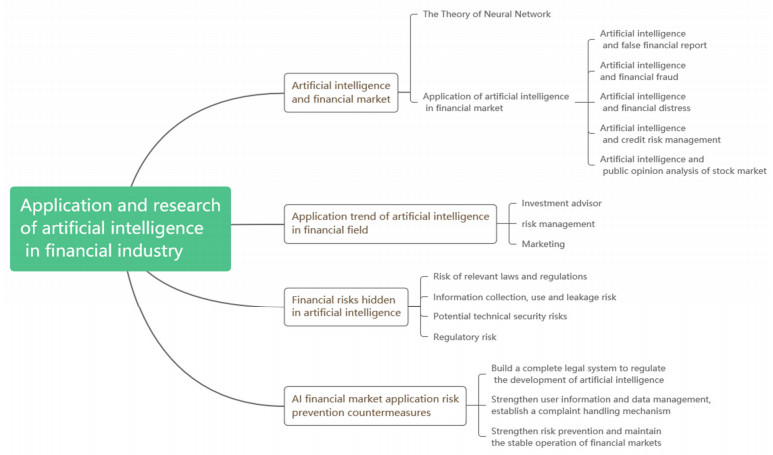
Artificial Intelligence (AI) is deemed to be the commanding point of science and technology in the next era. In recent years, with the enhancement of computer computing power, the improvement of the quantity and quality of big data, and the important breakthroughs in many research fields such as machine learning and speech recognition, AI technology has developed rapidly and has been widely used in all walks of life. In the financial industry, the application of AI technology in risk control, marketing, customer service, transaction, operation, and product optimization of financial institutions is becoming increasingly mature, and some new business models have been created. Starting from the application status and significance of AI in the international financial field, this paper expounds on the application, status quo, and development trend of AI in the financial industry. Then, in view of the risks and practical challenges existing in the development process of AI, based on the reality of international financial development, this paper summarizes the measures to promote the in-depth, healthy, and sustainable development of AI in the financial market. This paper aims to let readers understand the development status of AI in the financial field, and also provide theoretical reference for scholars in this field.
Citation: Yuxin Li, Jizheng Yi, Huanyu Chen, Duanxiang Peng. Theory and application of artificial intelligence in financial industry[J]. Data Science in Finance and Economics, 2021, 1(2): 96-116. doi: 10.3934/DSFE.2021006
Artificial Intelligence (AI) is deemed to be the commanding point of science and technology in the next era. In recent years, with the enhancement of computer computing power, the improvement of the quantity and quality of big data, and the important breakthroughs in many research fields such as machine learning and speech recognition, AI technology has developed rapidly and has been widely used in all walks of life. In the financial industry, the application of AI technology in risk control, marketing, customer service, transaction, operation, and product optimization of financial institutions is becoming increasingly mature, and some new business models have been created. Starting from the application status and significance of AI in the international financial field, this paper expounds on the application, status quo, and development trend of AI in the financial industry. Then, in view of the risks and practical challenges existing in the development process of AI, based on the reality of international financial development, this paper summarizes the measures to promote the in-depth, healthy, and sustainable development of AI in the financial market. This paper aims to let readers understand the development status of AI in the financial field, and also provide theoretical reference for scholars in this field.

| [1] | Abbadi IM, Alawneh M (2008) Preventing insider information leakage for enterprises. 2008 Second International Conference on Emerging Security Information, Systems and Technologies, 99–106. |
| [2] |
Abellán J, Castellano JG (2017) A comparative study on base classifiers in ensemble methods for credit scoring. Expert Syst Appl 73: 1–10. doi: 10.1016/j.eswa.2016.12.020

|
| [3] |
Albashrawi M (2021) Detecting financial fraud using data mining techniques: A decade review from 2004 to 2015. J Data Sci 14: 553–570. doi: 10.6339/JDS.201607_14(3).0010
|
| [4] | Anthony M, Bartlett P (1999) Neural Network Learning-Theoretical Foundations. |
| [5] | Khedr AE, Salama SE, Yaseen N (2017) Predicting stock market behavior using data mining technique and news sentiment analysis. Int J Intell Syst Appl 9: 22–30. |
| [6] |
Bahnsen AC, Aouada D, Stojanovic A (2016) Feature engineering strategies for credit card fraud detection. Expert Syst Appl 51: 134–142. doi: 10.1016/j.eswa.2015.12.030
|
| [7] | Bahnsen AC, Stojanovic A, Aouada D, et al. (2013) Cost sensitive credit card fraud detection using bayes minimum risk. 2013 12th International Conference on Machine Learning and Applications. |
| [8] | Bhingarde A, Bangar A, Gupta K, et al. (2015) Credit card fraud detection using hidden markov model. Int J Comput Sci Inform Technol 76: 169–170. |
| [9] | Brummer C (2010) How International Financial Law Works (and How it Doesn't). |
| [10] | Cerullo MJ, Cerullo V (1999) Using neural networks to predict financial reporting fraud: part 2. Comput Fraud Secur 1999: 14–17. |
| [11] |
Chen WS, Du YK (2009) Using neural networks and data mining techniques for the financial distress prediction model. Expert Syst Appl 36: 4075–4086. doi: 10.1016/j.eswa.2008.03.020
|
| [12] | Cheng DL (2016) Application status and security risk analysis of artificial intelligence in financial field. Financ Technol Era 2016: 47–49. |
| [13] | Cheng J, He J, Yuan H, et al. (2017) Financial technology risks and regulatory countermeasures. China Financ 2017. |
| [14] | Chu AB (2018) Mobile Technology and financial inclusion. In: Handbook of Blockchain, Digital Finance, and Inclusion, 1 Eds., Cambridge: Academic Press, 131–44. |
| [15] |
Du Jardin P (2010) Predicting bankruptcy using neural networks and other classification methods: The influence of variable selection techniques on model accuracy. Neurocomputing 73: 2047–2060. doi: 10.1016/j.neucom.2009.11.034
|
| [16] | Fu K, Cheng D, Tu Y, et al. (2016) Credit card fraud detection using convolutional neural networks. International Conference on Neural Information Processing, 483–490. |
| [17] | Gutierrez FH, Levin SC, Chambers MA, et al. (2015) FinCEN proposes AML requirements for registered investment advisers. Bank Financ Serv Policy Rep 34:15–18. |
| [18] | Ibrahim A (2004) Chapter 6-Neural networks. |
| [19] | IDC (2016) Worldwide Semiannual Cognitive/Artificial Intelligence Systems Spending Guide. |
| [20] | Jiang HY, Wu CF (2016) Development status and regulatory suggestions of intelligent investment consultant. Secur Mark Guide. |
| [21] | Kaminski KA, Wetzel TS, Guan L (2004) Can financial ratios detect fraudulent financial reporting? Managerial Auditing J 19: 15–28. |
| [22] |
Khandani AE, Kim AJ, Lo AW (2010) Consumer credit-risk models via machine-learning algorithms. J Bank Financ 34: 2767–2787. doi: 10.1016/j.jbankfin.2010.06.001
|
| [23] |
Khashman A (2011) Credit risk evaluation using neural networks: Emotional versus conventional models. Appl Soft Comput 11: 5477–5484. doi: 10.1016/j.asoc.2011.05.011
|
| [24] | Killeen A, Chan R (2018) Global financial institutions 2.0, In: Handbook of Blockchain, Digital Finance, and Inclusion, 2 Eds., Amsterdam: Elsevier Inc, 213–242. |
| [25] | Kim D, Kwahk K (2013) Investigating the global financial markets from a social network analysis perspective. J Korean Oper Res Manage Sci Soc 38: 11–33. |
| [26] | Kim J (2018) Tasks and current status of the uses of artificial intelligence (fintech ai) in the fintech industry in the USA. J Payment Settlement 10: 185–214. |
| [27] | Korinek A, Stiglitz JE (2017) Artificial intelligence and its implications for income distribution and unemployment. Natl Bur Econ Res. |
| [28] |
Koskivaara E (2004) Artificial neural networks in analytical review procedures. Manage Auditing J 19: 191–223. doi: 10.1108/02686900410517821
|
| [29] | Kotsiantis S, Koumanakos E, Tzelepis D, et al. (2006) Forecasting fraudulent financial statements using data mining. Int J Comput Int 3: 104–110. |
| [30] |
Kumar V, Rajan B, Venkatesan R, et al. (2019) Understanding the role of artificial intelligence in personalized engagement marketing. Calif Manage Rev 61: 135–155. doi: 10.1177/0008125619859317
|
| [31] | Küükkocaolu G, Benli Y, Küçüksözen C (1997) Detecting the manipulation of financial information by using artificial neural network models. Istanbul Stock Exc Rev 9. |
| [32] |
Lessmann S, Baesens B, Seow HV, et al. (2015) Benchmarking state-of-the-art classification algorithms for credit scoring: An update of research. Eur J Oper Res 247: 124–136. doi: 10.1016/j.ejor.2015.05.030
|
| [33] | Li JZ (2012) Improving the management structure of consumer protection in banking institutions-Also commenting on the notice of China Banking Regulatory Commission on improving the customer complaint handling mechanism of banking financial institutions and doing a good job in financial consumer protection. Banker, 116–119. |
| [34] |
Lin C, Chiu A, Huang SY, et al. (2015) Detecting the financial statement fraud: The analysis of the differences between data mining techniques and experts' judgments. Knowl Based Syst 89: 459–470. doi: 10.1016/j.knosys.2015.08.011
|
| [35] | Ma SL, Wei FY (2018) Application of artificial intelligence technology in financial field: main difficulties and countermeasures. South Financ, 78–84. |
| [36] | Marcus C, Huang Z (2019) Artificial intelligence attacks: Artificial intelligence security vulnerabilities and countermeasures. Inform Secur Commun Secrecy, 72–81. |
| [37] |
Mashrur A, Luo W, Zaidi NA, et al. (2020) Machine learning for financial risk management: A survey. IEEE Access 8: 203203–203223. doi: 10.1109/ACCESS.2020.3036322
|
| [38] | McCauley D (2016) Ghosts in the Machine: Artificial Intelligence, Risks and Regulation in Financial Markets. London Thought Leadership Consulting. Available from: https://www.euromoneythoughtleadership.com/ghostsinthemachine/. |
| [39] |
Mustafa M, Rahman M (2015) Financial inclusion and per capita real GSP growth across fifty US states and the district of Columbia: Evidence from panel cointegration and GMM estimates. Glob Bus Financ Rev 20: 87–94. doi: 10.17549/gbfr.2015.20.1.87
|
| [40] | Pacelli V (2011) An artificial neural network approach for credit risk management. J Intell Learn Syst Appl 3: 103–112. |
| [41] | Patel CI, Labana D, Pandya S, et al. (2020) Histogram of oriented gradient-based fusion of features for human action recognition in action video sequences. Sensors 20: 7299. |
| [42] |
Patel J, Shah S, Thakkar P, et al. (2015) Predecting stock and stock price index movement using trend deterministic data preparation and machine learning techniques. Expert Syst Appl 42: 2162–2172. doi: 10.1016/j.eswa.2014.10.031
|
| [43] | Ponemon L, Julian T, Lalan C (2016) IBM & Ponemon Institute Study: Data Breach Costs Rising, Now $4 million per Incident. |
| [44] |
Sahin Y, Bulkan S, Duman E (2013) A cost-sensitive decision tree approach for fraud detection. Expert Syst Appl 40: 5916–5923. doi: 10.1016/j.eswa.2013.05.021
|
| [45] | Schwab K (2017) Science and technology policy institute forum, In: The Fourth Industrial Revolution, 26 Eds., Geneva: Crown Publishing Group, 12–15. |
| [46] | Sureshkumar K, Elango N (2012) Performance analysis of stock price prediction using artificial neural network. Glob J Comput Sci Technol 12. |
| [47] | Swicegood P, Clark JA (2001) Off-site monitoring systems for predicting bank underperformance: a comparison of neural networks, discriminant analysis, and professional human judgment, intelligent. Syst Account Financ Manage 10: 169–186. |
| [48] | Timoshenko A, Hauser JR (2019) Identifying customer needs from user-generated content. Mark Sci 38. |
| [49] | Tractica (2015) Artificial Intelligence for Enterprise Applications: Deep Learning, Predictive Computing, Image Recognition, Speech Recognition, and Other AI Technologies for Enterprise Markets-Global Market Analysis and Forecasts. Available from: https://tractica.omdia.com/wp-content/uploads/2015/04/AIE-15-Brochure.pdf. |
| [50] |
Tsai CF, Wu JW (2008) Using neural network ensembles for bankruptcy prediction and credit scoring. Expert Syst Appl 34: 2639–2649. doi: 10.1016/j.eswa.2007.05.019
|
| [51] |
Tu JV (1996) Advantages and disadvantages of using artificial neural networks versus logistic regression for predicting medical outcomes. J Clin Epidemiol 49: 1225–1231. doi: 10.1016/S0895-4356(96)00002-9
|
| [52] | Wang D (2017) Traditional financial institutions are ready to move. Is it more advantageous to set foot in intelligent investment advisory. China's Strategic Emerg Ind, 70–72. |
| [53] |
Wong BK, Lai VS, Lam J (2000) A bibliography of neural network business applications research: 1994–1998. Comput Oper Res 27: 1045–1076. doi: 10.1016/S0305-0548(99)00142-2
|
| [54] | Wu HD (2017) Institutional arrangement and legal regulation in the age of artificial intelligence. Legal Sci, 128–136. |
| [55] | Wu J, Chen L, Gao Y (2016) The application of foreign artificial intelligence in the field of financial investment advisory and its enlightenment to my country. Financ Asp, 88–92. |
| [56] | Wu C, Wu F, Liu J, et al. (2019) Neural demographic prediction using search query. Proceedings of the Twelfth ACM International Conference on Web Search and Data Mining. |
| [57] | Alvarez Y, Leguizamón-Páez MA, Londoño TJ (2020) Risks and security solutions existing in the Internet of things (IoT) in relation to Big Data. Ing Compet 23: 9–10. |
| [58] | Yu M (2019) Research on the current situation and development trend of marketing industry under the background of artificial intelligence. Wealth Life, 82–83. |
| [59] | Yu XJ, Peng YY (2017) Application and challenge of artificial intelligence in financial risk management. South Financ. |
| [60] |
Yu L, Yue W, Wang S, et al. (2010) Support vector machine based multiagent ensemble learning for credit risk evaluation. Expert Syst Appl 37: 1351–1360. doi: 10.1016/j.eswa.2009.06.083
|
Figures(5)
Yuxin Li, Jizheng Yi, Huanyu Chen, Duanxiang Peng. Theory and application of artificial intelligence in financial industry[J]. Data Science in Finance and Economics, 2021, 1(2): 96-116. doi: 10.3934/DSFE.2021006







 DownLoad:
DownLoad: