Citation: Hassan Ali Khan, Wu Jue, Muhammad Mushtaq, Muhammad Umer Mushtaq. Brain tumor classification in MRI image using convolutional neural network[J]. Mathematical Biosciences and Engineering, 2020, 17(5): 6203-6216. doi: 10.3934/mbe.2020328

| [1] | NBTS, National Brain Tumor Society: Quick brain tumor facts, 2020. Available from: https://braintumor.org/brain-tumor-information/brain-tumor-facts/. |
| [2] | Cancer. Net, Brain Tumor: Staticstics, 2020. Available from: https://www.cancer.net/cancertypes/brain-tumor/statistics. |
| [3] | NHS, National Health Service: Brain Tumours, 2020. Available from: https://www.nhs.uk/conditions/brain-tumours/. |
| [4] | S. Basheera, M. S. S. Ram, Classification of brain tumors using deep features extracted using CNN, J. Phys., 1172 (2019), 012016. |
| [5] | M. Sajjad, S. Khan, M. Khan, W. Wu, A. Ullah, S. W. Baik, Multi-grade brain tumor classification using deep CNN with extensive data augmentation, J. Comput. Sci., 30 (2019), 174-182. |
| [6] | R. Carlo, C. Renato, C. Giuseppe, U. Lorenzo, I. Giovanni, S. Domenico, Distinguishing Functional from Non-functional Pituitary Macroadenomas with a Machine Learning Analysis, Mediterranean Conference on Medical and Biological Engineering and Computing, Springer, 2019, 1822-1829. |
| [7] | S. Khawaldeh, U. Pervaiz, A. Rafiq, R. Alkhawaldeh, Noninvasive grading of glioma tumor using magnetic resonance imaging with convolutional neural networks, J. Appl. Sci., 8 (2018), 27. |
| [8] | N. Abiwinanda, M. Hanif, S. Hesaputra, A. Handayani, T. R. Mengko, Brain tumor classification using convolutional neural network, World Congress on Medical Physics and Biomedical Engineering, Springer, Singapore, 2019. |
| [9] | S. Das, R. Aranya, N. Labiba, Brain tumor classification using convolutional neural network, 2019 1st International Conference on Advances in Science, Engineering and Robotics Technology (ICASERT), 2019. |
| [10] | V. Romeo, R. Cuocolo, C. Ricciardi, L. Ugga, S. Cocozza, F. Verde, et al., Prediction of tumor grade and nodal status in oropharyngeal and oral cavity squamous-cell carcinoma using a radiomic approach, Anticancer Res., 40 (2020), 271-280. |
| [11] | M. Talo, U. B. Baloglu, O. Yldrm, U. R. Acharya, Application of deep transfer learning for automated brain abnormality classification using MRI images, Cognitive Systems Research, 54 (2019), 176-188. |
| [12] | A. Rehman, S. Naz, M. I. Razzak, F. Akram, M. Imran, A Deep Learning-Based Framework for Automatic Brain Tumors Classification Using Transfer Learning, Circuits Syst. Signal Process., 39 (2020), 757-775. |
| [13] | A. Cinar, M. Yldrm, Detection of tumors on brain MRI images using the hybrid convolutional neural network architecture, Med. Hypotheses, 139 (2020), 109684. |
| [14] | N. Chakrabarty, Brain MRI images dataset for brain tumor detection, Kaggle, 2019. Available from: https://www.kaggle.com/navoneel/brain-mri-images-for-brain-tumor-detection. |
| [15] | J. F. Canny, Canny Edge Detection, Open Source Computer Vision, OpenCV. Available from: https://docs.opencv.org/trunk/da/d22/tutorial_py_canny.html. |
| [16] | C. Shorten, T. M. Khoshgoftaa, A survey on image data augmentation for deep learning, J. Big Data, 6 (2019), 60. |
| [17] | Keras, Image data preprocessing keras API, Keras documentation. Available from: https://keras.io/api/preprocessing/image/. |
| [18] | V. Nair, G. Hinton, Rectified linear units improve restricted boltzmann machines, ICML, 2010. |
| [19] | S. Mannor, D. Peleg, R. Rubinstein, The cross entropy method for classification, Proceedings of the 22nd international conference on Machine learning, 2005. |
| [20] | D. P. Kingma, J. Ba, A method for stochastic optimization, arXiv: 1412.6980. |
| [21] | H. Robbins, S. Munro, A Stochastic Approximation Method, Ann. Math. Stat., 22 (1951), 400-407. |
| [22] | G. Hinton, Neural networks for machine learning online course lecture 6a, Coursera. Available from: http://www.cs.toronto.edu/tijmen/csc321/slides/lecture_slides_lec6.pdf. |
| [23] | S. J. Pan, Q. Yang, A survey on transfer learning, IEEE Trans. Knowl. Data Eng., 22 (2010), 1345-1359. |
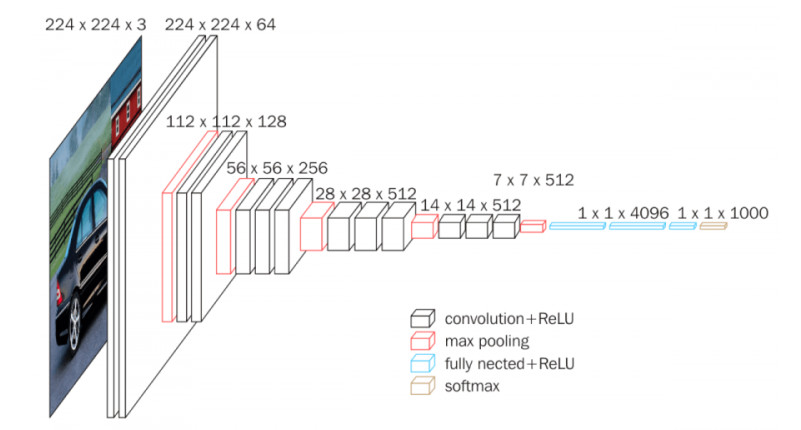
| [24] | K. Simonyan, A. Zisserman, Very deep convolutional networks for large-scale image recognition, arXiv: 1409.1556. |
| [25] | C. Szegedy, W. Liu, Y. Jia, P. Sermanet, S. Reed, D. Anguelov, et al., Going deeper with convolutions, Proceedings of the IEEE conference on computer vision and pattern recognition, 2015. |
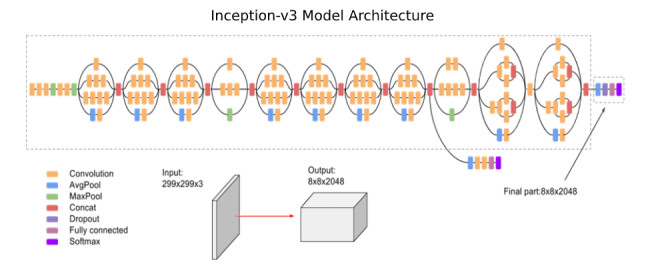
| [26] | C. Szegedy, V. Vanhoucke, S. Ioffe, J. Shlens, Z. Wojna, Rethinking the inception architecture for computer vision, Proceedings of the IEEE conference on computer vision and pattern recognition, 2016. |
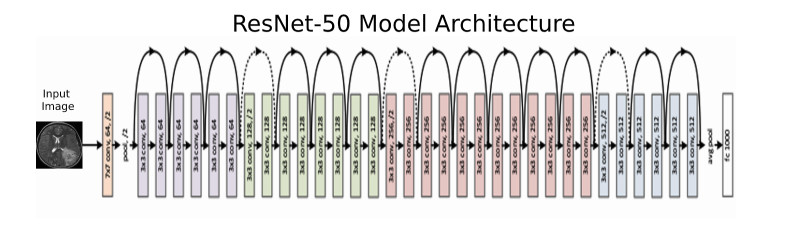
| [27] | K. He, X. Zhang, S. Ren, J. Sun, Deep residual learning for image recognition, Proceedings of the IEEE conference on computer vision and pattern recognition, 2016. |
Figures(9) / Tables(2)

Hassan Ali Khan, Wu Jue, Muhammad Mushtaq, Muhammad Umer Mushtaq. Brain tumor classification in MRI image using convolutional neural network[J]. Mathematical Biosciences and Engineering, 2020, 17(5): 6203-6216. doi: 10.3934/mbe.2020328







 DownLoad:
DownLoad: