Obesity represents one of the wellness diseases concurring to increase the incidence of diabetes, cardiovascular diseases, and cancer. One of the main perpetuating factors of obesity is food craving, which is characterized by an urgent desire to eat a large and various amount of food, regardless of calories requirement or satiety signals, and it might be addressed to the alteration of the dorsolateral prefrontal cortex (DLPFC) activity. Despite most of the gold-standard therapies focus on symptom treatment only, non-invasive brain stimulation techniques such as transcranial direct current stimulation (tDCS) could help treat overeating by modulating specific neural pathways. The current systematic review was conducted to identify whether convergent evidence supporting the usefulness of tDCS to deal with food craving are present in the literature. The review was conducted by searching articles published up to January 1st 2022 on MEDLINE, Scopus and PsycInfo databases. We included studies investigating the effects of tDCS on food craving in subjects affected by overweight and obesity. According to eligibility criteria, 5 articles were included. Results showed that tDCS targeting left DLPFC with unipolar montage induced ameliorating effects on food craving. Controversial results were shown for the other studies, that might be ascribable to the use of bipolar montage, and the choice of other target areas. Further investigations including expectancy effect control, larger sample sizes and follow-up are needed to support more robust conclusions. To conclude, tDCS combined with the use of psychoeducative intervention, diet and physical activity, might represents a potential to manage food craving in individuals with overweight and obesity.
Citation: Graziella Orrù, Valentina Cesari, Eleonora Malloggi, Ciro Conversano, Danilo Menicucci, Alessandro Rotondo, Cristina Scarpazza, Laura Marchi, Angelo Gemignani. The effects of Transcranial Direct Current Stimulation on food craving and food intake in individuals affected by obesity and overweight: a mini review of the magnitude of the effects[J]. AIMS Neuroscience, 2022, 9(3): 358-372. doi: 10.3934/Neuroscience.2022020
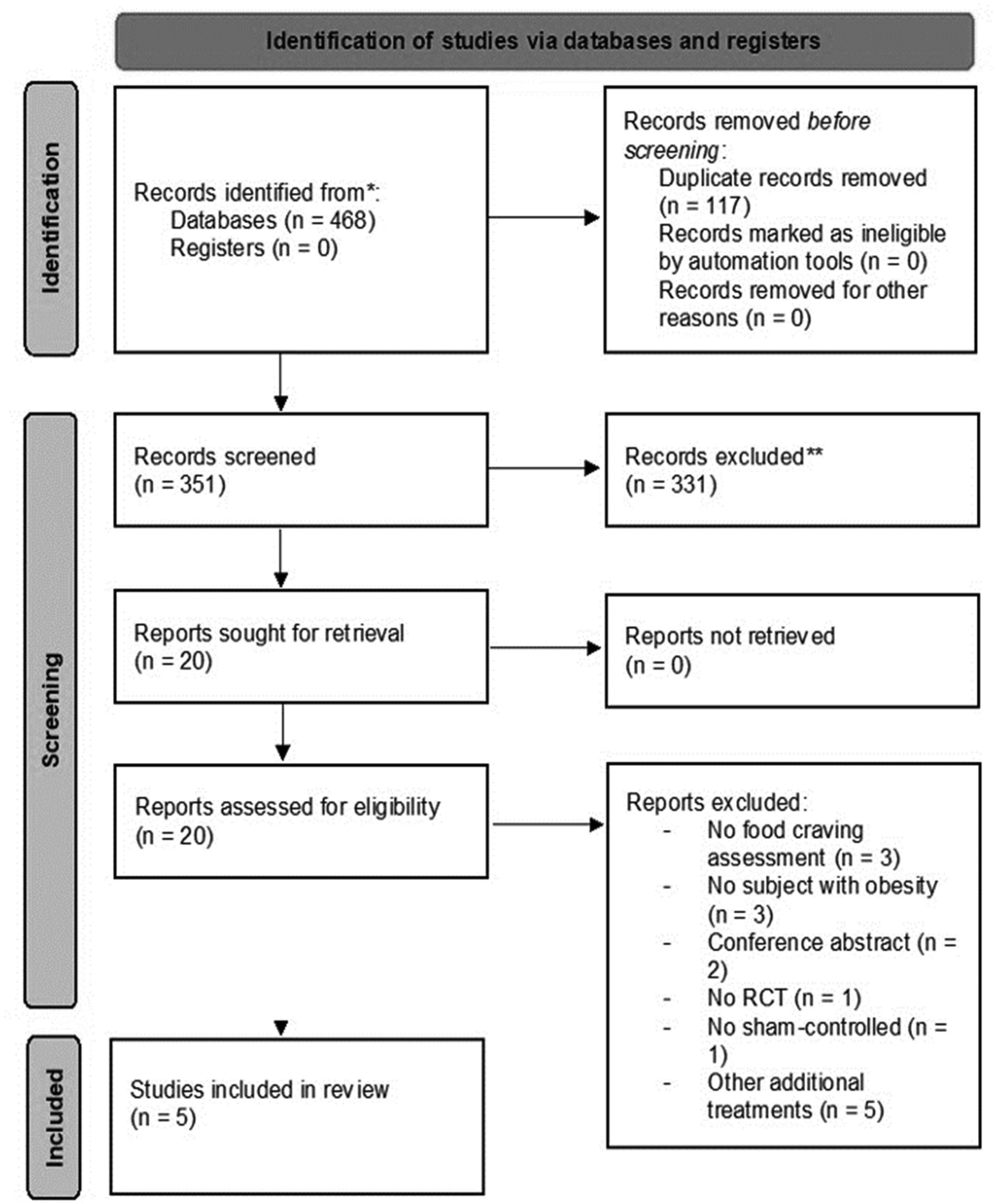
Obesity represents one of the wellness diseases concurring to increase the incidence of diabetes, cardiovascular diseases, and cancer. One of the main perpetuating factors of obesity is food craving, which is characterized by an urgent desire to eat a large and various amount of food, regardless of calories requirement or satiety signals, and it might be addressed to the alteration of the dorsolateral prefrontal cortex (DLPFC) activity. Despite most of the gold-standard therapies focus on symptom treatment only, non-invasive brain stimulation techniques such as transcranial direct current stimulation (tDCS) could help treat overeating by modulating specific neural pathways. The current systematic review was conducted to identify whether convergent evidence supporting the usefulness of tDCS to deal with food craving are present in the literature. The review was conducted by searching articles published up to January 1st 2022 on MEDLINE, Scopus and PsycInfo databases. We included studies investigating the effects of tDCS on food craving in subjects affected by overweight and obesity. According to eligibility criteria, 5 articles were included. Results showed that tDCS targeting left DLPFC with unipolar montage induced ameliorating effects on food craving. Controversial results were shown for the other studies, that might be ascribable to the use of bipolar montage, and the choice of other target areas. Further investigations including expectancy effect control, larger sample sizes and follow-up are needed to support more robust conclusions. To conclude, tDCS combined with the use of psychoeducative intervention, diet and physical activity, might represents a potential to manage food craving in individuals with overweight and obesity.
anodal transcranial direct current stimulation
Body Mass Index
cathodal transcranial direct current stimulation
dorsolateral prefrontal cortex
left dorsolateral prefrontal cortex
Preferred Reporting Items for Systematic Review
randomized controlled trials
right dorsolateral prefrontal cortex
transcranial direct current stimulation
visual analogue scale

| [1] | World Obesity Day [Internet]World Obesity Federation. [cited 2022 Jul 13]. Available from: https://www.worldobesity.org/what-we-do/world-obesity-day |
| [2] | Iasevoli M, Giantin V, Voci A, et al. (2012) Discussing end-of-life care issues with terminally ill patients and their relatives: comparisons among physicians, nurses and psychologists. Aging Clin Exp Res 24: 35-42. |
| [3] |
Salari N, Hosseinian-Far A, Jalali R, et al. (2020) Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Globalization Health 16: 57. https://doi.org/10.1186/s12992-020-00589-w 
|
| [4] | Maharaj PE, Barclay N, Descartes C, et al. (2019) Intimate Partner Violence and Sleep: An Overview of Sleep Disturbances and Interventions. Handbook of Interpersonal Violence and Abuse Across the Lifespan: A project of the National Partnership to End Interpersonal Violence Across the Lifespan (NPEIV) [Internet] . Cham: Springer International Publishing p. 1-25. Available from: https://doi.org/10.1007/978-3-319-62122-7_132-1. [cited 2022 May 12] |
| [5] |
Mattioli AV, Pinti M, Farinetti A, et al. (2020) Obesity risk during collective quarantine for the COVID-19 epidemic. Obes Med 20: 100263. https://doi.org/10.1016/j.obmed.2020.100263
|
| [6] |
Weingarten HP, Elston D (1990) The phenomenology of food cravings. Appetite 15: 231-246. https://doi.org/10.1016/0195-6663(90)90023-2
|
| [7] |
Pelchat ML, Johnson A, Chan R, et al. (2004) Images of desire: food-craving activation during fMRI. Neuroimage 23: 1486-1493. https://doi.org/10.1016/j.neuroimage.2004.08.023
|
| [8] |
Bénard M, Camilleri GM, Etilé F, et al. (2017) Association between Impulsivity and Weight Status in a General Population. Nutrients 9: E217. https://doi.org/10.3390/nu9030217
|
| [9] | Favieri F, Forte G, Casagrande M (2019) The Executive Functions in Overweight and Obesity: A Systematic Review of Neuropsychological Cross-Sectional and Longitudinal Studies. Front Psychol . https://doi.org/10.3389/fpsyg.2019.02126 |
| [10] |
Basdevant A, Craplet C, Guy-Grand B (1993) Snacking patterns in obese French women. Appetite 21: 17-23. https://doi.org/10.1006/appe.1993.1033
|
| [11] |
Narayanaswami V, Dwoskin LP (2017) Obesity: Current and potential pharmacotherapeutics and targets. Pharmacol Ther 170: 116-147. https://doi.org/10.1016/j.pharmthera.2016.10.015
|
| [12] |
Uher R, Murphy T, Brammer MJ, et al. (2004) Medial prefrontal cortex activity associated with symptom provocation in eating disorders. Am J Psychiatry 161: 1238-1246. https://doi.org/10.1176/appi.ajp.161.7.1238
|
| [13] |
Fabricatore AN, Wadden TA (2004) Psychological aspects of obesity. Clin Dermatol 22: 332-337. https://doi.org/10.1016/j.clindermatol.2004.01.006
|
| [14] |
Kim S, Lee D (2011) Prefrontal Cortex and Impulsive Decision Making. Biol Psychiatry 69: 1140-1146. https://doi.org/10.1016/j.biopsych.2010.07.005
|
| [15] |
Szabo-Reed AN, Martin LE, Hu J, et al. (2020) Modeling interactions between brain function, diet adherence behaviors, and weight loss success. Obes Sci Pract 6: 282-292. https://doi.org/10.1002/osp4.403
|
| [16] | Orrù G, Baroni M, Cesari V, et al. (2019) The effect of single and repeated tDCS sessions on motor symptoms in Parkinson's disease: a systematic review. Arch Ital Biol 157: 89-101. https://doi.org/10.12871/00039829201925 |
| [17] | Orrù G, Cesari V, Baroni M, et al. (2020) Letter to the Editor: the application of transcranial direct current stimulation on phantom phenomena. Mediterr J Clin Psyc 8. Available from: https://cab.unime.it/journals/index.php/MJCP/article/view/2382 |
| [18] |
Orrù G, Cesari V, Conversano C, et al. (2021) The clinical application of transcranial direct current stimulation in patients with cerebellar ataxia: a systematic review. Int J Neurosci 131: 681-688. https://doi.org/10.1080/00207454.2020.1750399
|
| [19] |
Orrù G, Conversano C, Hitchcott PK, et al. (2020) Motor stroke recovery after tDCS: a systematic review. Rev Neurosci 31: 201-218. https://doi.org/10.1515/revneuro-2019-0047
|
| [20] |
Chen J, Qin J, He Q, et al. (2020) A Meta-Analysis of Transcranial Direct Current Stimulation on Substance and Food Craving: What Effect Do Modulators Have?. Front Psychiatry 11: 598. https://doi.org/10.3389/fpsyt.2020.00598
|
| [21] |
Nitsche MA, Paulus W (2000) Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J Physiol 527: 633-639. https://doi.org/10.1111/j.1469-7793.2000.t01-1-00633.x
|
| [22] |
Nitsche MA, Fricke K, Henschke U, et al. (2003) Pharmacological modulation of cortical excitability shifts induced by transcranial direct current stimulation in humans. J Physiol 553: 293-301. https://doi.org/10.1113/jphysiol.2003.049916
|
| [23] |
Angius L, Santarnecchi E, Pascual-Leone A, et al. (2019) Transcranial Direct Current Stimulation over the Left Dorsolateral Prefrontal Cortex Improves Inhibitory Control and Endurance Performance in Healthy Individuals. Neuroscience 419: 34-45. https://doi.org/10.1016/j.neuroscience.2019.08.052
|
| [24] |
Ota K, Shinya M, Kudo K (2019) Transcranial Direct Current Stimulation Over Dorsolateral Prefrontal Cortex Modulates Risk-Attitude in Motor Decision-Making. Front Hum Neurosci 13: 297. https://doi.org/10.3389/fnhum.2019.00297
|
| [25] |
Friehs MA, Frings C, Hartwigsen G (2021) Effects of single-session transcranial direct current stimulation on reactive response inhibition. Neurosci Biobehav R 128: 749-65. https://doi.org/10.1016/j.neubiorev.2021.07.013
|
| [26] |
Lowe CJ, Vincent C, Hall PA (2017) Effects of Noninvasive Brain Stimulation on Food Cravings and Consumption: A Meta-Analytic Review. Psychosom Med 79: 2-13. https://doi.org/10.1097/PSY.0000000000000368
|
| [27] |
Mostafavi SA, Khaleghi A, Mohammadi MR, et al. (2020) Is transcranial direct current stimulation an effective modality in reducing food craving? A systematic review and meta-analysis. Nutr Neurosci 23: 55-67. https://doi.org/10.1080/1028415X.2018.1470371
|
| [28] | Orru G, Miniati M, Conversano C, et al. (2021) A machine learning analysis of psychopathological features of Eating Disorders: a retrospective study. Mediterr J Clin Psyc 9. Available from: https://cab.unime.it/journals/index.php/MJCP/article/view/2670 |
| [29] |
Meule A, Küppers C, Harms L, et al. (2018) Food cue-induced craving in individuals with bulimia nervosa and binge-eating disorder. PLOS ONE 13: e0204151. https://doi.org/10.1371/journal.pone.0204151
|
| [30] |
Moher D, Liberati A, Tetzlaff J, et al. (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339: b2535. https://doi.org/10.1136/bmj.b2535
|
| [31] |
da Costa Santos CM, de Mattos Pimenta CA, Nobre MRC (2007) The PICO strategy for the research question construction and evidence search. Rev Lat Am Enfermagem 15: 508-511. https://doi.org/10.1590/S0104-11692007000300023
|
| [32] | Mendeley - Reference Management Software [Internet]. [cited 2022 Jul 13]. Available from: https://www.mendeley.com/?interaction_required=true |
| [33] |
Jadad AR, Moore RA, Carroll D, et al. (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Control Clin Trials 17: 1-12. https://doi.org/10.1016/0197-2456(95)00134-4
|
| [34] |
Higgins JPT, Altman DG, Gøtzsche PC, et al. (2011) The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343: d5928. https://doi.org/10.1136/bmj.d5928
|
| [35] |
Grundeis F, Brand C, Kumar S, et al. (2017) Non-invasive Prefrontal/Frontal Brain Stimulation Is Not Effective in Modulating Food Reappraisal Abilities or Calorie Consumption in Obese Females. Front Neurosci 11: 334. https://doi.org/10.3389/fnins.2017.00334
|
| [36] |
Ray MK, Sylvester MD, Helton A, et al. (2019) The effect of expectation on transcranial direct current stimulation (tDCS) to suppress food craving and eating in individuals with overweight and obesity. Appetite 136: 1-7. https://doi.org/10.1016/j.appet.2018.12.044
|
| [37] |
Marron EM, Viejo-Sobera R, Cuatrecasas G, et al. (2019) Prefronto-cerebellar neuromodulation affects appetite in obesity. Int J Obes (Lond) 43: 2119-2124. https://doi.org/10.1038/s41366-018-0278-8
|
| [38] |
Gluck ME, Alonso-Alonso M, Piaggi P, et al. (2015) Neuromodulation targeted to the prefrontal cortex induces changes in energy intake and weight loss in obesity. Obesity 23: 2149-2156. https://doi.org/10.1002/oby.21313
|
| [39] |
Heinitz S, Reinhardt M, Piaggi P, et al. (2017) Neuromodulation directed at the prefrontal cortex of subjects with obesity reduces snack food intake and hunger in a randomized trial. Am J Clin Nutr 106: 1347-1357. https://doi.org/10.3945/ajcn.117.158089
|
| [40] | Lenhard W, Lenhard A Computation of Effect Sizes (2017). |
| [41] |
Wilson SJ, Sayette MA, Fiez JA (2004) Prefrontal responses to drug cues: a neurocognitive analysis. Nat Neurosci 7: 211-214. https://doi.org/10.1038/nn1200
|
| [42] |
Alonso-Alonso M, Pascual-Leone A (2007) The right brain hypothesis for obesity. JAMA 297: 1819-1822. https://doi.org/10.1001/jama.297.16.1819
|
| [43] | Legget KT, Wylie KP, Cornier MA, et al. (2020) Altered between-network connectivity in individuals prone to obesity. Physiol Behav 113242. https://doi.org/10.1016/j.physbeh.2020.113242 |
| [44] |
Son NT Le D, Pannacciulli N, Chen K, et al. (2007) Less activation in the left dorsolateral prefrontal cortex in the reanalysis of the response to a meal in obese than in lean women and its association with successful weight loss. Am J Clin Nutr 86: 573-579. https://doi.org/10.1093/ajcn/86.3.573
|
| [45] |
Wager TD, Atlas LY (2015) The neuroscience of placebo effects: connecting context, learning and health. Nat Rev Neurosci 16: 403-418. https://doi.org/10.1038/nrn3976
|
| [46] |
Benedetti F, Carlino E, Pollo A (2011) How Placebos Change the Patient's Brain. Neuropsychopharmacology 36: 339-354. https://doi.org/10.1038/npp.2010.81
|
| [47] |
Heekeren HR, Marrett S, Bandettini PA, et al. (2004) A general mechanism for perceptual decision-making in the human brain. Nature 431: 859-862. https://doi.org/10.1038/nature02966
|
| [48] |
Rolls ET, Critchley HD, Browning A, et al. (1998) The Neurophysiology of Taste and Olfaction in Primates, and Umami Flavora. Ann NY Acad Sci 855: 426-437. https://doi.org/10.1111/j.1749-6632.1998.tb10602.x
|
| [49] | Kumar S, Grundeis F, Brand C, et al. (2016) Differences in Insula and Pre-/Frontal Responses during Reappraisal of Food in Lean and Obese Humans. Front Hum Neurosci 10: 233. https://doi.org/10.3389/fnhum.2016.00233 |
| [50] | Berman BD, Horovitz SG, Hallett M (2013) Modulation of functionally localized right insular cortex activity using real-time fMRI-based neurofeedback. Front Hum Neurosci . https://doi.org/10.3389/fnhum.2013.00638 |
| [51] |
Noori HR, Cosa Linan A, Spanagel R (2016) Largely overlapping neuronal substrates of reactivity to drug, gambling, food and sexual cues: A comprehensive meta-analysis. Eur Neuropsychopharmacol 26: 1419-1430. https://doi.org/10.1016/j.euroneuro.2016.06.013
|
| [52] |
Bryant M, Truesdale KP, Dye L (2006) Modest changes in dietary intake across the menstrual cycle: implications for food intake research. Br J Nutr 96: 888-894. https://doi.org/10.1017/BJN20061931
|
| [53] |
Accornero N, Capozza M, Pieroni L, et al. (2014) EEG mean frequency changes in healthy subjects during prefrontal transcranial direct current stimulation. J Neurophysiol 112: 1367-1375. https://doi.org/10.1152/jn.00088.2014
|
| [54] |
Noetscher GM, Yanamadala J, Makarov SN, et al. (2014) Comparison of cephalic and extracephalic montages for transcranial direct current stimulation--a numerical study. IEEE Trans Biomed Eng 61: 2488-2498. https://doi.org/10.1109/TBME.2014.2322774
|
| [55] |
Misonou H, Mohapatra DP, Park EW, et al. (2004) Regulation of ion channel localization and phosphorylation by neuronal activity. Nat Neurosci 7: 711-718. https://doi.org/10.1038/nn1260
|
| [56] | Prehn K, Flöel A (2015) Potentials and limits to enhance cognitive functions in healthy and pathological aging by tDCS. Front Cell Neurosci . https://doi.org/10.3389/fncel.2015.00355 |
| [57] |
Lefaucheur JP, Antal A, Ayache SS, et al. (2017) Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin Neurophysiol 128: 56-92. https://doi.org/10.1016/j.clinph.2016.10.087
|
| [58] | Davis SE, Smith GA (2019) Transcranial Direct Current Stimulation Use in Warfighting: Benefits, Risks, and Future Prospects. Front Hum Neurosci . https://doi.org/10.3389/fnhum.2019.00114 |
| [59] |
Chang CC, Kao YC, Chao CY, et al. (2020) The Effects of Bi-Anodal tDCS Over the Prefrontal Cortex Regions With Extracephalic Reference Placement on Insight Levels and Cardio-Respiratory and Autonomic Functions in Schizophrenia Patients and Exploratory Biomarker Analyses for Treatment Response. Int J Neuropsychopharmacol 24: 40-53. https://doi.org/10.1093/ijnp/pyaa063
|
| [60] |
Saxena V, Pal A (2021) Role of Transcranial Direct Current Stimulation in the Management of Alzheimer's Disease: A Meta-analysis of Effects, Adherence and Adverse Effects. Clin Psychopharmacol Neurosci 19: 589-599. https://doi.org/10.9758/cpn.2021.19.4.589
|
 neurosci-09-03-020-s001.pdf neurosci-09-03-020-s001.pdf |
 |
Figures(1) / Tables(2)

Graziella Orrù, Valentina Cesari, Eleonora Malloggi, Ciro Conversano, Danilo Menicucci, Alessandro Rotondo, Cristina Scarpazza, Laura Marchi, Angelo Gemignani. The effects of Transcranial Direct Current Stimulation on food craving and food intake in individuals affected by obesity and overweight: a mini review of the magnitude of the effects[J]. AIMS Neuroscience, 2022, 9(3): 358-372. doi: 10.3934/Neuroscience.2022020







 DownLoad:
DownLoad: