016-0031
|
| [29] |
Morra MJ, Popova IE, Boydston RA (2018) Bioherbicidal activity of Sinapis alba seed meal extracts. Ind Crops Prod 115: 174–181. https://doi.org/10.1016/j.indcrop.2018.02.027 doi: 10.1016/j.indcrop.2018.02.027
|
| [30] |
El-Wakeel MA, Ahmed SEDAEG, El-Desoki ER (2019) Allelopathic efficiency of Eruca sativa in controlling two weeds associated with Pisum sativum plants. J Plant Prot Res 59: 170–176. https://doi.org/10.24425/jppr.2019.129283 doi: 10.24425/jppr.2019.129283
|
| [31] |
Meksawat S, Pornprom T (2010) Allelopathic effect of itchgrass (Rottboellia cochinchinensis) on seed germination and plant growth. Weed Biol Manage 10: 16–24. https://doi.org/10.1111/j.1445-6664.2010.00362.x doi: 10.1111/j.1445-6664.2010.00362.x
|
| [32] |
Dayan FE, Howell J, Marais JP, et al. (2011) Manuka oil, a natural herbicide with pre-emergence activity. Weed Sci 59: 464–469. https://doi.org/10.1614/ws-d-11-00043.1 doi: 10.1614/ws-d-11-00043.1
|
| [33] |
Tesio F, Weston LA, Ferrero A (2011) Allelochemicals identified from Jerusalem artichoke (Helianthus tuberosus L.) residues and their potential inhibitory activity in the field and laboratory. Sci Hortic 129: 361–368. https://doi.org/10.1016/j.scienta.2011.04.003 doi: 10.1016/j.scienta.2011.04.003
|
| [34] |
Bezuidenhout SR, Reinhardt CF, Whitwell MI (2012) Cover crops of oats, stooling rye and three annual ryegrass cultivars influence maise and Cyperus esculentus growth. Weed Res 52: 153–160. https://doi.org/10.1111/j.1365-3180.2011.00900.x doi: 10.1111/j.1365-3180.2011.00900.x
|
| [35] |
de Bertoldi C, De Leo M, Ercoli L, et al. (2012) Chemical profile of Festuca arundinacea extract showing allelochemical activity. Chemoecology 22: 13–21. https://doi.org/10.1007/s00049-011-0092-4 doi: 10.1007/s00049-011-0092-4
|
| [36] |
El-Rokiek KG, El-Nagdi WM, El-Masry RR (2012) Controlling of Portulaca oleracea and Meloidogyne incognita infecting sunflower using leaf extracts of Psidium guava. Arch Phytopathol Plant Prot 45: 2369–2385. https://doi.org/10.1080/03235408.2012.727326 doi: 10.1080/03235408.2012.727326
|
| [37] |
Skinner EM, Díaz-Pérez JC, Phatak SC, et al. (2012) Allelopathic effects of sunnhemp (Crotalaria juncea L.) on germination of vegetables and weeds. HortScience 47: 138–142. https://doi.org/10.21273/hortsci.47.1.138 doi: 10.21273/hortsci.47.1.138
|
| [38] |
Tabaglio V, Marocco A, Schulz M (2013) Allelopathic cover crop of rye for integrated weed control in sustainable agroecosystems. Ital J Agron 8: 35–40. https://doi.org/10.4081/ija.2013.e5 doi: 10.4081/ija.2013.e5
|
| [39] |
Wang CM, Chen HT, Li TC, et al. (2014) The role of pentacyclic triterpenoids in the allelopathic effects of Alstonia scholaris. J Chem Ecol 40: 90–98. https://doi.org/10.1007/s10886-013-0376-y doi: 10.1007/s10886-013-0376-y
|
| [40] |
Intanon S, Hulting AG, Mallory-Smith CA (2015) Field evaluation of meadowfoam (Limnanthes alba) seed meal for weed management. Weed Sci 63: 302–311. https://doi.org/10.1614/ws-d-14-00087.1 doi: 10.1614/ws-d-14-00087.1
|
| [41] | Kordali S, Tazegul A, Cakir A (2015) Phytotoxic effects of Nepeta meyeri Benth. extracts and essential oil on seed germinations and seedling growths of four weed species. Rec Nat Prod 9: 404–418. |
| [42] |
Wathugala DL, Ranagalage AS (2015) Effect of incorporating the residues of Sri Lankan improved rice (Oryza sativa L.) varieties on germination and growth of barnyard grass (Echinochloa crus-galli). J Natl Sci Found Sri Lanka 43: 57–64. https://doi.org/10.4038/jnsfsr.v43i1.7915 doi: 10.4038/jnsfsr.v43i1.7915
|
| [43] |
Aslani F, Juraimi AS, Ahmad-Hamdani MS, et al. (2016) Control of weeds in glasshouse and rice field conditions by phytotoxic effects of Tinospora crispa (L.) Hook. f. & Thomson leaves. Chil J Agric Res 76: 432–440. https://doi.org/10.4067/S0718-58392016000400006 doi: 10.4067/S0718-58392016000400006
|
| [44] |
Sturm DJ, Kunz C, Gerhards R (2016) Inhibitory effects of cover crop mulch on germination and growth of Stellaria media (L.) Vill., Chenopodium album L. and Matricaria chamomilla L. Crop Prot 90: 125–131. https://doi.org/10.1016/j.cropro.2016.08.032 doi: 10.1016/j.cropro.2016.08.032
|
| [45] |
Bali AS, Batish DR, Singh HP, et al. (2017). Phytotoxicity and weed management potential of leaf extracts of Callistemon viminalis against the weeds of rice. Acta Physiol Plant 39: 25. https://doi.org/10.1007/s11738-016-2313-5 doi: 10.1007/s11738-016-2313-5
|
| [46] |
Hazrati H, Saharkhiz MJ, Niakousari M, et al. (2017) Natural herbicide activity of Satureja hortensis L. essential oil nano emulsion on the seed germination and morphophysiological features of two important weed species. Ecotoxicol Environ Saf 142: 423–430. https://doi.org/10.1016/j.ecoenv.2017.04.041 doi: 10.1016/j.ecoenv.2017.04.041
|
| [47] |
Abbas T, Nadeem MA, Tanveer A, et al. (2018) Exploring the herbicidal and hormetic potential of allelopathic crops against fenoxaprop resistant Phalaris minor. Planta Daninha 36: 1–8. https://doi.org/10.1590/S0100-83582018360100056 doi: 10.1590/S0100-83582018360100056
|
| [48] |
Álvarez-Iglesias L, Puig CG, Revilla P, et al. (2018) Faba bean as green manure for field weed control in maize. Weed Res 58: 437–449. https://doi.org/10.1111/wre.12335 doi: 10.1111/wre.12335
|
| [49] |
El-Mergawi R, El-Desoki, ER (2018) Allelopathic activities of celery extract and its fractions against Corchorus olitorius, Echinochloa Crus-galli and Portulaca oleracea weeds. Adv Hortic Sci 32: 503–510. https://doi.org/10.13128/ahs-22083 doi: 10.13128/ahs-22083
|
| [50] |
Ghafari Z, Karimmojeni H, Majidi MM, et al. (2018) Assessment of the allelopathic potential of cumin accessions in different soil water potential. J Crop Sci Biotechnol 21: 249–260. https://doi.org/10.1007/s12892-017-0107-0 doi: 10.1007/s12892-017-0107-0
|
| [51] | Gołebiowska H, Kieloch R, Rdzanek M, et al. (2018) The effect of plant extracts from Solanum nigrum L. and Avena fatua L. on the growth of some weed species and agropathogenic fungi. Acta Agrobot 71: 1739. https://doi.org/10.5586/aa.1739 |
| [52] |
Dhungana SK, Kim ID, Adhikari B, et al. (2019) Reduced germination and seedling vigor of weeds with root extracts of maise and soybean, and the mechanism defined as allelopathic. J Crop Sci Biotechnol 22: 11–16. https://doi.org/10.1007/s12892-018-0251-0 doi: 10.1007/s12892-018-0251-0
|
| [53] |
El-Metwally IM, El-Rokiek KG (2019) Eucalyptus citriodora leaf extract as a source of allelochemicals for weed control in pea fields compared with some chemical herbicides. J Plant Prot Res 59: 392–399. https://doi.org/10.24425/jppr.2019.129751 doi: 10.24425/jppr.2019.129751
|
| [54] | Frabboni L, Tarantino A, Petruzzi F, et al. (2019) Bio-herbicidal effects of oregano and rosemary essential oils on chamomile (Matricaria chamomilla L.) crop in organic farming system. Agronomy 9: 475. https://doi.org/10.3390/agronomy9090475 |
| [55] | Al-Batsh LJ, Qasem JR (2020) Phytotoxicity of wild plants extracts to redroot pigweed (Amaranthus retroflexus L.) and nettle-leaved goosefoot (Chenopodium murale L.). Pak J Agric Sci 57: 1441–1456. https://doi.org/10.21162/PAKJAS/20.9695 |
| [56] |
Begum K, Motobayashi T, Hasan N, et al. (2020) Indigo as a plant growth inhibitory chemical from the fruit pulp of Couroupita guianensis Aubl. Agronomy 10: 1388. https://doi.org/10.3390/agronomy10091388 doi: 10.3390/agronomy10091388
|
| [57] | Ghimire BK, Hwang MH, Sacks EJ, et al. (2020). Screening of allelochemicals in Miscanthus sacchariflorus extracts and assessment of their effects on germination and seedling growth of common weeds. Plants 9: 1313. https://doi.org/10.3390/plants9101313 |
| [58] |
Pardo-Muras M, Puig CG, Souza-Alonso P, et al. (2020) The phytotoxic potential of the flowering foliage of gorse (Ulex europaeus) and scotch broom (Cytisus scoparius), as pre-emergent weed control in maise in a glasshouse pot experiment. Plants 9: 203. https://doi.org/10.3390/plants9020203 doi: 10.3390/plants9020203
|
| [59] | Verdeguer M, Torres-Pagan N, Muñoz M, et al. (2020). Herbicidal activity of Thymbra capitata (L.) Cav. essential oil. Molecules 25: 2832. https://doi.org/10.3390/molecules25122832 |
| [60] | Kalinova J (2010) Allelopathy and organic farming. In: Lichtfouse E (Eds.), Sociology, Organic Farming, Climate Change and Soil Science, Springer, 379–418. |
| [61] | Sodaeizadeh H, Rafieiolhossaini M, Havlík J, et al. (2009) Allelopathic activity of different plant parts of Peganum harmala L. and identification of their growth inhibitors substances. Plant Growth Regul 59: 227–236. https://doi.org/10.1007/s10725-009-9408-6 |
| [62] | Teasdale JR, Brandsaeter LO, Calegari A, et al. (2007) Cover crops and weed management. In: Upadhyaya MK, Blackshaw R (Eds.), Non-Chemical Weed Management: Principles, Concepts and Technology, CAB International, 49–64. |
| [63] |
Oraon S, Mondai S (2021) Allelopathic effect of lamiaceous weeds on seed germination and early growth of aromatic rice (Oryza sativa 'Gobindobhog'). Acta Agrobot 74: 741. https://doi.org/10.5586/aa.741 doi: 10.5586/aa.741
|
| [64] |
Tan PW, Ismail BS, Chuah TS, et al. (2018) Herbicidal potential of the allelochemicals from Pennisetum purpureum Schumach. on the seedling growth of Paspalum conjugatum. Aust J Crop Sci 12: 173–177. https://doi.org/10.21475/ajcs.18.12.02.pne256 doi: 10.21475/ajcs.18.12.02.pne256
|
| [65] |
Mahé I, Chauvel B, Colbach N, et al. (2022) Deciphering field-based evidences for crop allelopathy in weed regulation. A review. Agron Sustain Dev 42: 50. https://doi.org/10.1007/s13593-021-00749-1 doi: 10.1007/s13593-021-00749-1
|


Figures(3) / Tables(4)

Muhd Arif Shaffiq Sahrir, Nornasuha Yusoff, Kamalrul Azlan Azizan. Allelopathy activity under laboratory, greenhouse and field conditions: A review[J]. AIMS Agriculture and Food, 2023, 8(1): 78-104. doi: 10.3934/agrfood.2023004







 DownLoad:
DownLoad: